
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-062
Crack and Shock: A Case Report on Angioplasty in Elderly
By Wei Liang Lee, Ting Yuen Beh
Presenter
Wei Liang Lee
Authors
Wei Liang Lee1, Ting Yuen Beh1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-062
Coronary - Complex PCI - Calcified Lesion
Crack and Shock: A Case Report on Angioplasty in Elderly
Wei Liang Lee1, Ting Yuen Beh1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
85 years old gentlemanComorbidities: Hypertension, Dyslipidemia, smokerRecent NSTEMI in March 2024 at a district hospital.
Referred for cardiac assessment.
Upon review in clinic,
He was having frequent angina at rest
lungs auscultation was clear, no pedal edema
Relevant Test Results Prior to Catheterization
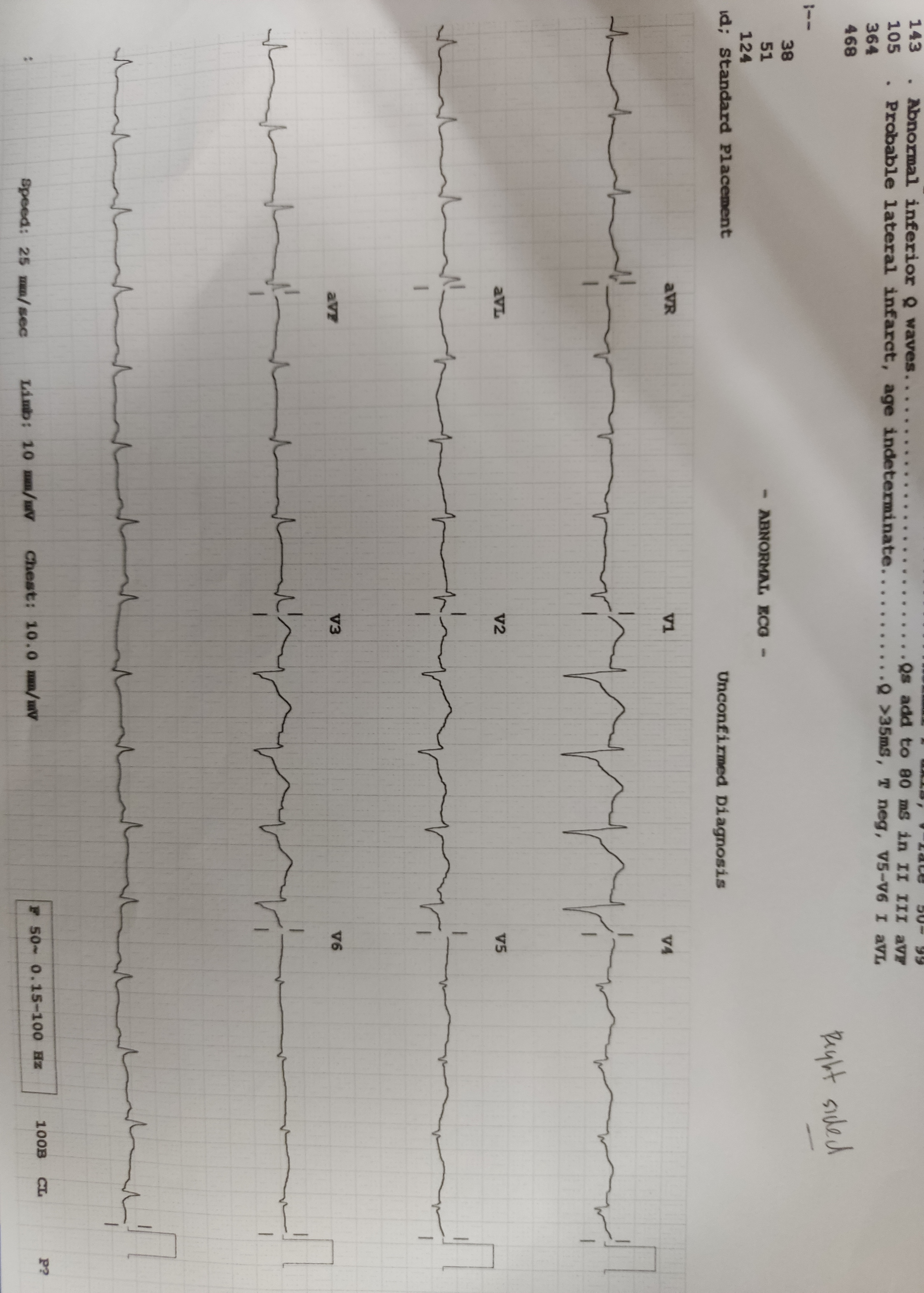
ECG: sinus, ST depression at anterior leads
Echocardiography: LVEF 40-45%, hypokinesia apical and anterior
He was admitted for coronary angiogram.
Relevant Catheterization Findings
Left main stem- shortLAD- severe stenosis ostial-proximalLCx- dominant, severe stenosis at midsegment (ulcerated plaque)RCA- small vessel, severe stenosisproximal
Interventional Management
Procedural Step
Guide Catheter EBU 3.5/6Fr
PCI to LCxCoronary wire runthrough floppy to LCx, Sion Blue to LADPredilate: Scoring NC balloon 2.5x15mmDrug Eluting Stent: 2.5x18mm Postdilate: NC balloon 3.0x15mm up to 12 atm
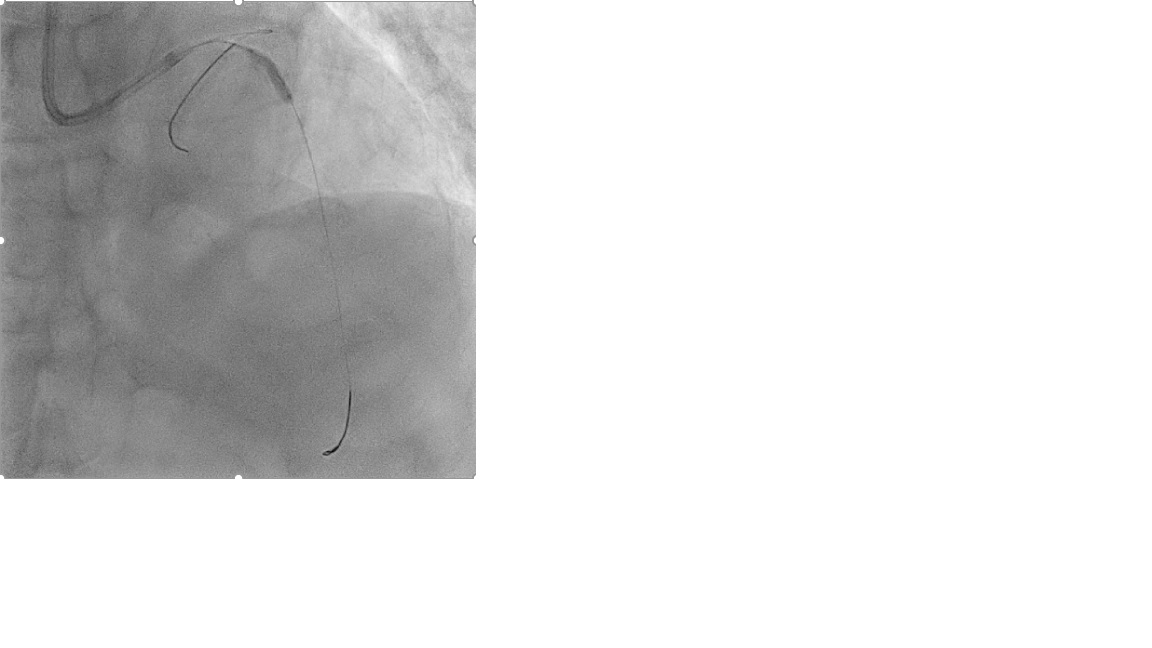
PCI to LADTight proximal calcified stenosis. Predilate with SC balloon 1.5x15mm to facilitate IVUS passageSC balloon 1.5x15mm did not open fullyTried with SC balloon 2.0x15mm- balloon rupturedThen tried NC 2.0x15mm balloon up to 16atm, lesion open partially. Proceeded with IVUSIVUS showed calcified nodule.Predilate with Scoring NC balloon 3.0x13mm at high pressure 24atm=> balloon wasting IVL 3.0mm at 6-8atm for 80 pulsesFurther predilate with scoring balloon 3.0x13mm and OPN 3.0x10mm up to 30atm, calcium successfully crackedProceeded with drug eluting stent 3.0x35mm
PCI to LCxCoronary wire runthrough floppy to LCx, Sion Blue to LADPredilate: Scoring NC balloon 2.5x15mmDrug Eluting Stent: 2.5x18mm Postdilate: NC balloon 3.0x15mm up to 12 atm
PCI to LADTight proximal calcified stenosis. Predilate with SC balloon 1.5x15mm to facilitate IVUS passageSC balloon 1.5x15mm did not open fullyTried with SC balloon 2.0x15mm- balloon rupturedThen tried NC 2.0x15mm balloon up to 16atm, lesion open partially. Proceeded with IVUSIVUS showed calcified nodule.Predilate with Scoring NC balloon 3.0x13mm at high pressure 24atm=> balloon wasting IVL 3.0mm at 6-8atm for 80 pulsesFurther predilate with scoring balloon 3.0x13mm and OPN 3.0x10mm up to 30atm, calcium successfully crackedProceeded with drug eluting stent 3.0x35mm
Case Summary
Lesion preparation is crucial for the successful coronary stent implantation.NC balloon and scoring balloon remain the first line when dealing with calcified lesion.However, novel approaches such as lithotripsy can be consider when conventional balloon fails.