
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-096
Obligatory Challenging Way in a "Retrograde CTO PCI to RCA"
By Ramy Mohamed Atlm, Salma Mohamed Elshokafy
Presenter
Ramy Mohamed Atlm
Authors
Ramy Mohamed Atlm1, Salma Mohamed Elshokafy1
Affiliation
Tanta University Hospital, Egypt1,
View Study Report
TCTAP C-096
Coronary - Complex PCI - CTO
Obligatory Challenging Way in a "Retrograde CTO PCI to RCA"
Ramy Mohamed Atlm1, Salma Mohamed Elshokafy1
Tanta University Hospital, Egypt1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
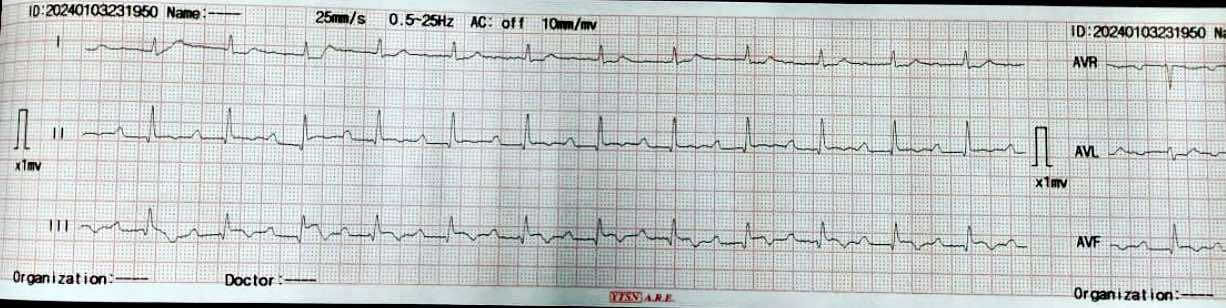
Male patient, 68 years old , Diabetic , Hypertensive .Ischemic heart disease with PCI to LAD 2 years ago .Recurrent chest pain with multiple admissions with ACS during the last 3 months for which coronary angiography was recommended ECG: SR with ST , T changes in inferior leads .ECHO: IHD with EF 52%, RSWMAs in the form of ( apical and Mid inferior and infero-septal wall hypokinesia ) with Moderate mitral valve incompetence BLPR: 140/90 mmHg , HR : 75 B/M , TEMP: 36.2 c , RBS : 258
Relevant Test Results Prior to Catheterization
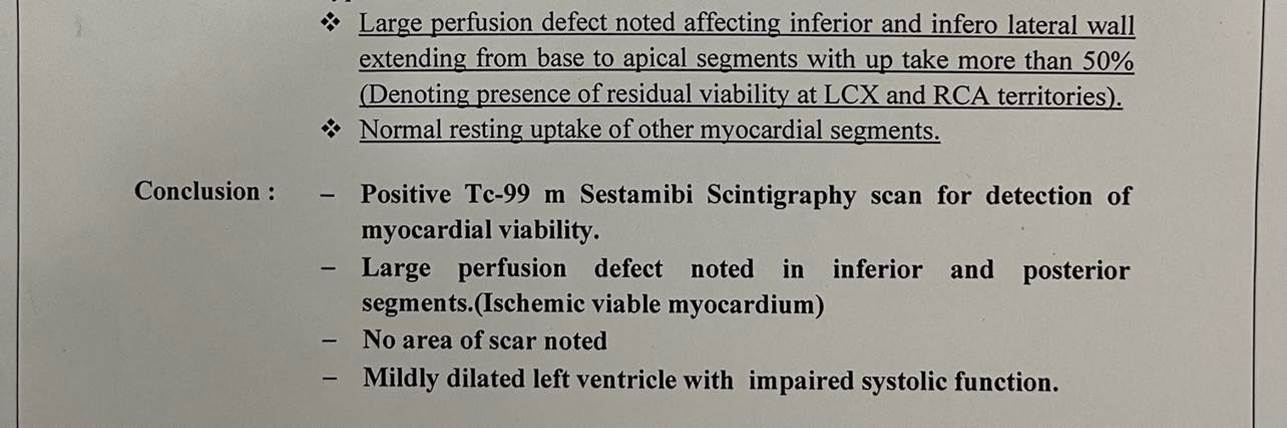
Coronary angiography was done showing patent previous LAD stent and CTO RCA ** Symptomatic patient ** Good EF with SWMA at RCA territory ** Recurrent admissions with ACS And also Thallium study was done to document Ischemic burden of RCA territory and was positive
Relevant Catheterization Findings
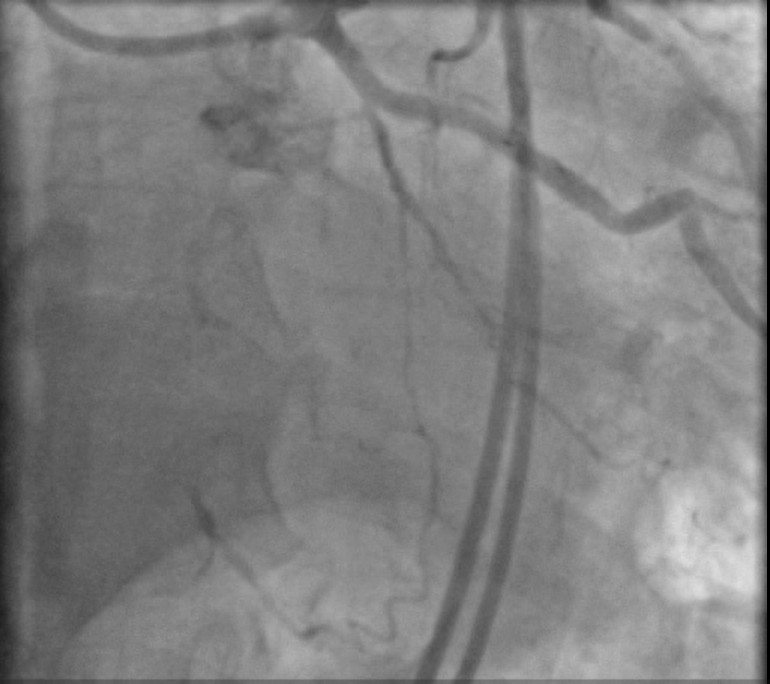
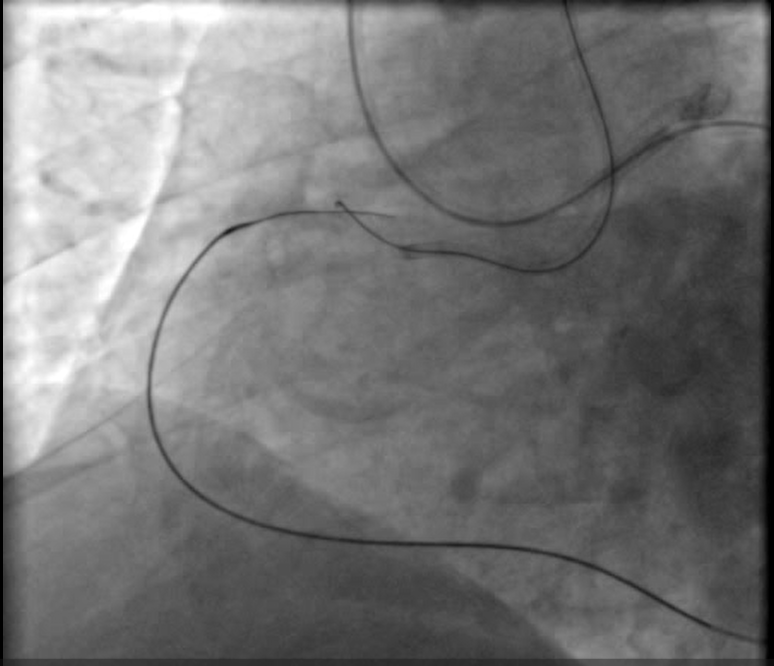
LM : Normal vessel bifurcating into LAD & LCX.LAD : Atherosclerotic vessel with patent previously deployed stent .LCX: A atherosclerotic small diffusely diseased vessel .RCA : Atherosclerotic vessel with proximal CTO with bridging collaterals and retrograde good septal and epicardial collaterals from left system

Interventional Management
Procedural Step
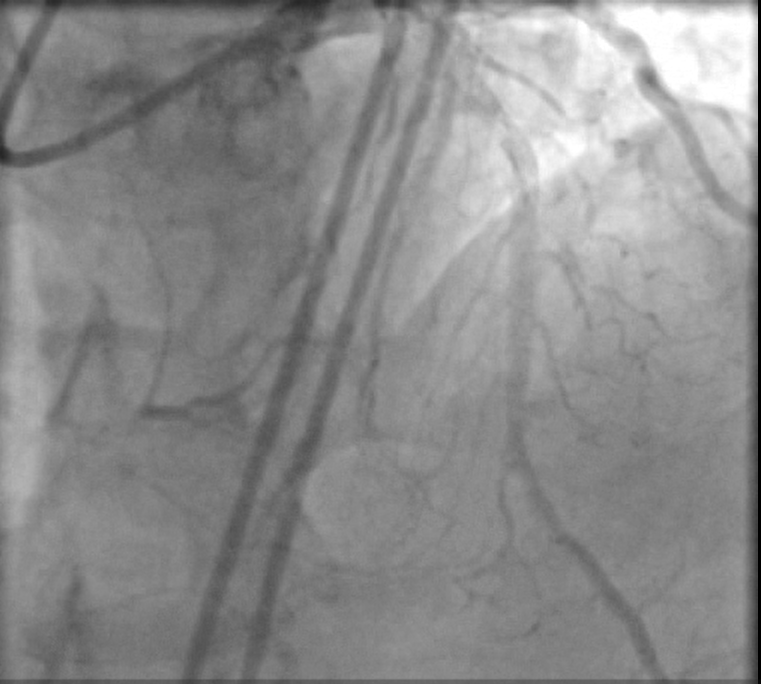
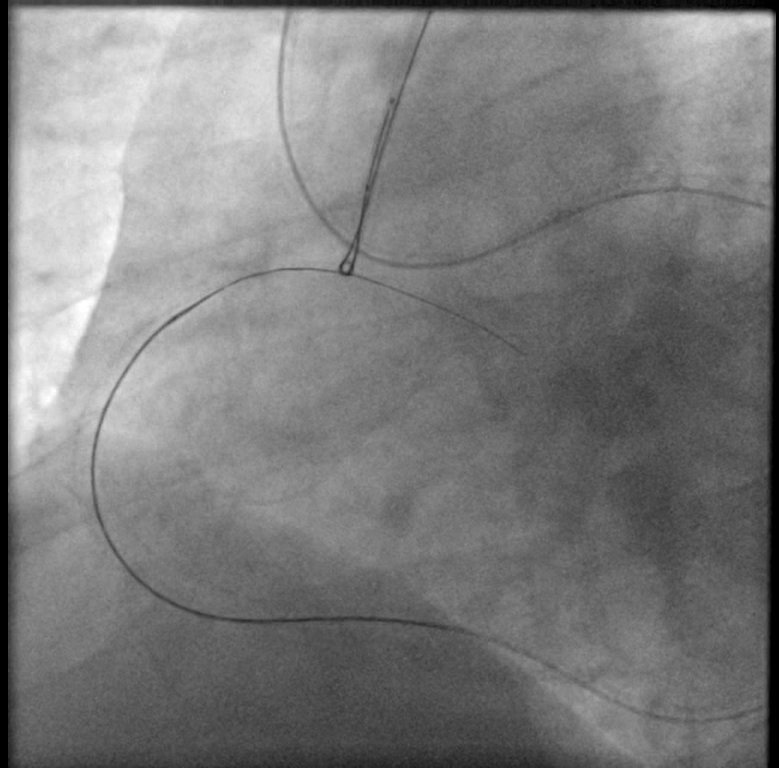
Dual femoral access , Dual injection through AL1 7F & XB4 7F Target vessel assessment ( RCA ) with calculation of J-CTO score then deciding which strategy we decided a Trial antegrade, If failed , Retrograde through septals , If failed , shift to epicardial collateral.Antegrade Trial with GAIA Wires , Corsair MC failed , Retrograde trial through septals failed as it seems not connected shifting strategy to epicardial : Sion blue navigated through epicardial collaterals , corsair 150 MC successfully passed through PL branch MC advanced to distal Cap & GAIA 2nd wire successfully pierced distal cap , but failed to entre antegrade guide Trial snaring through AL guiding by a home made snare but failed , Guiding changed to JR with successful snaring of wire into antegrade guide followed by MCPilot 50 wire introduced through retrograde MC ( Rendezvous Technique , Reverse TIP IN ) then MC Withdrawn we started conventional PCI with Antegrade Balloon dilatation 2.5 * 15 mm semicompliant then 3.5 * 15 mm NC balloons Then stenting with 2 overlapping DES with postdialtation with 4*15 NC balloon with final good angiographic results

Case Summary
** Assessing CC size is mandatory , as sizable epicardial channel can accommodate corsair MC.** Snaring and Rendezvous ( TIP IN ) technique can over come challenges during standard wire externalization .** Short wires ( 180 cm ) NEVER be snared , but if it happens the wire should be pulled out from the antegrade guide , without attempting to retrieve it from the retrograde direction . ** Keep your mind active and Always be prepared for surprises