
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-058
Embrace the Unconventional Approach to Deal With Angulated Diffuse Calcified Lesion
By Andrico Tobing
Presenter
Andrico Tobing
Authors
Andrico Tobing1
Affiliation
Murni Teguh Memorial Hospital, Indonesia1,
View Study Report
TCTAP C-058
Coronary - Complex PCI - Calcified Lesion
Embrace the Unconventional Approach to Deal With Angulated Diffuse Calcified Lesion
Andrico Tobing1
Murni Teguh Memorial Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 67-year-old Male with a history of Type 2 diabetes melitus, hypertension, and dyslipidemia was admitted because of worsening chest pain for the last 3 months (CCS III). The patient is a heavy smoker and suffered from uncontrolled Diabetes (HbA1C 9.7). His vital signs were stable and laboratory examination came unremarkable.
Relevant Test Results Prior to Catheterization
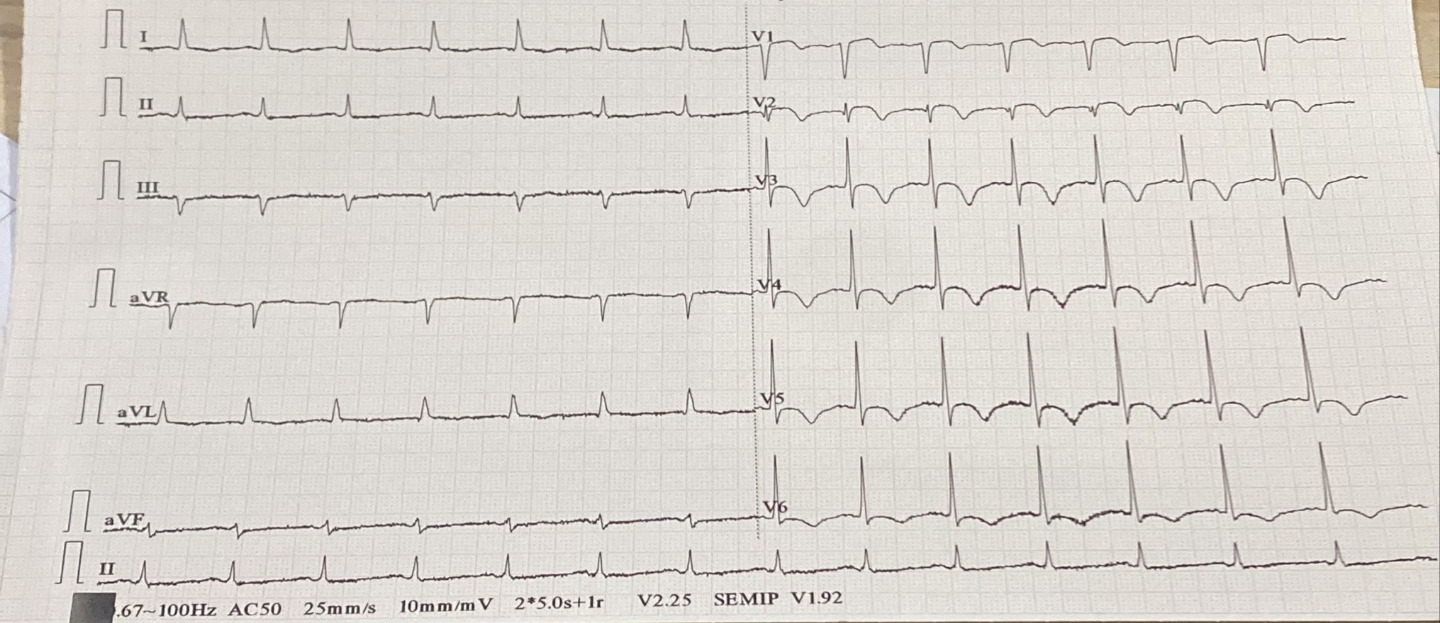
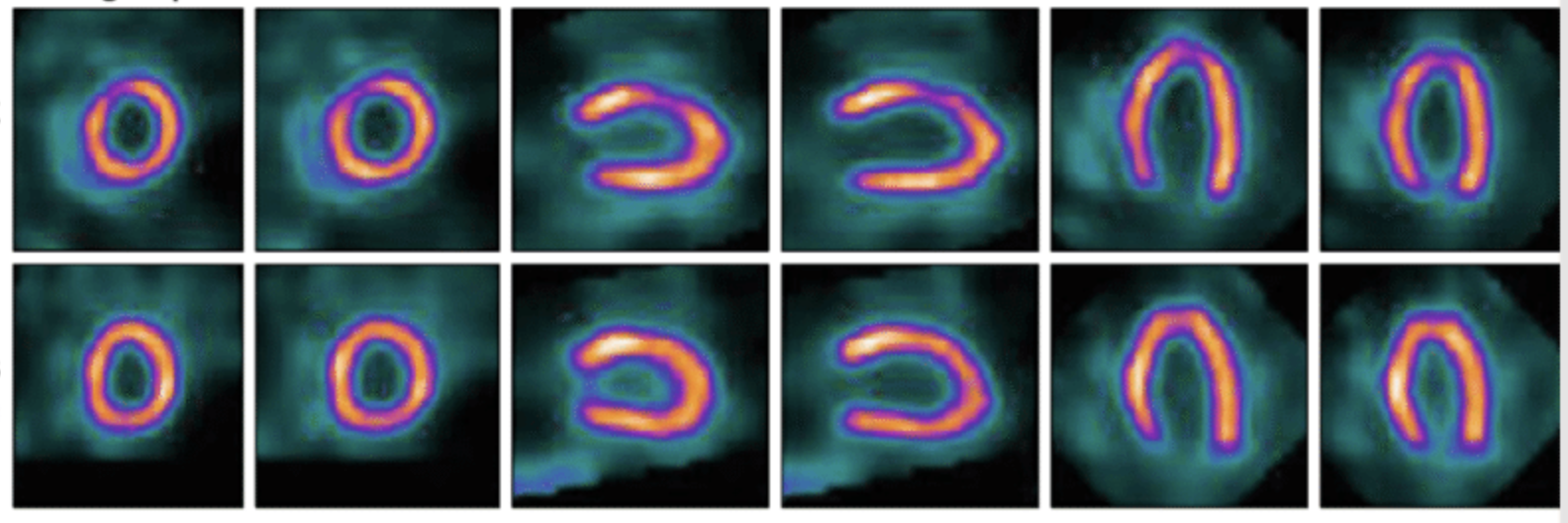
ECG showed Sinus rhythm and T-wave inversion on anterolateral leads. MPI revealed dilated LAD and reversible defect on LAD territory. Echocardiography showed EF 40 %, anteroseptal wall hypokinetic, mild Mitral Regurgitation with LVH.
Relevant Catheterization Findings
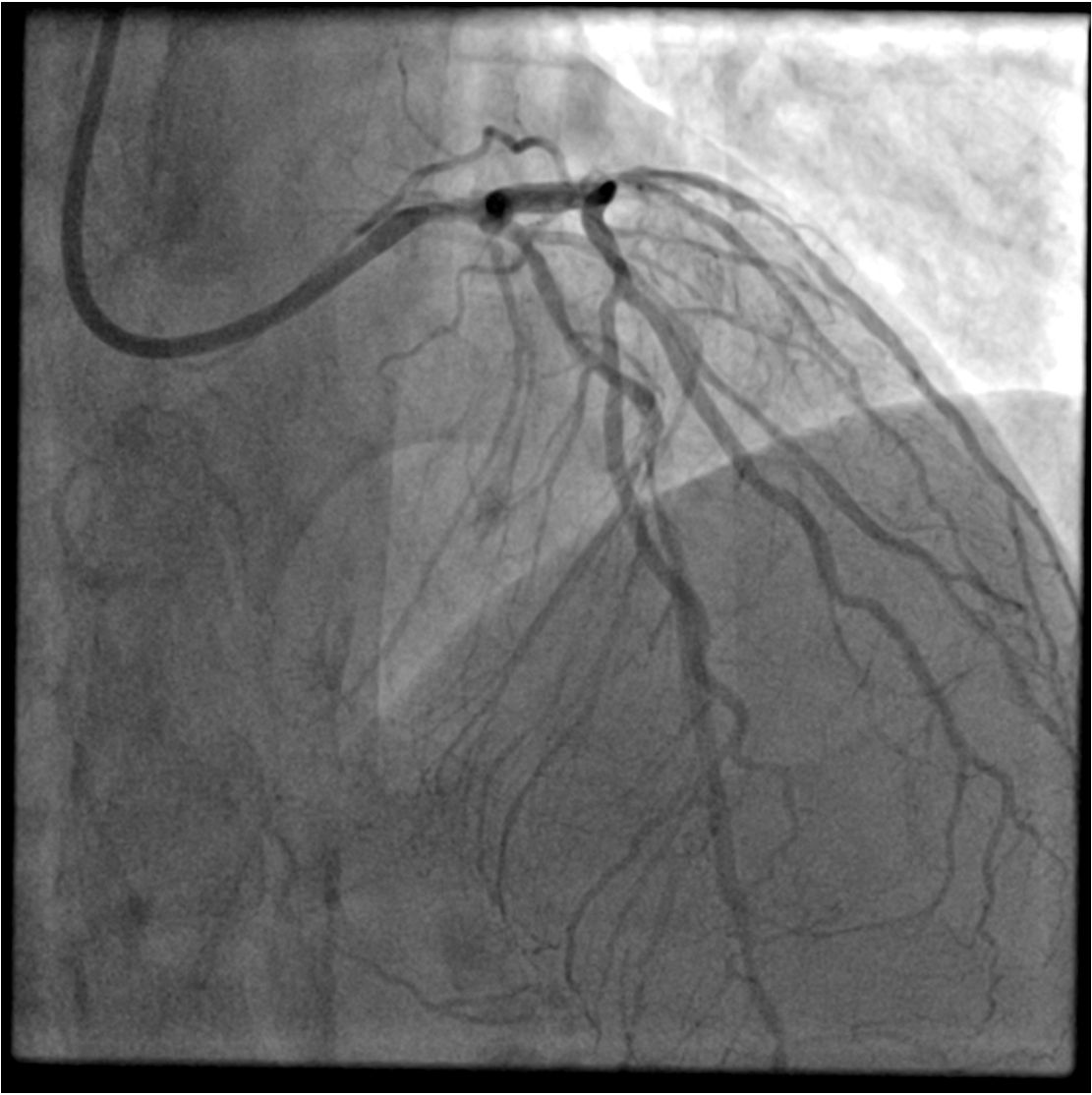
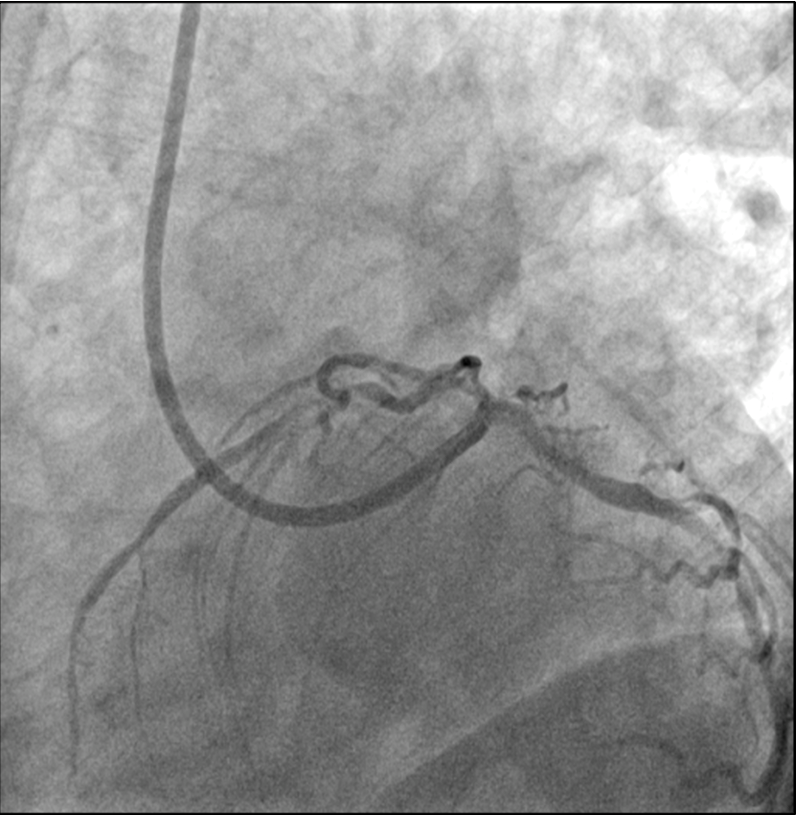
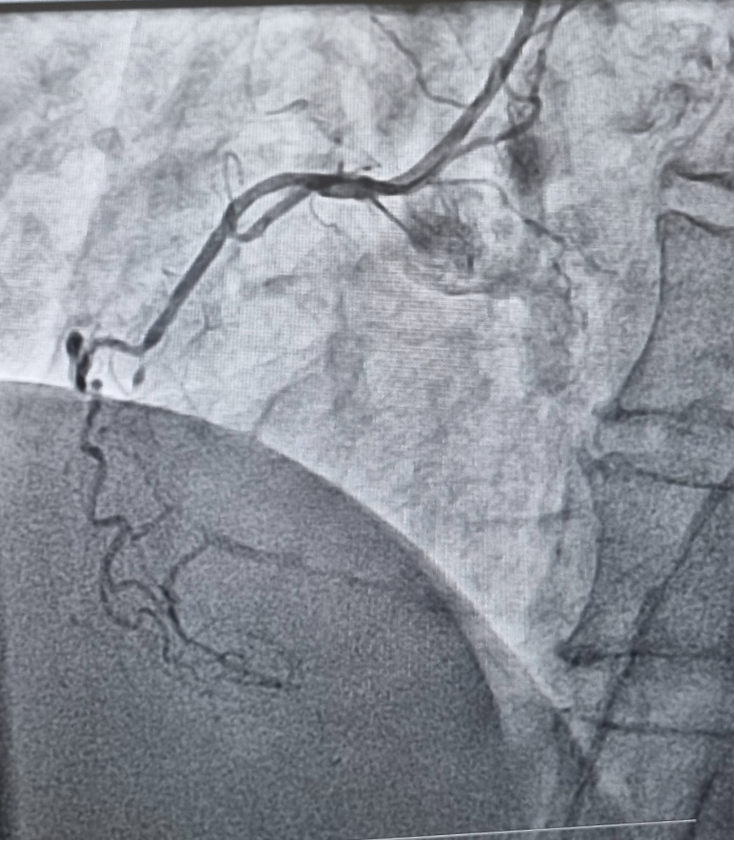
Left coronary angiography showed angulated diffuse calcified Left main (LM) to Proximal LAD 80 % stenosis, mid LAD 90 % stenosis, calcified proximal LCx 50% stenosis and mid-distal 60% LCx stenosis. Right coronary angiography showed diffuse 60% proximal stenosis and CTO on mid RCA (collateralization from LAD). Syntax score was 30 and revascularization strategy between PCI or CABG was discussed to the patient but patient finally declined the CABG.
Interventional Management
Procedural Step
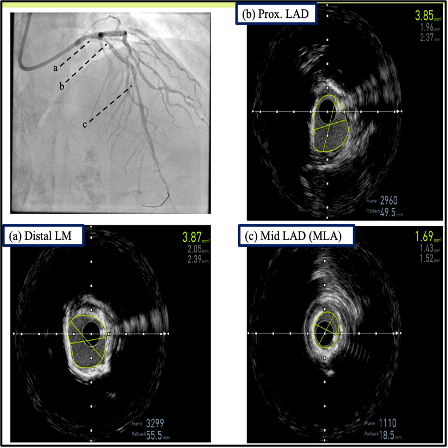
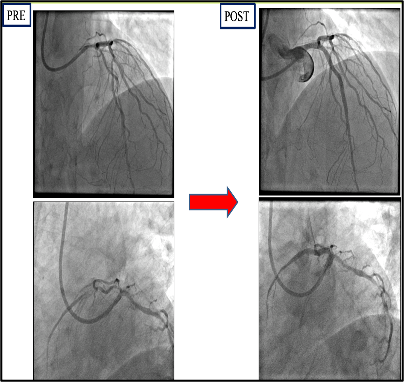
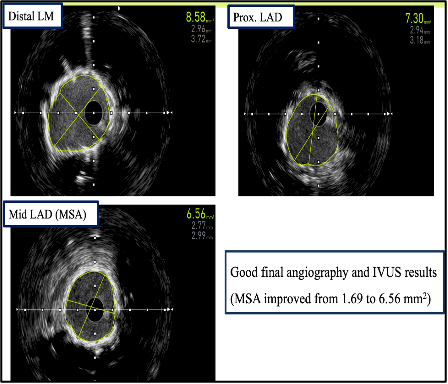
Left coronary was cannulated with 7F EBU 3.5 GC. Runthrough NS wire was advanced into the distal LAD with Finecross microcatheter. IVUS was unable to advance across the lesion. We considered this as an uncrossable lesion. Then we used rotational atherectomy for lesion preparation. Wire was exchanged to Rotafloppy guidewire. We performed Rotational atherectomy using Rota Pro 1.25 mm Burr with maximum speed 180.000 rpm. 10 runs were performed from LM to proximal LAD but Rotaburr was unable to pass through the mid LAD. 13 more runs were performed from proximal to mid LAD, but rotablator was still unable to cross and ablate the mid LAD. Lesion was next predilated with 1.25 x 15 mm SC balloon (12 atm) and 2.0 x 15 mm NC balloon (24 atm). IVUS was performed and showed calcium fractures at multiple lesion sites. IVUS also revealed residual concentric superficial and deep calcifications at mid LAD & distal LM (MLA 1.69 mm2). Since we concluded that lesion preparation was still inadequate, we proceeded to use Intravascular Lithotripsy (IVL) for better lesion preparation, and we concluded our atherectomy as “Halfway Rotablation”. We performed IVL using Shockwave 3.0 x12 mm C2 IVL balloon. 50 pulses were administered at mid LAD and 30 pulses at distal LM. DES 3.0 x 32 mm was implanted at proximal - mid LAD and overlapped with DES 3.5 x 28 mm at LM - proximal LAD. Stents were postdilated with 3.0, 3.5 and 4.0 NC balloon. Final angiography and OCT showed good result (MSA 6.56 mm2).
Case Summary
Halfway Rotablation is a novel technique for angulated diffuse calcified lesion, in which operator does not advance the burr throughout the calcified lesion, but otherwise performs balloon dilatation to treat the remaining lesion. Halfway rotablation may decrease incidence of severe complications during rotational atherectomy. Imaging guidance are essential as a guidance to improve procedural outcome.