
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-225
Percutaneous Strategy for Heterogenous Valve Pathologies - Is There Any Wisdom in It?
By John Jose Erungaren
Presenter
John Jose Erungaren
Authors
John Jose Erungaren1
Affiliation
Christian Medical College Hospital Vellore, India1,
View Study Report
TCTAP C-225
Structural - Tricuspid Valve Intervention
Percutaneous Strategy for Heterogenous Valve Pathologies - Is There Any Wisdom in It?
John Jose Erungaren1
Christian Medical College Hospital Vellore, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
65-year-old male presented with 3-month history of shortness of breath, bilateral pedal oedema, ascites and recurrent hospitalization for heart failure. He had mitral valve replacement- mechanical plus tricuspid annuloplasty in 2010. His risk profile included atrial fibrillation, COPD, seizure disorder, chronic liver disease, low body weight (36kg,BMI-15.6kg/m2), and recent subdural hematoma with burr hole evacuation. Examination showed anasarca and pulmonary oedema

Relevant Test Results Prior to Catheterization
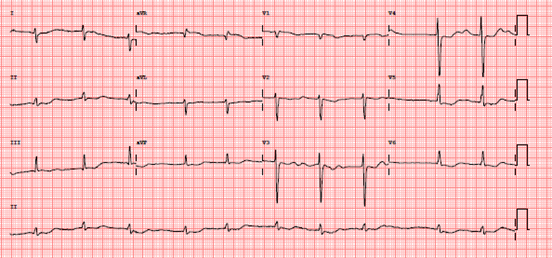
ECG- Atrial fibrillationChest X-ray: Cardiomegaly,bilateral pleural effusion, pulmonary congestion

Relevant Catheterization Findings
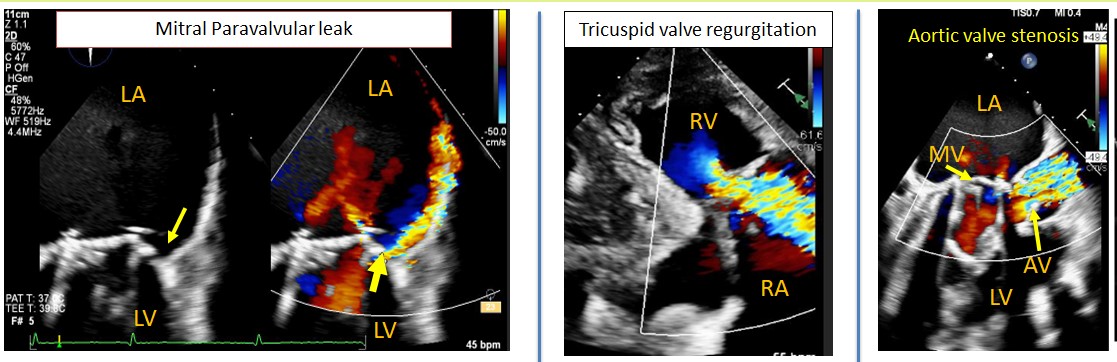
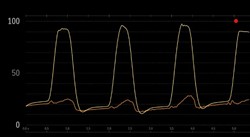
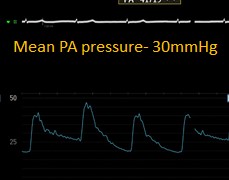
Coronary angiogram - no significant diseaseMean pulmonary artery pressure-30mmHgNo significant transmitral gradientV wave amplitude > 25mmHg in RA tracing
DiagnosisAortic stenosis and regurgitation of rheumatic etiology
DiagnosisAortic stenosis and regurgitation of rheumatic etiology
Interventional Management
Procedural Step
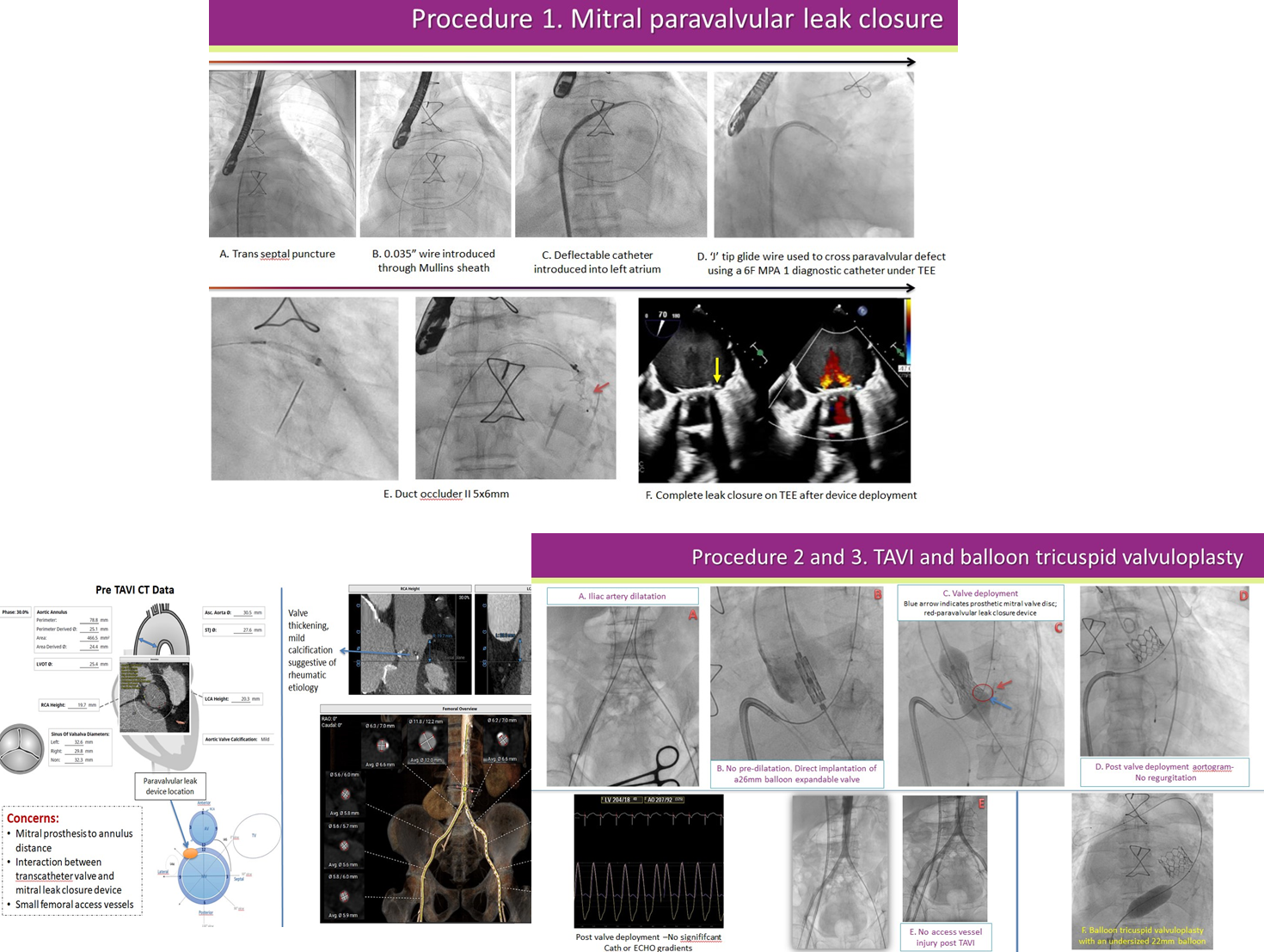
Treatment plan A: Surgical repair of mitral paravalvular leak, aortic and tricuspid valve replacement • Declined by surgeons in view of co-morbidities and high operative risk. Hence treatment plan B outlined below was considered Treatment plan B: Staged procedure • Stage1: Closure of mitral paravalvular leak with a duct occluder, transcatheter aortic valve implantation (TAVI) and balloon tricuspid valvuloplasty (Regurgitation already severe, valvuloplasty to relieve restriction) • Stage2 (A week later): Bicaval valve (TRIC)implantation for tricuspid valve- But inferior vena caval (IVC) Valve of TRIC embolized to right atrium in recovery room, it was retrieved surgically, surgical IVC valve implantation attempted but not possible. CT review of IVC-hepatic vein anatomy showed
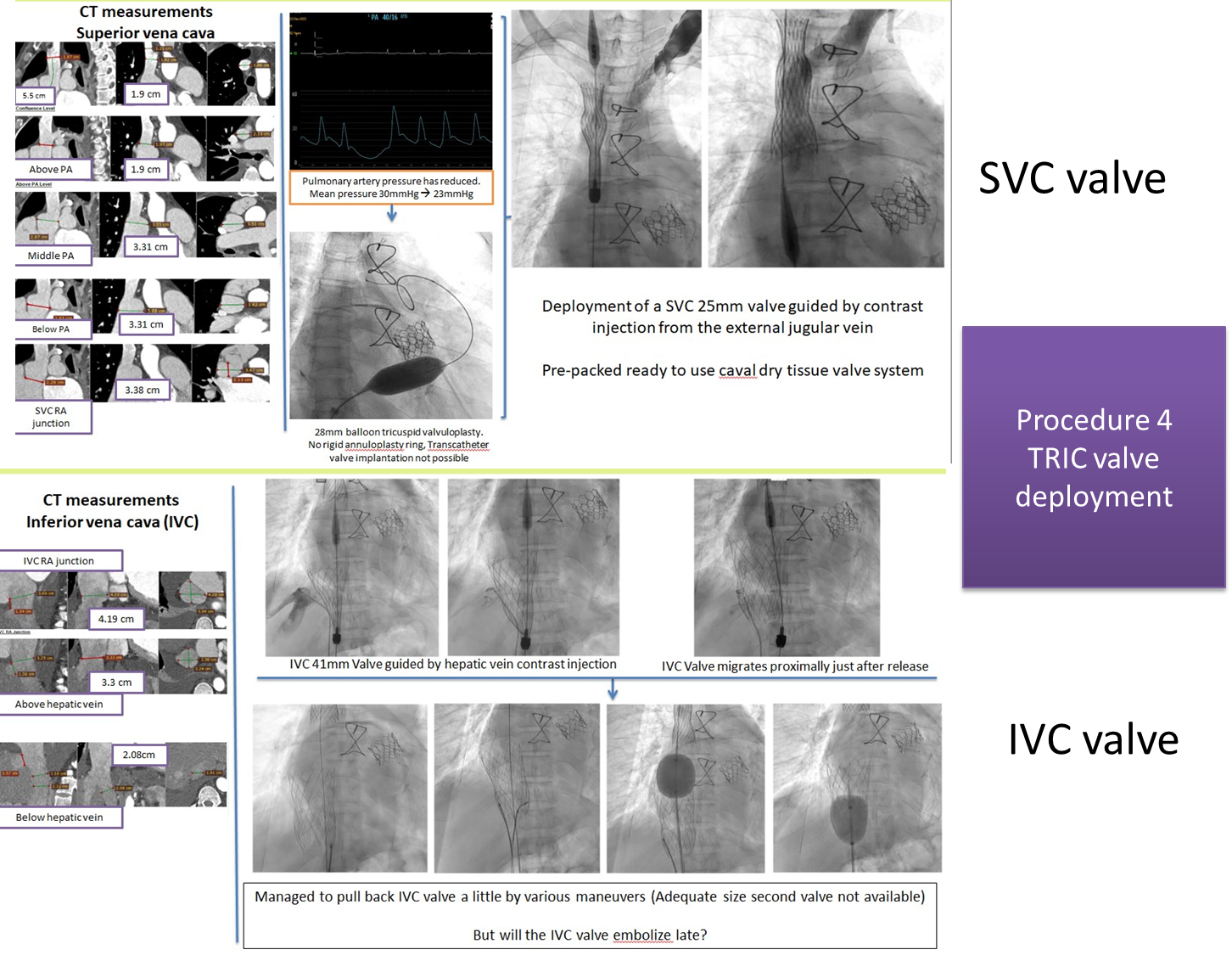
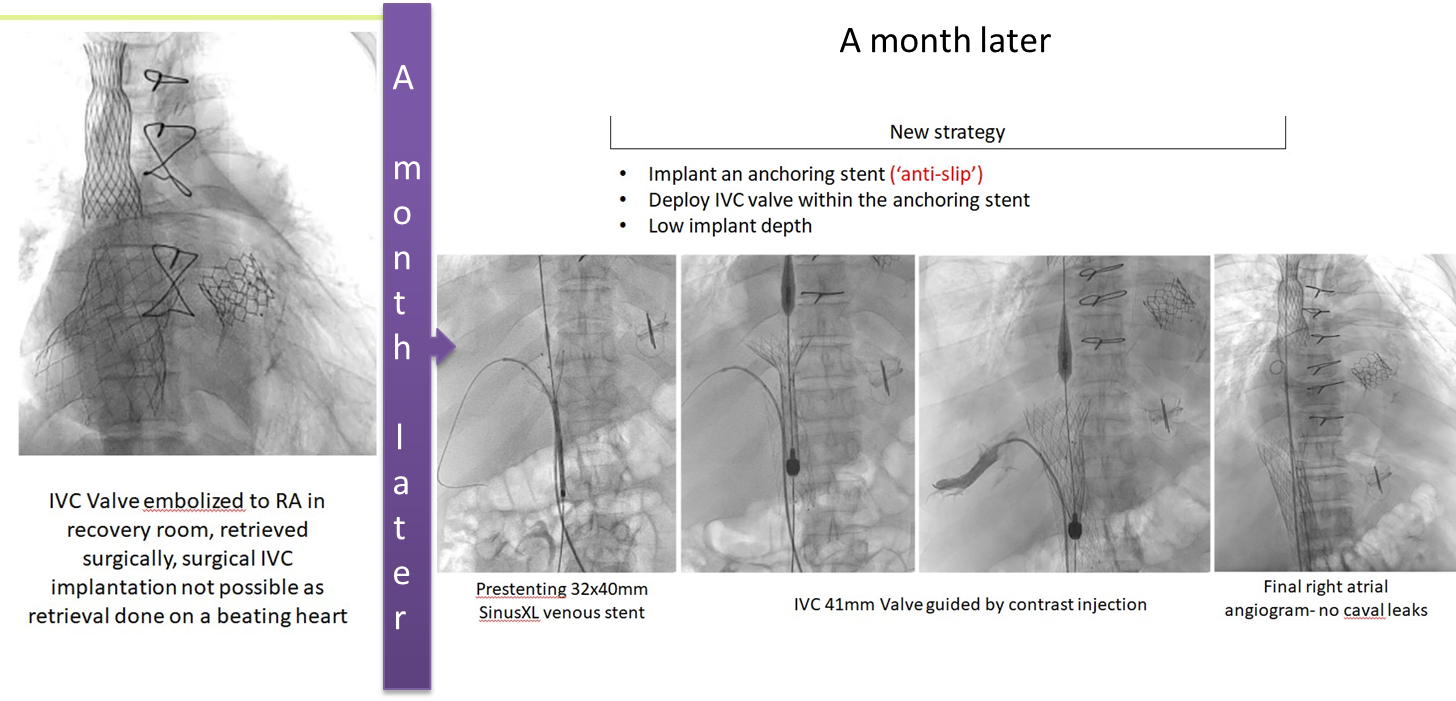
- Large IVC diameter at RA junction as compared to infra hepatic segment IVC diameter
- Short hepatic vein to right atrial distance
Case Summary
What we learned from our experience?