
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-177
PCI in Left Main Coronary Lesions With Severe Heart Failure Supported by PulseCath iVAC 2L: A Game-Changing Approach
By Hsin Yi Huang, Bin Han Lo
Presenter
Hsin Yi Huang
Authors
Hsin Yi Huang1, Bin Han Lo1
Affiliation
China Medical University Hospital, Taiwan1,
View Study Report
TCTAP C-177
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
PCI in Left Main Coronary Lesions With Severe Heart Failure Supported by PulseCath iVAC 2L: A Game-Changing Approach
Hsin Yi Huang1, Bin Han Lo1
China Medical University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
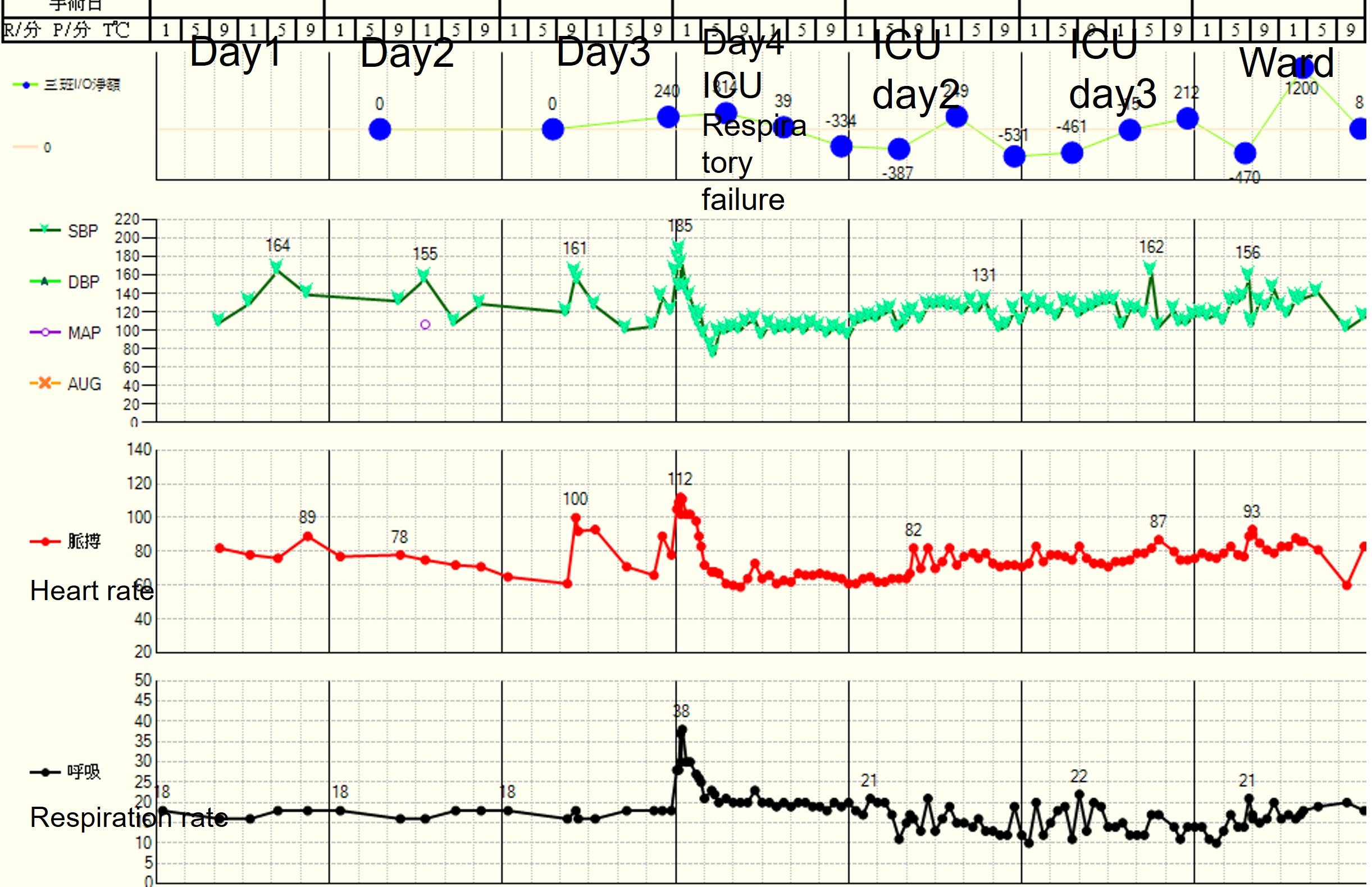
The 88-year-old male with history of hypertension, type 2 diabetes melitus, admitted for short of breath for 2 weeks. Dyspnea on exertion, mild orthopnea, increased body weight with 3 kilograms in one month and edema of legs has been noted. Phyiscal examination revealed crackles over lungs, regular heart beats with systolic murmur and pitting edema 3+. 1 1361087

Relevant Test Results Prior to Catheterization
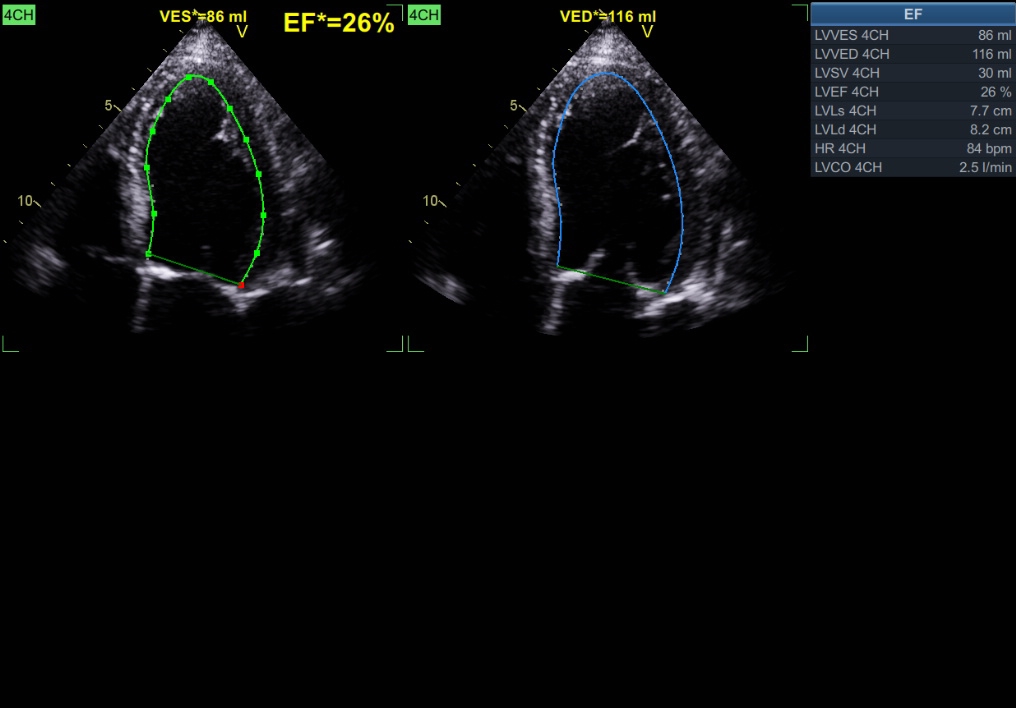
Chest radiography revealed pulmonary edema and pleural effusion. Echocardiography revealed global hypokinesia with impaired LV contractility (EF: 25%) and dilated LV. Dobutamine stress echocardiography for viable myocardium of LAD territory . The laboratory data revealed peak cTnI: 0.35ng/ml and NT-pro BNP:3267 pg/ml, Cr: 0.92 mg/dL. Aortic CT reveal stenosis of right common iliac artery and severe calcified aorta.


Relevant Catheterization Findings
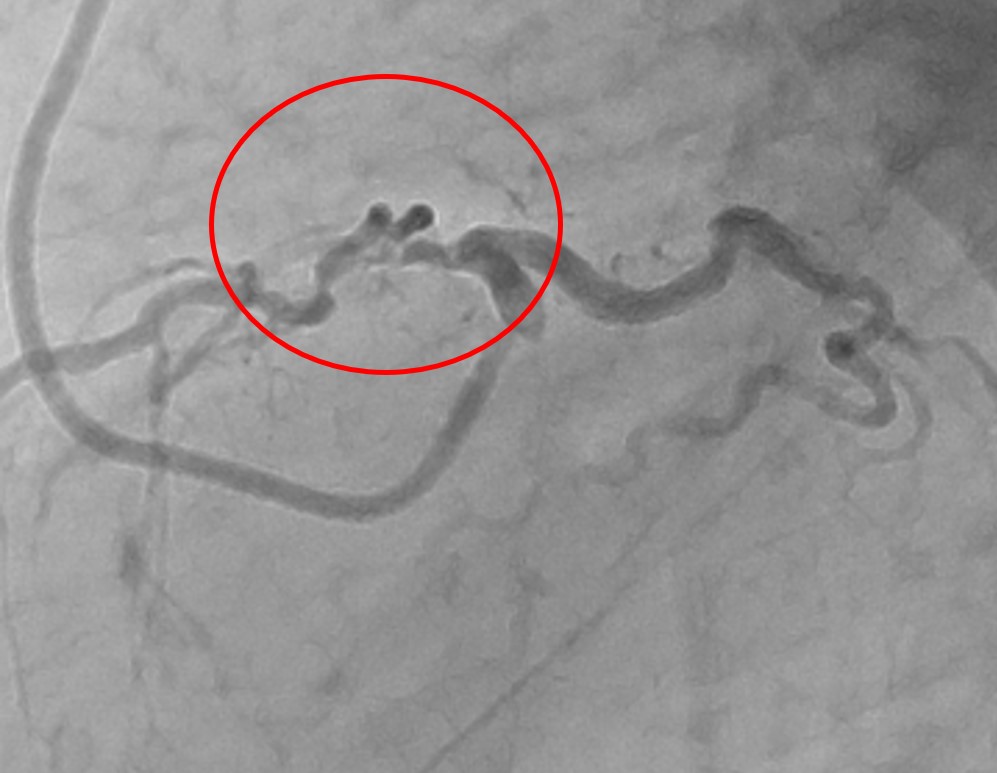
The coronary angiography revealed diffuse calcification and tortous vessel: 90% stenosis of LM ostium, 60% stenosis of distal LM, 80% stenosis of LAD ostium, 80% stenosis of proximal and distal LAD. 70% stenosis of distal LCX. Severe calcification, ostial lesion of RCA, 95% stenosis of proximal RCA, 80% stenosis of mid RCA and functional occlusion of PDA. Collateral branch from LAD septal branch to PDA. There was also severe stenosis of right subclavian artery.


Interventional Management
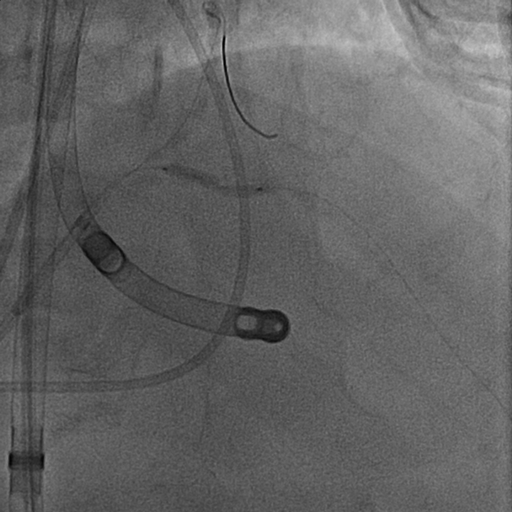
Procedural Step
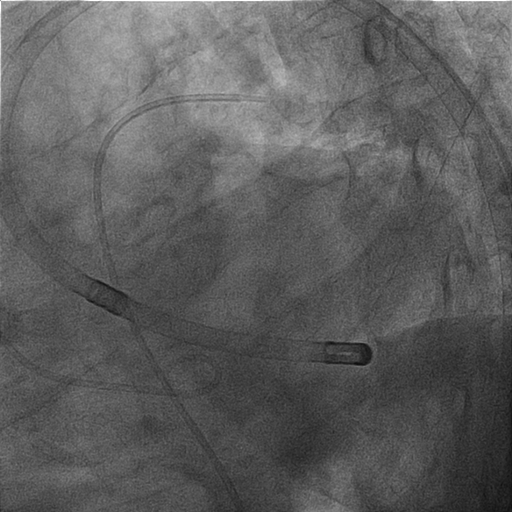
The right-sided cardiac catherization with Bal-Wedge 6Fr. was used for PCWP monitoring and cardiac output before and after procedure. C.O was 3.61 L/min at first. The final C.O. was 3.3L/min. Intervention Procedure: The iVAC 2.0L introduced by safari wire to LV via LFA by 18Fr sheath. LCA was engaged with a 7Fr. EBU 3.75 and the LM-LAD lesion was crossed with SION blue. LCX was crossed with Runthrough.. By GL 5.5Fr, LAD lesion dilated with Euphora 2.5/30 at 8-10 bars, NC 2.5/20 rupture at 20 bars over d-LM. Mid-LAD dilated by NC 2.5/12 at 12-20 bars, NC 2.0/12 at 20 bars. SynergyXD 2.5/48 deployed over p-miLAD at 8 bars. Dilated with NC 2.5/12 at 17-22 bars. LM-pLAD was dilated by Euphora 2.5/30 at 12 bars, Euphora 2.5/20 at 10 bars. SynergyXD 3.5/38 was deployed from osLM-pLAD at 14 bars and distal LM dilated with NC Emerge 4.5/8 at 14-16 bars. Rewired LCX via SASUKE and m -LAD dilated with NC 3.5/12 at 12-20 bars after IVUS. NC 2.25/12 dilated strut and LAD-LCX KBT with NC 3.5/12 and NC 2.5/12 at 8-10 bars. POT by NC 5.0/8 at 12-18 bars. LAD dilated by NC 3.5/12 at 20-22bars, NC 3.0/12 at 12-22 bars. GL 6Fr. was used. Onyx 2.0/12 deployed at 6-16 bars for edge dissection and dilated with NC 2.5/12 at 8-22 bars. The final blood flow was TIMI 3

Case Summary
Managing complex cases of critical lesion in acute phase with severe left ventricular dysfunction presents challenges for the patient and operator. Meticulous planning (heart team), comprehensive evaluation by risk assessmen (clinical factors and technical feasibility) and image study, the judious use of mechanical circulatory support depending on their varying capabilities and the specific needs of patient. The PulseCath iVAC2L offer tailored support for patients undergoing high-risk interventions, with distinct characteristics that enhance cardiac output support. Real-time monitoring with right-heart catheterization also enhancing procedural stability.