
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-178
Complex, High Risk Ad Hoc Percutaneous Coronary Intervention With Mechanical Circulatory Support in Unstable Non ST Elevation Myocardial Infarction
By Zhong Shiun Lee, Ciprian Dospinescu
Presenter
Zhong Shiun Lee
Authors
Zhong Shiun Lee1, Ciprian Dospinescu1
Affiliation
Aberdeen Royal Infirmary, United Kingdom1,
View Study Report
TCTAP C-178
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Complex, High Risk Ad Hoc Percutaneous Coronary Intervention With Mechanical Circulatory Support in Unstable Non ST Elevation Myocardial Infarction
Zhong Shiun Lee1, Ciprian Dospinescu1
Aberdeen Royal Infirmary, United Kingdom1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
84 years old lady admitted for non ST elevation myocardial infarction. She has background of chronic kidney disease stage 3, and had history of percutaneous coronary intervention to left anterior descending artery in 2005. She was clinically overloaded and blood pressure unsupported. She developed further chest pain and unresponsiveness with brief asystole while in the ward.
Relevant Test Results Prior to Catheterization
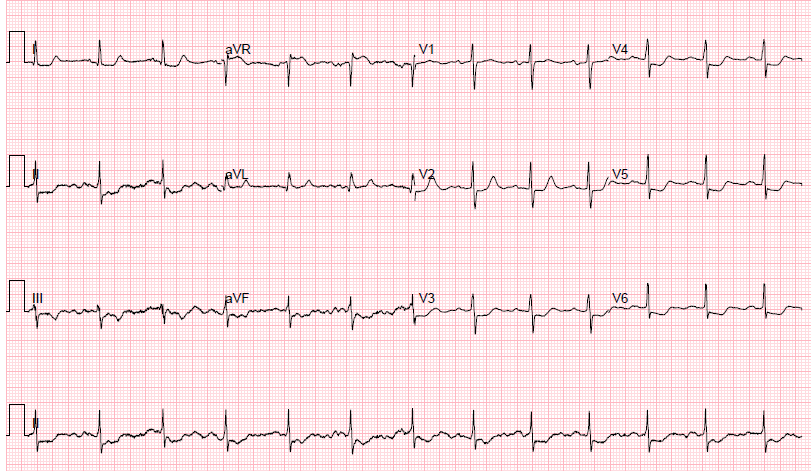
Chronic kidney disease stage 3.ECG sinus rhythm, ST elevation aVR with widespread ST depression.Echocardiogram showed moderate left ventricular systolic dysfunction.
Relevant Catheterization Findings
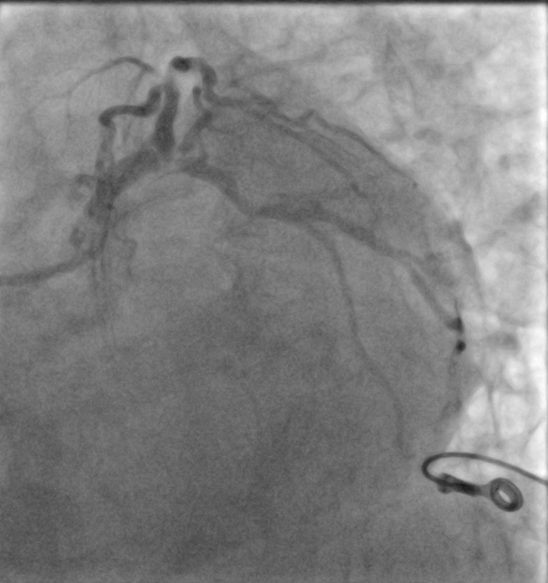
Right dominant systemCritical distal left main diseaseFocal severe disease mid right coronary arteryDiscussion with cardiothoracic surgeon, agree percutaneous coronary intervention most appropriate, with mechanical circulatory support.

Interventional Management
Procedural Step
Right femoral vein ultrasound guided access obtained upfront in case temporary pacing requiring.
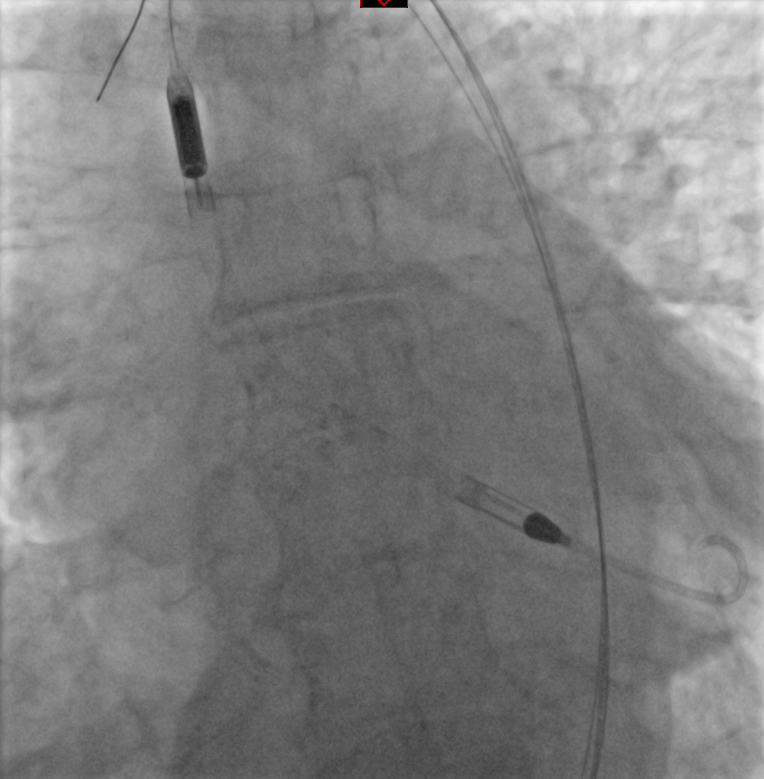
Right femoral artery ultrasound guided access. Iliofemoral angiogram showed suitable calibre vessel free of disease. Predeployed single ProGlide (Abbott, Chicago). Upsized to 14 French sheath over stiff wire. Aortic valve crossed with pigtail and J wire. Impella (Abiomed, Danvers) placed. 8French long femoral sheath inserted in the same sheath for coronary intervention.
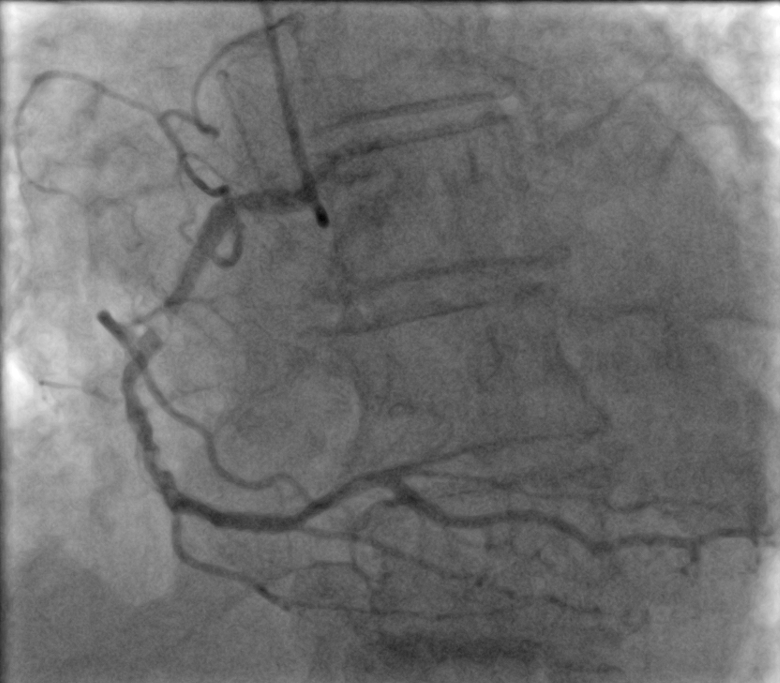
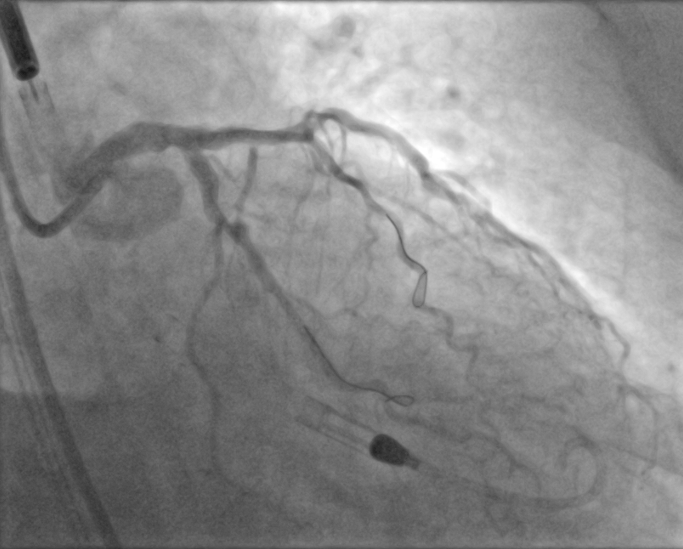
Intervention to left main bifurcation. EBU 3.5 7 French guiding catheter. Prowater (Asahi Intecc, Aichi) wired to left anterior descending (LAD). Pilot 50 (Abbott, Chicago) wired to left circumflex (LCx). Intravascular ultrasound guided. Double kissing crush technique used, with drug eluting stent 3.5 x 18mm to LCx and 3.5 x 18mm to LAD. Final kissing balloon with noncompliant balloons 4.0mm in LAD and 3.5mm in LCx. Left main stent postdilated with 4.5mm noncompliant balloon.
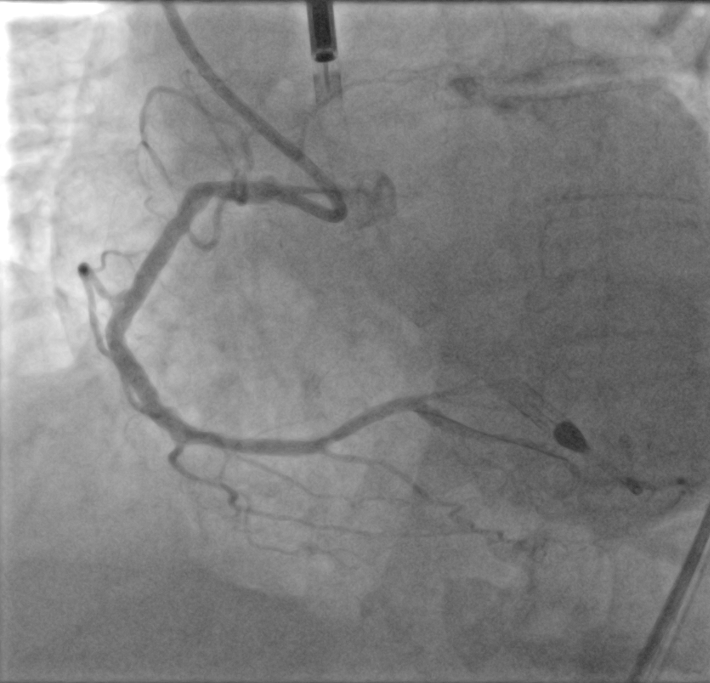
Intervention to right coronary artery (RCA). AL1.0 guiding catheter. Severely calcified lesion which required guide extension support and calcium modification with 4.0mm intravascular lithotripsy balloon. Drug eluting stent 3.5 x 48mm to proximal to mid RCA, postdilated with 3.5mm noncompliant balloon.
Haemodynamically stable throughout procedure.
Right femoral artery closed with predeployed ProGlide (Abbott, Chicago) and 8 French ANGIO-SEAL (Terumo, Shibuya).
Right femoral artery ultrasound guided access. Iliofemoral angiogram showed suitable calibre vessel free of disease. Predeployed single ProGlide (Abbott, Chicago). Upsized to 14 French sheath over stiff wire. Aortic valve crossed with pigtail and J wire. Impella (Abiomed, Danvers) placed. 8French long femoral sheath inserted in the same sheath for coronary intervention.
Intervention to left main bifurcation. EBU 3.5 7 French guiding catheter. Prowater (Asahi Intecc, Aichi) wired to left anterior descending (LAD). Pilot 50 (Abbott, Chicago) wired to left circumflex (LCx). Intravascular ultrasound guided. Double kissing crush technique used, with drug eluting stent 3.5 x 18mm to LCx and 3.5 x 18mm to LAD. Final kissing balloon with noncompliant balloons 4.0mm in LAD and 3.5mm in LCx. Left main stent postdilated with 4.5mm noncompliant balloon.
Intervention to right coronary artery (RCA). AL1.0 guiding catheter. Severely calcified lesion which required guide extension support and calcium modification with 4.0mm intravascular lithotripsy balloon. Drug eluting stent 3.5 x 48mm to proximal to mid RCA, postdilated with 3.5mm noncompliant balloon.
Haemodynamically stable throughout procedure.
Right femoral artery closed with predeployed ProGlide (Abbott, Chicago) and 8 French ANGIO-SEAL (Terumo, Shibuya).
Case Summary
This complex, high risk intervention was aided by a robust multidisciplinary team discussion. The upfront use of mechanical circulatory support provided haemodynamic stability that allowed for complex intervention to proceed smoothly and achieving a single stage complete revascularization. Large bore vascular access requires meticulous attention to each step to reduce the risk of bleeding or ischaemic complications. The single femoral access allowed advancement of mechanical circulatory support device and also for percutaneous coronary intervention. Intravascular imaging is now an indispensable tool in optimising intervention outcomes.