
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-111
The Strategy of a Challenging Case of Chronic Total Occlusion With Deep Calcified In-Stent Restenosis
By Chun-Yen Chiang
Presenter
Chun-Yen Chiang
Authors
Chun-Yen Chiang1
Affiliation
Chi-Mei Medical Center, Taiwan1,
View Study Report
TCTAP C-111
Coronary - Complex PCI - In-Stent Restenosis
The Strategy of a Challenging Case of Chronic Total Occlusion With Deep Calcified In-Stent Restenosis
Chun-Yen Chiang1
Chi-Mei Medical Center, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
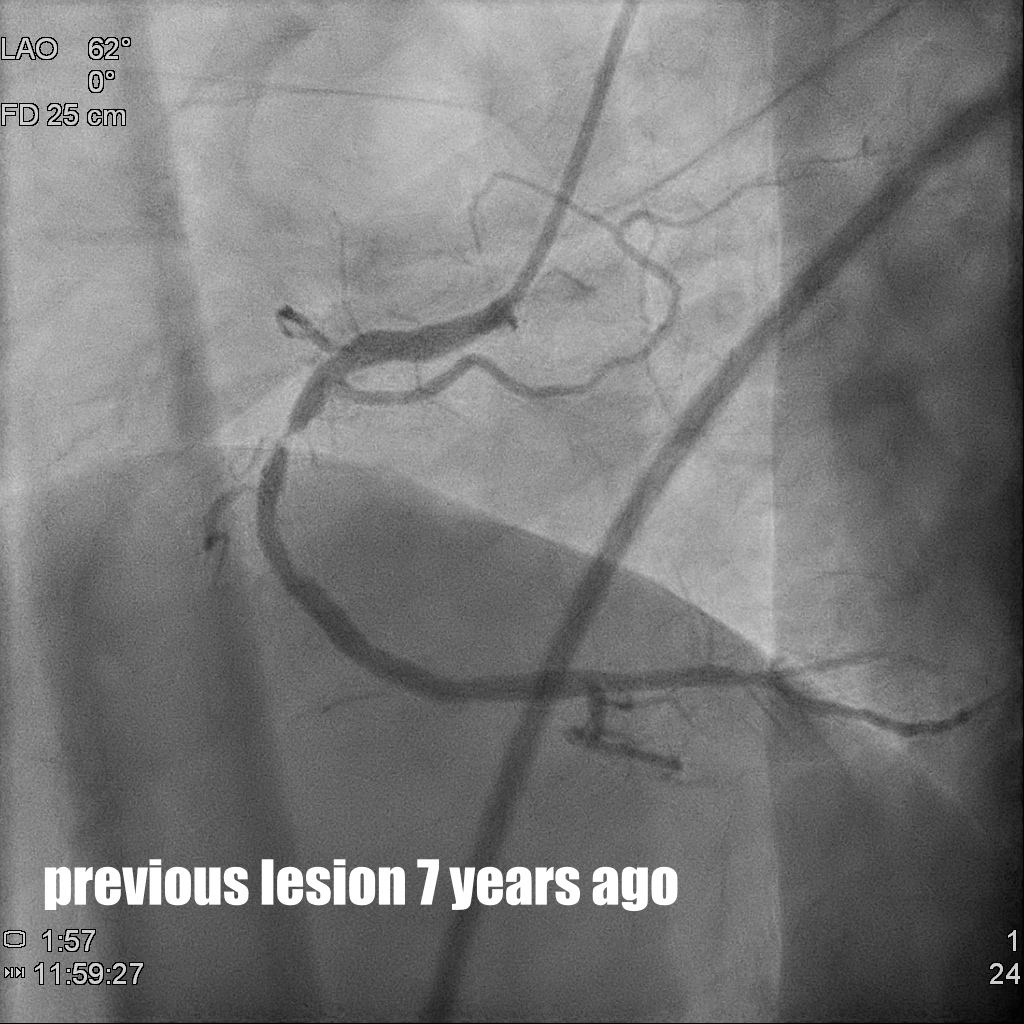
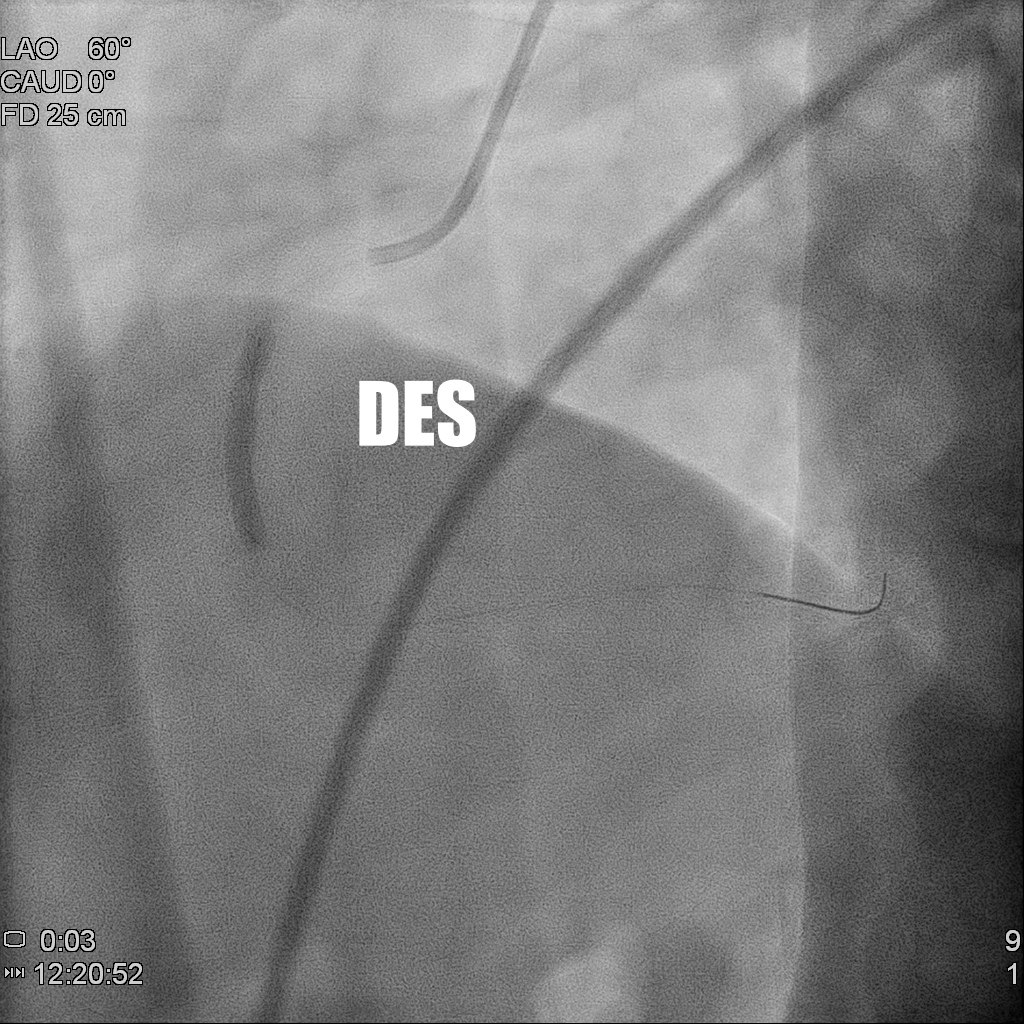
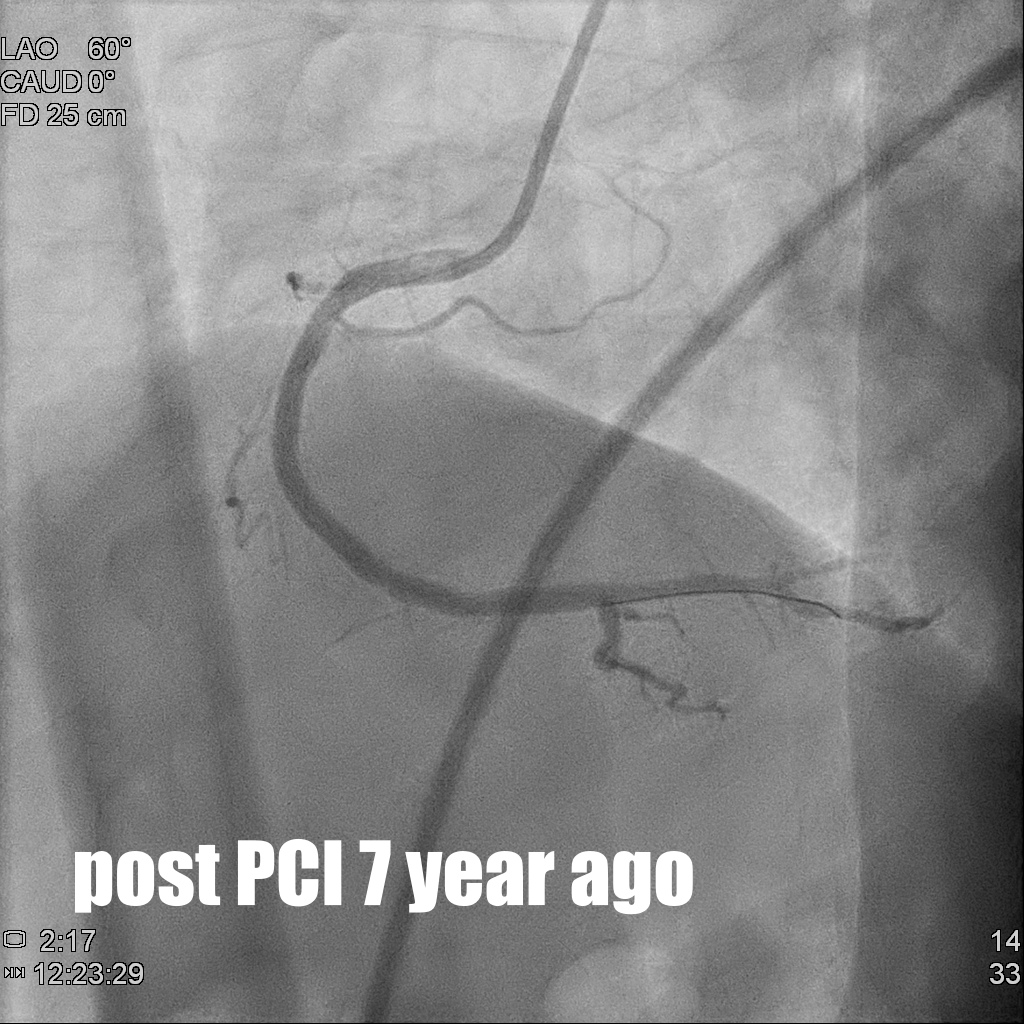
The 71 years-old male has the history of Non-ST-elevation myocardial infarction with coronary artery disease/three-vessel-disease 7 years ago and received percutaneouscoronary intervention for right coronary artery Middle part (Fig 1-1) by drug-eluting stent of Oynx 3.5x22mm 7 years ago (Fig 1-2, 1-3). He had chronic renal failure on peritoneal 5 years ago. He suffered from crescendo angina for a couples of days and his physical examination showed systolic murmur grade III over aortic area.
Relevant Test Results Prior to Catheterization
The thallium scan showed large extent of stress-inducedmyocardial ischemia of inferior wall and echocardiogram showed adequate LVsystolic performance and moderate calcified aortic stenosis.
Relevant Catheterization Findings
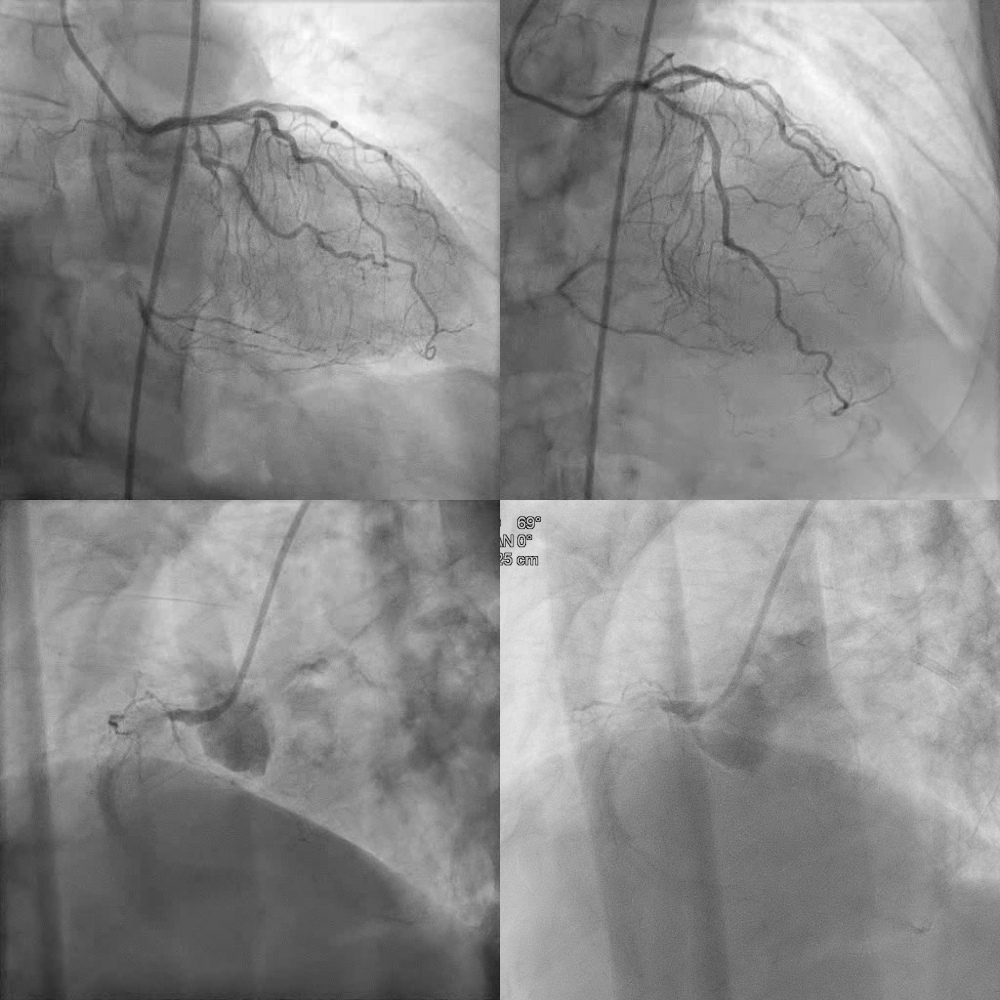
The cardiac catheterization of the patient showed coronary artery disease with triple vessel disease and chronic total occlusion of right coronary artery with in-stent total occlusion and collateral circulation from Left anterior descending artery and left circumflex to right coronary artery with diffuse long calcification of right coronary artery.
Interventional Management
Procedural Step
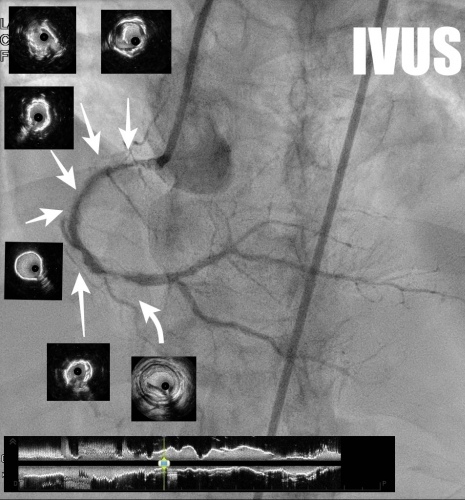
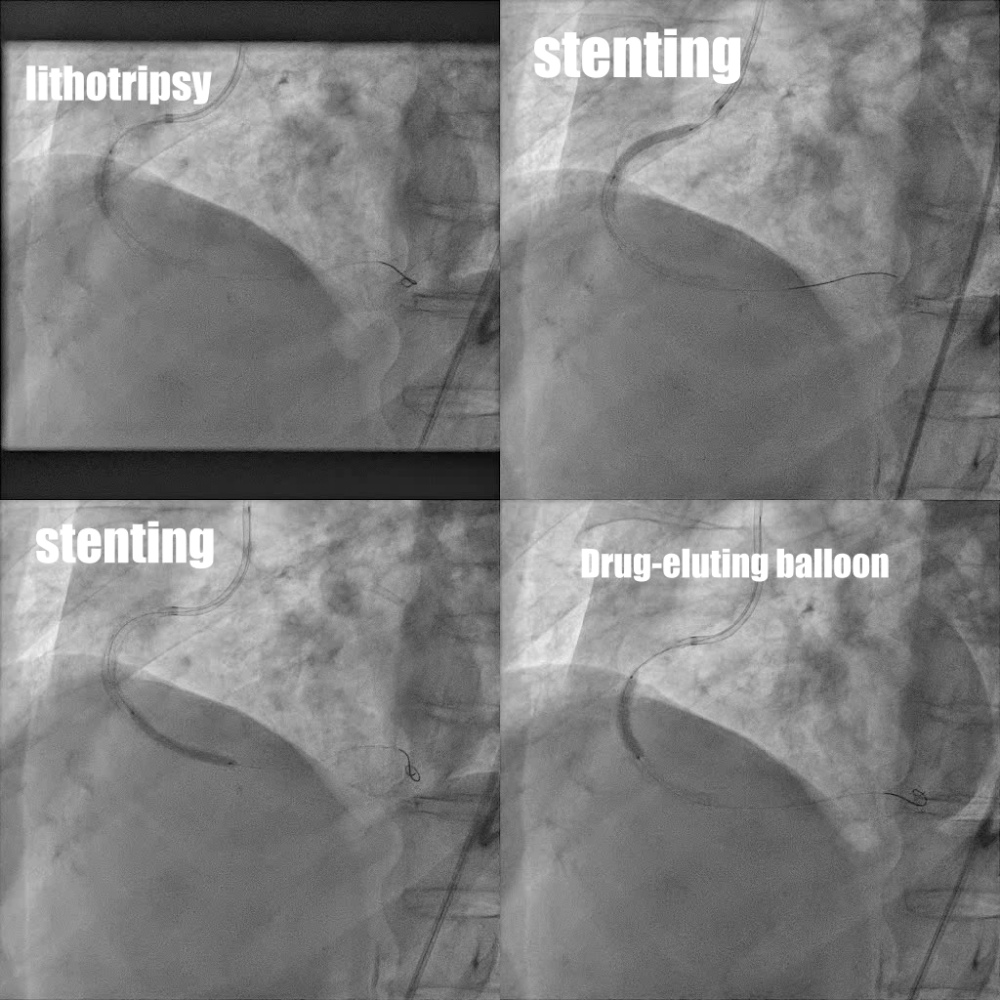
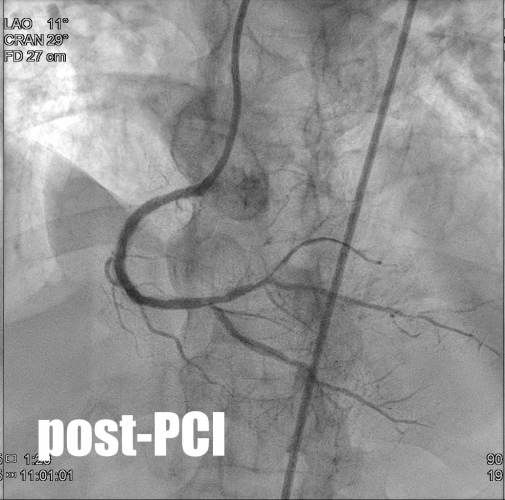
1. Under guiding catheter of AL1 Side hole, 7Fr via right femoral artery approach, we performed antegrade approach for chronic total occlusion of right coronary artery with guidewires escalation and microcatheter of Corsair Pro (2.6 French ; 135 cm) for chronic total occlusion of right coronary artery and then succeed to cross over it. However, there was NC balloon rupture with incomplete inflation of cutting-balloon of Wolverine 2.25x10mm for severe calcification in-stent restenosis of right coronary artery middle part and right coronary artery distal part. 2. Then we put intravenous ultrasound to right coronary artery distal part under the APT expressman guiding extension catheter and showed deep calcified in-stent restenosis of right coronary artery middle part and high calcium score and stenosis of right coronary artery distal part (Fig 3.1 )3. Then we performed lithotripsy ( 3.5x12mm) for deep calcified in-stent restenosis of right coronary artery middle part for total 80 pulses and there were cracks at right coronary artery middle part post lithotripsy. Then we used drug-coated balloon of Sequent Neo (3.5x25mm) for in-stent restenosis of right coronary artery middle part. (Fig 3.2 )4. Then we put two drug-eluting stents of Orsiro Mission ( 3.5x26mm ) to right coronary artery proximal part and Orisiro Mission (3.0x30mm) at right coronary artery distal part.(Fig 3.2) 5. The final coronary angiogram of right coronary artery showed TIMI III flow without restenosis. (Fig 3.3 )
Case Summary
Regarding chronic total occlusion of right coronary artery with deep calcified in-stent restenosis of the patient, percutaneous coronary intervention by lithotripsy with drug-coated balloon was performed to reduce the risk of double stents with in-stent restenosis.