
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-228
Comprehensive Approaches for SFA, ATA, and PTA CTOs in a Patient
By Szuchi Chien
Presenter
SZUCHI CHIEN
Authors
Szuchi Chien1
Affiliation
Changhua Christian Hospital, Taiwan1,
View Study Report
TCTAP C-228
Endovascular - Iliac / SFA Intervention
Comprehensive Approaches for SFA, ATA, and PTA CTOs in a Patient
Szuchi Chien1
Changhua Christian Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 63-year-old male with a history of hypertension and poorly controlled diabetes mellitus (HbA1c: 8.1) presented with intermittent claudication after walking 200 to 300 meters over the past six months, which consistently improved with rest. Based on clinical assessment, the patient was classified as Rutherford category 3.
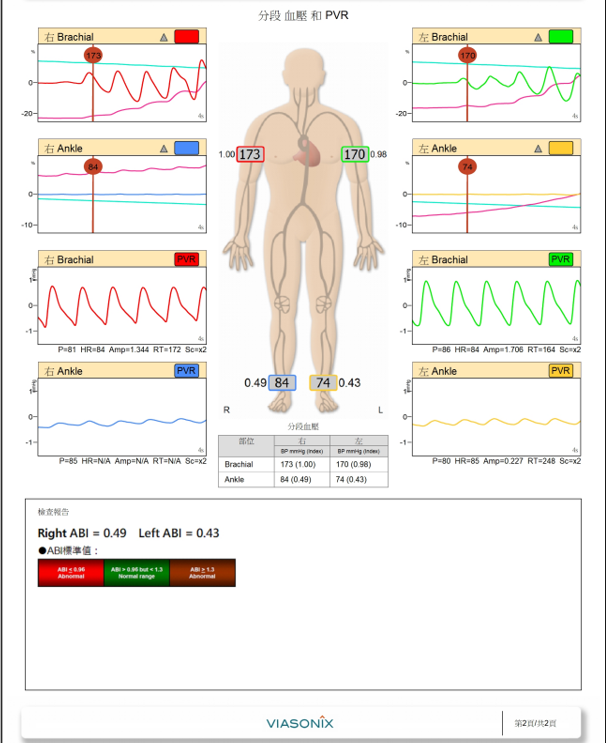
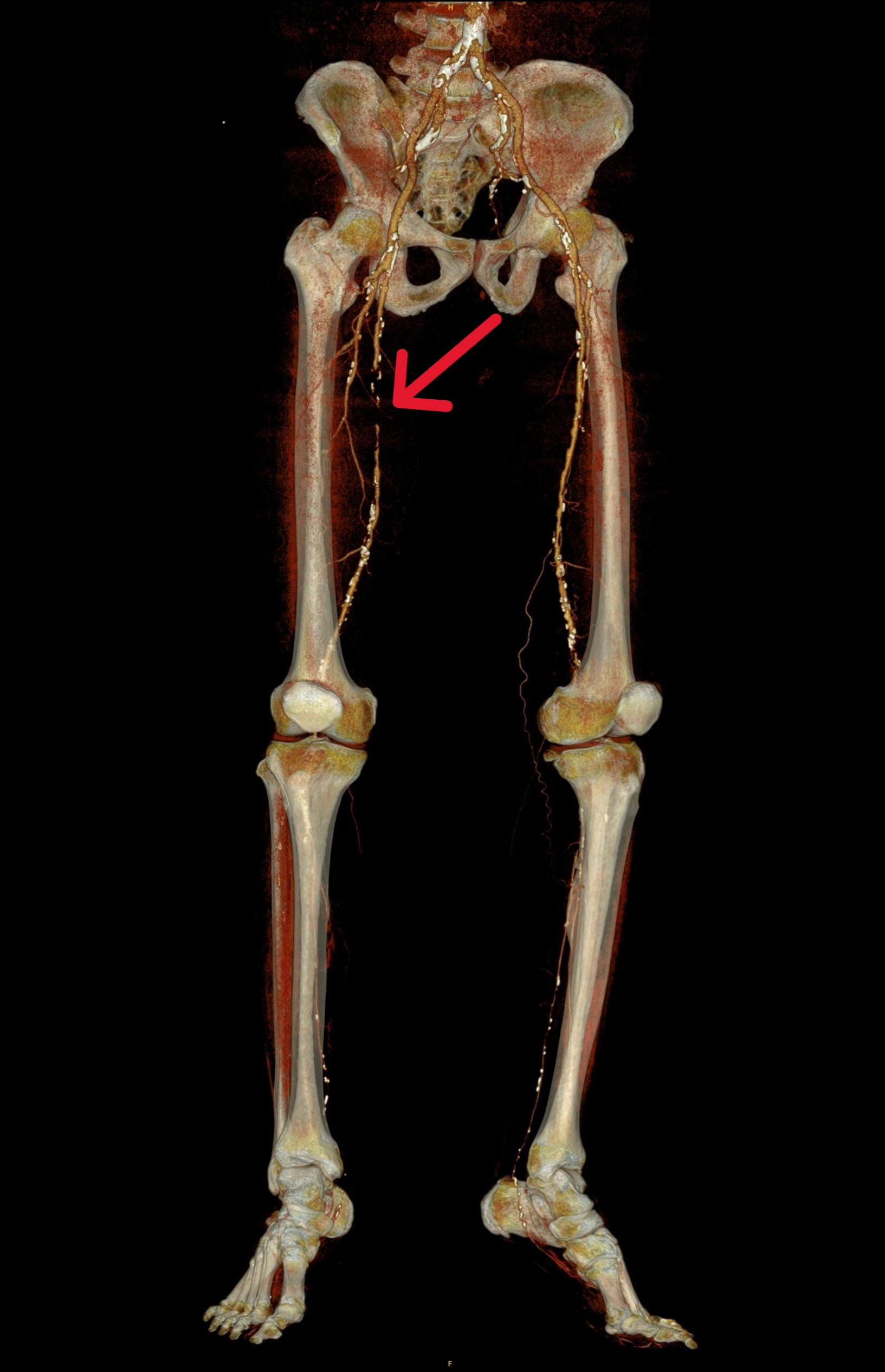

Relevant Test Results Prior to Catheterization
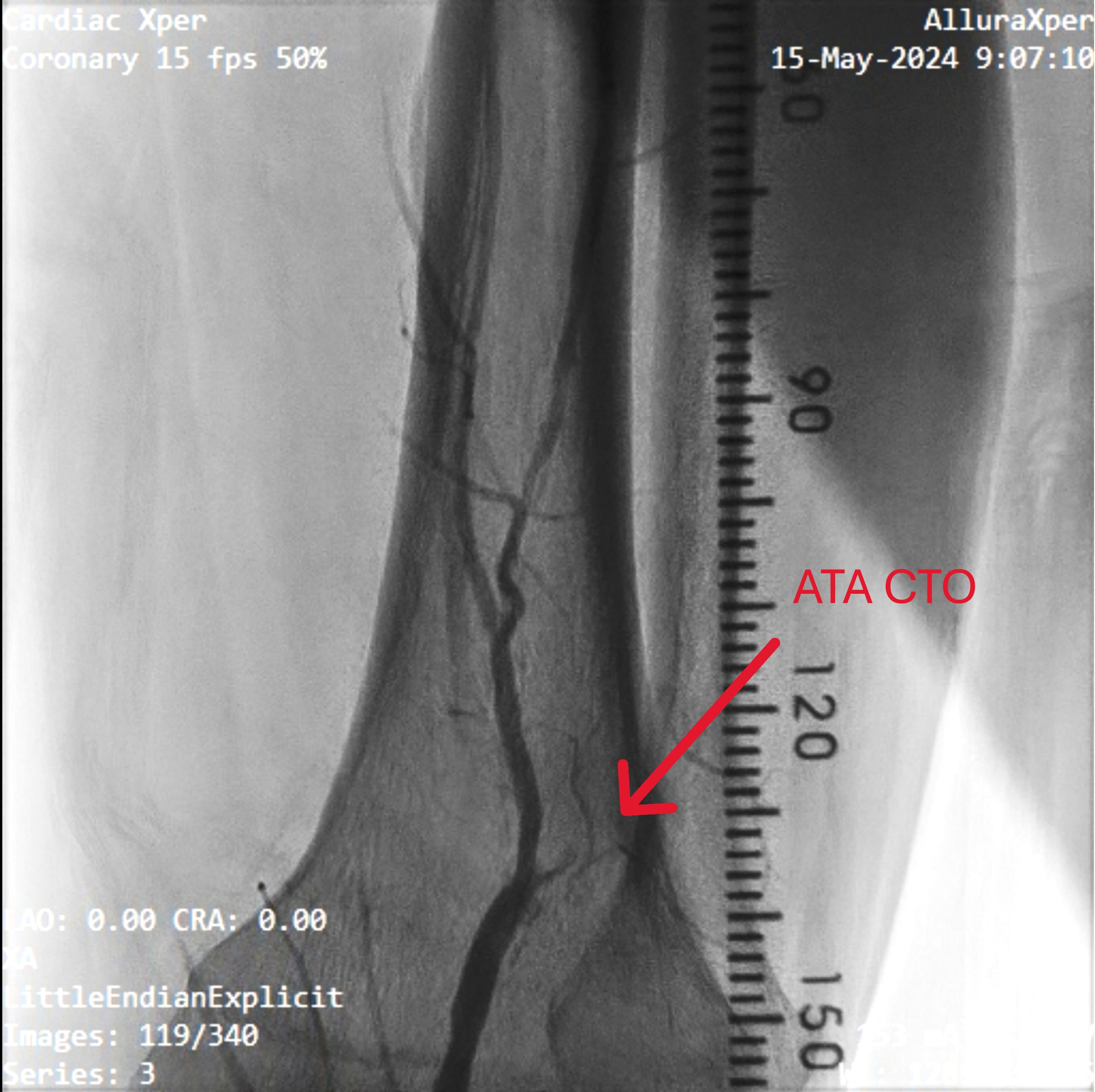
Right ABI is only 0.49, CTA showed SFA total occlusion, ATA proximal total occlusion and dsital PTA total occlusion.
Relevant Catheterization Findings
CTA showed SFA total occlusion, ATA proximal total occlusion and dsital PTA total occlusion.
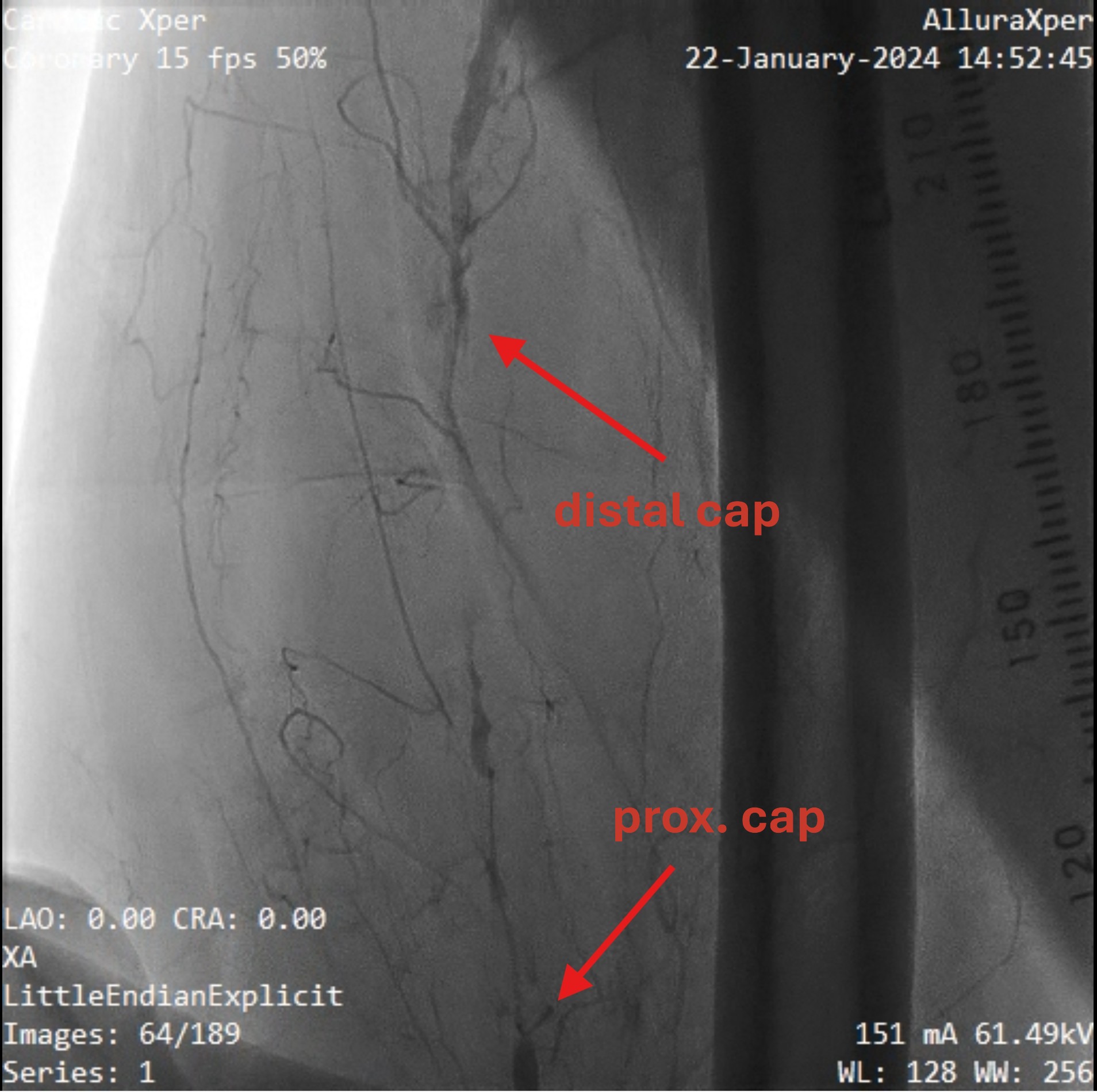
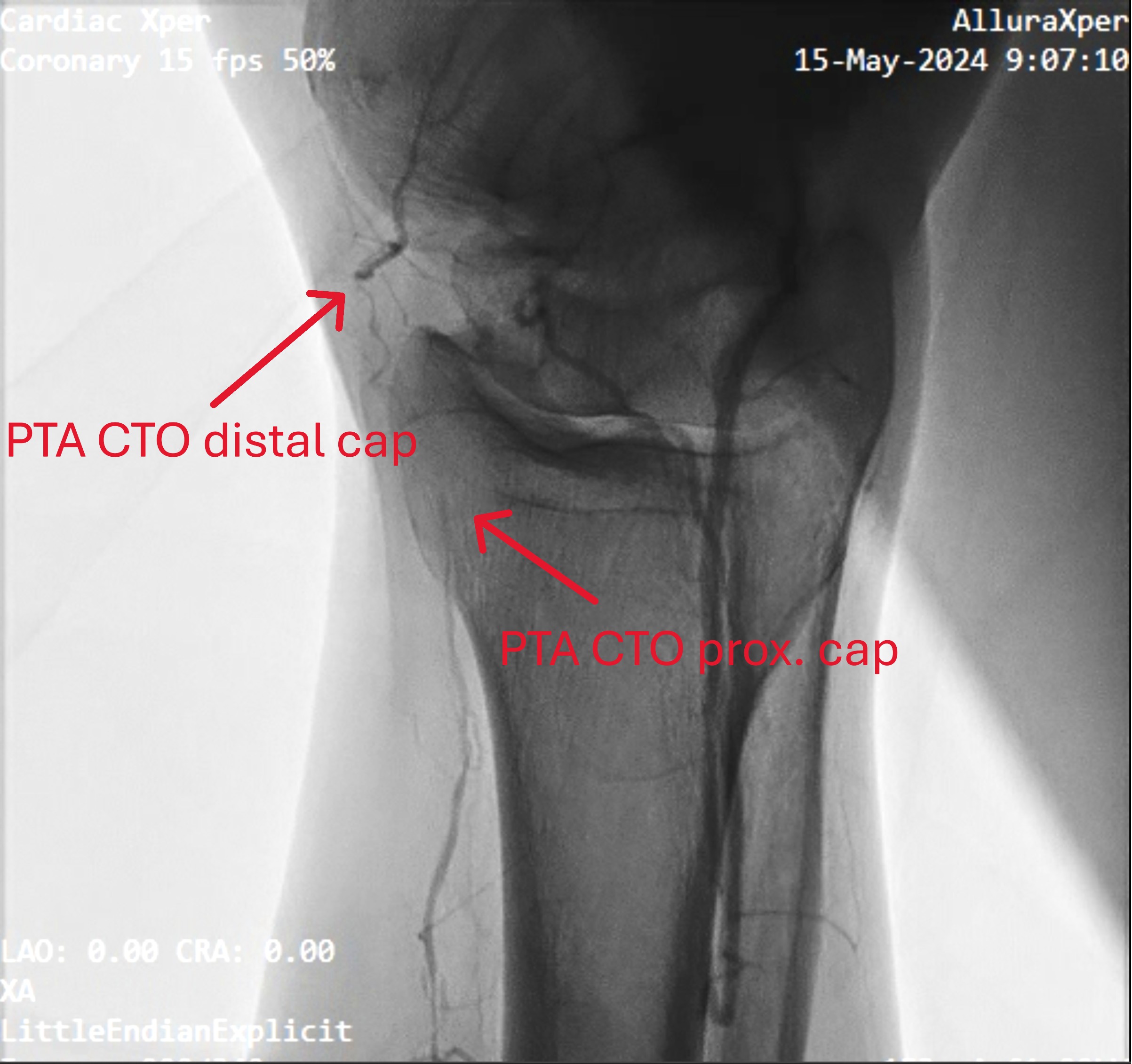
Interventional Management
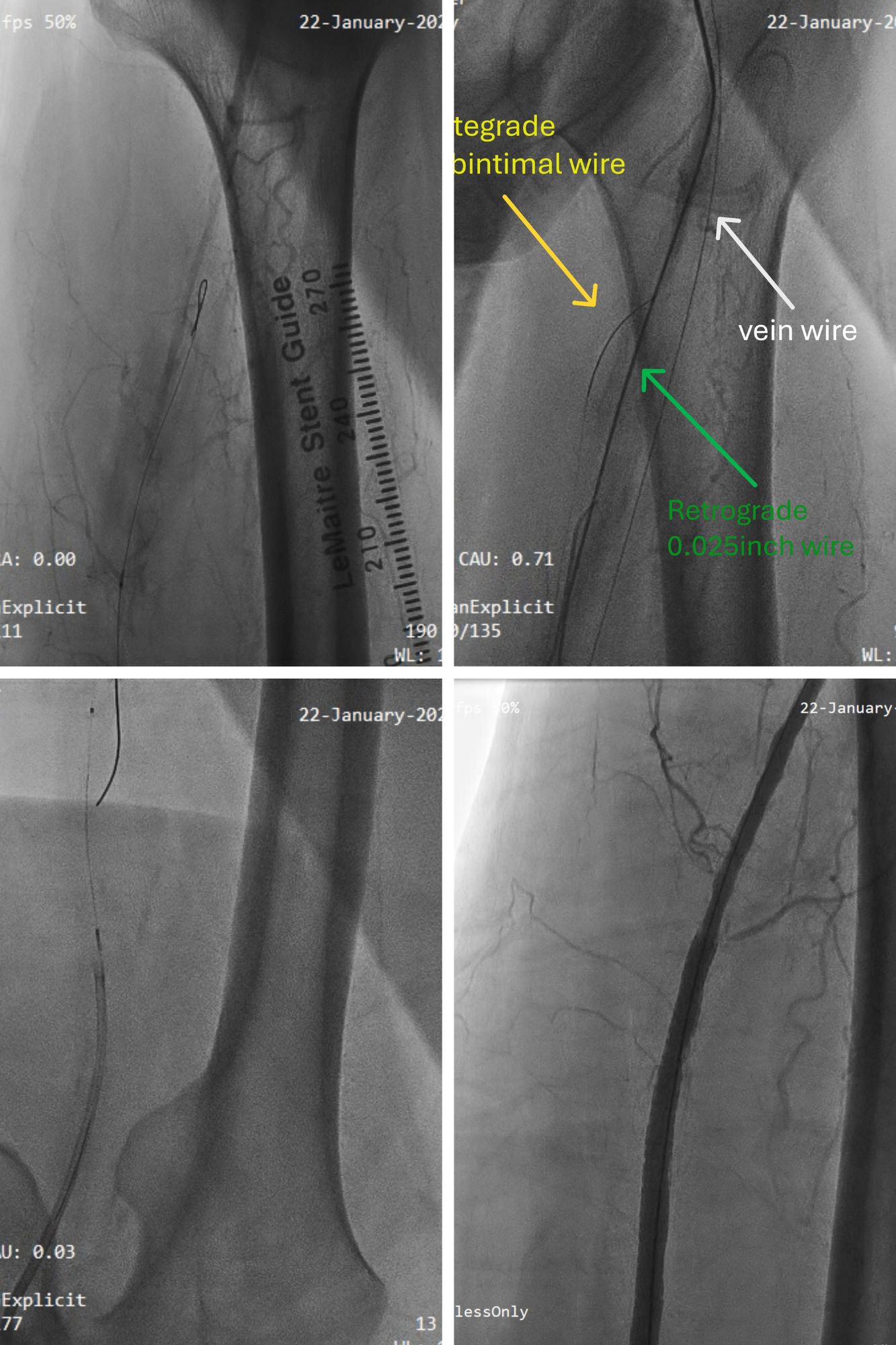
Procedural Step
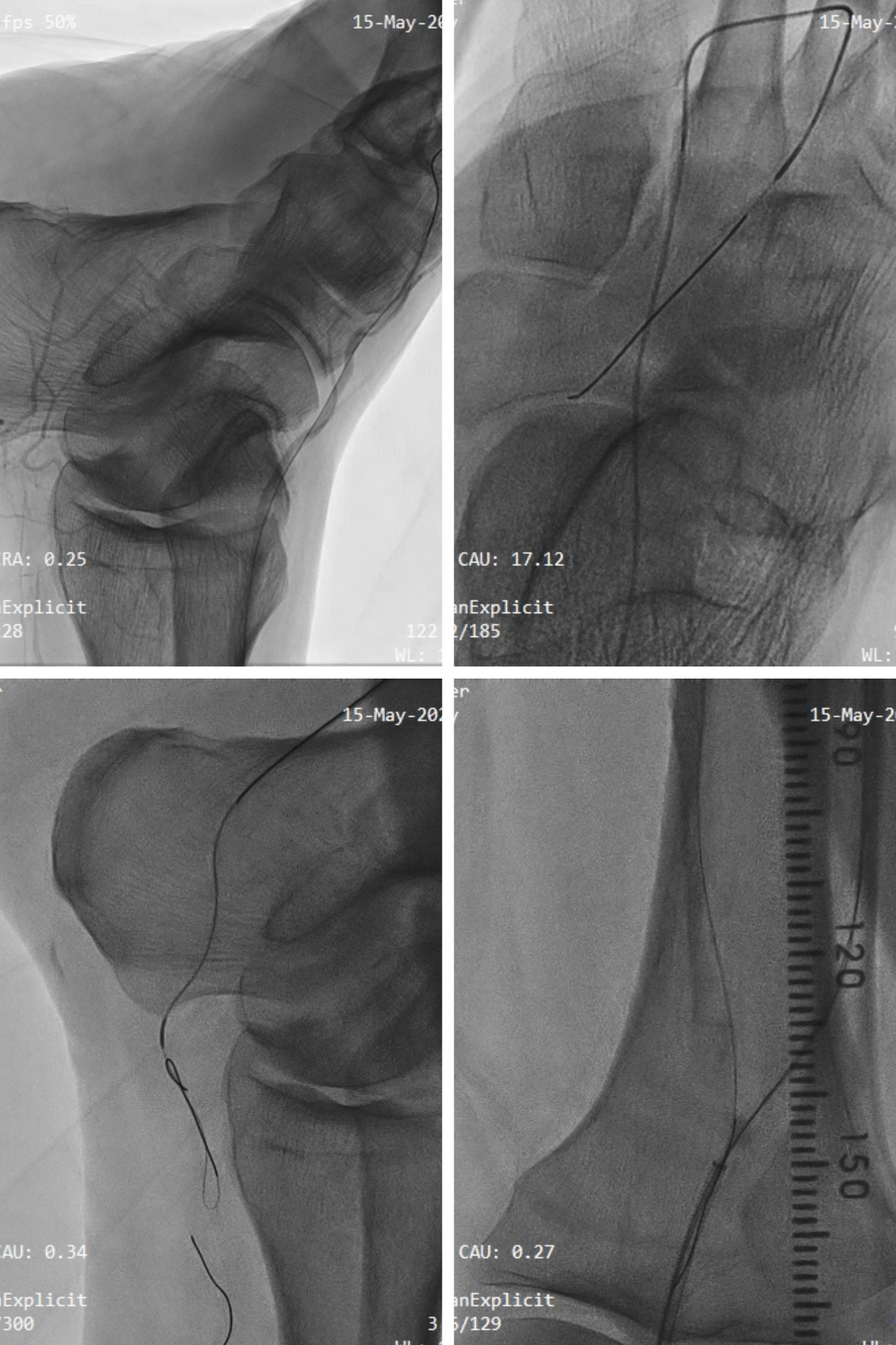
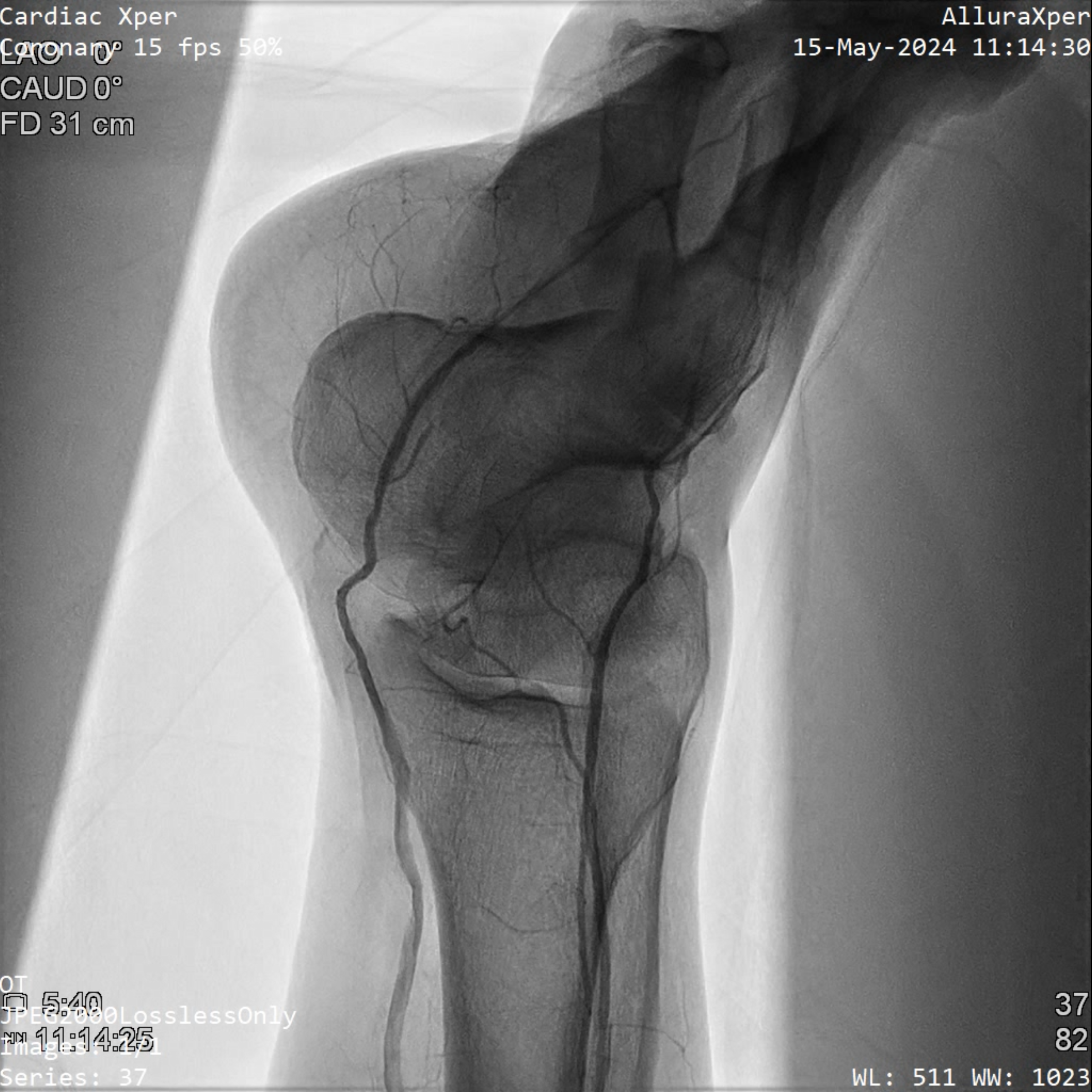
Antegrade wiring with 0.014 inch command wire with CXI, try to advance to distal true lumen, but failed. Try every possible way to manipulate the wire, but still in false lumen. so we puncture at popliteal artery(p2 area retrogradely). Successful retrograde wiring back to antegrade sheath, after externalization, use antegrade microcatheter to do tip in tehcnique into retrgrade sheath, then do balloon dilatation to seal the puncture wound. After stenting to SFA , final flow is acceptable. Then try to wiring down to distal ATA and dorsalis pedis, confirmed by fluoro. After that, do pedal loop tehcnique cross the pedal loop, back to lateral plantar artery. but very difficult to cross to distal PTA. So we do retrograde kissing cross and tip in to destination sheath in the p2 area. After final balloon dilataion, flow to distal ATA and PTA is good.
Case Summary
SFA , ATA and PTA CTO s/p successful retrograde crossing by puncture in popliteal artery, and pedal loop technique for PTA CTO crossing. Stenting with SUPERA in SFA dissection. follow up patient condition is good.