
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-148
Unraveling the Loop: Successful Resolution of a Rare and Complex Intra-Aortic Balloon Pumping Complication Without Surgery
By Hiroto Tanaka, Keiichiro Yamane, Soichiro Enomoto, Hirokazu Kondo, Toshihiro Tamura
Presenter
Hiroto Tanaka
Authors
Hiroto Tanaka1, Keiichiro Yamane1, Soichiro Enomoto1, Hirokazu Kondo1, Toshihiro Tamura1
Affiliation
Tenri hospital, Japan1,
View Study Report
TCTAP C-148
Coronary - Complication Management
Unraveling the Loop: Successful Resolution of a Rare and Complex Intra-Aortic Balloon Pumping Complication Without Surgery
Hiroto Tanaka1, Keiichiro Yamane1, Soichiro Enomoto1, Hirokazu Kondo1, Toshihiro Tamura1
Tenri hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 65-year-old female with a medical history significant for diabetes mellitus, hypertension, dyslipidemia, and prior percutaneous coronary intervention (PCI) to the #7 coronary segment presented with progressively worsening exertional chest pain that began in January 2024. She also had known stenosis in the #12 and RCA, managed with pharmacological therapy. Physical examination revealed a height of 163 cm, weight of 79 kg, and a BMI of 29.8. Heart sounds were normal.
Relevant Test Results Prior to Catheterization
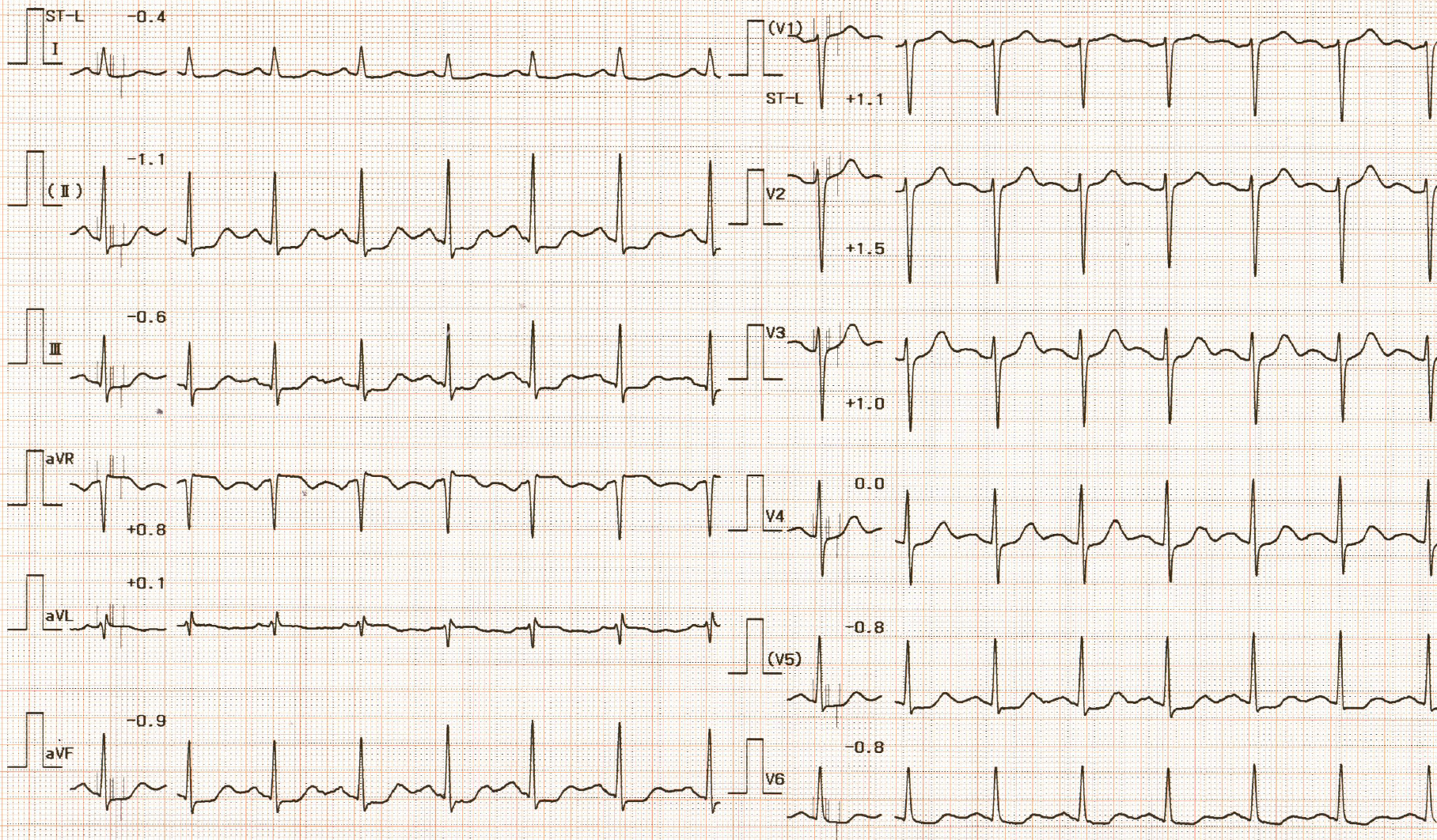
Resting electrocardiography revealed ST-segment depression in leads II, III, aVF, and V4-V6.
Relevant Catheterization Findings
Interventional Management
Procedural Step
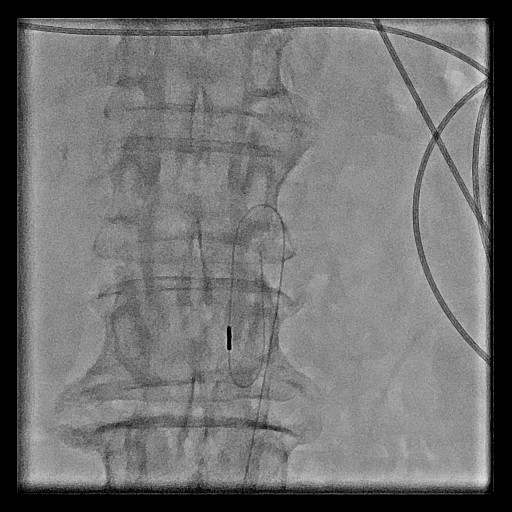
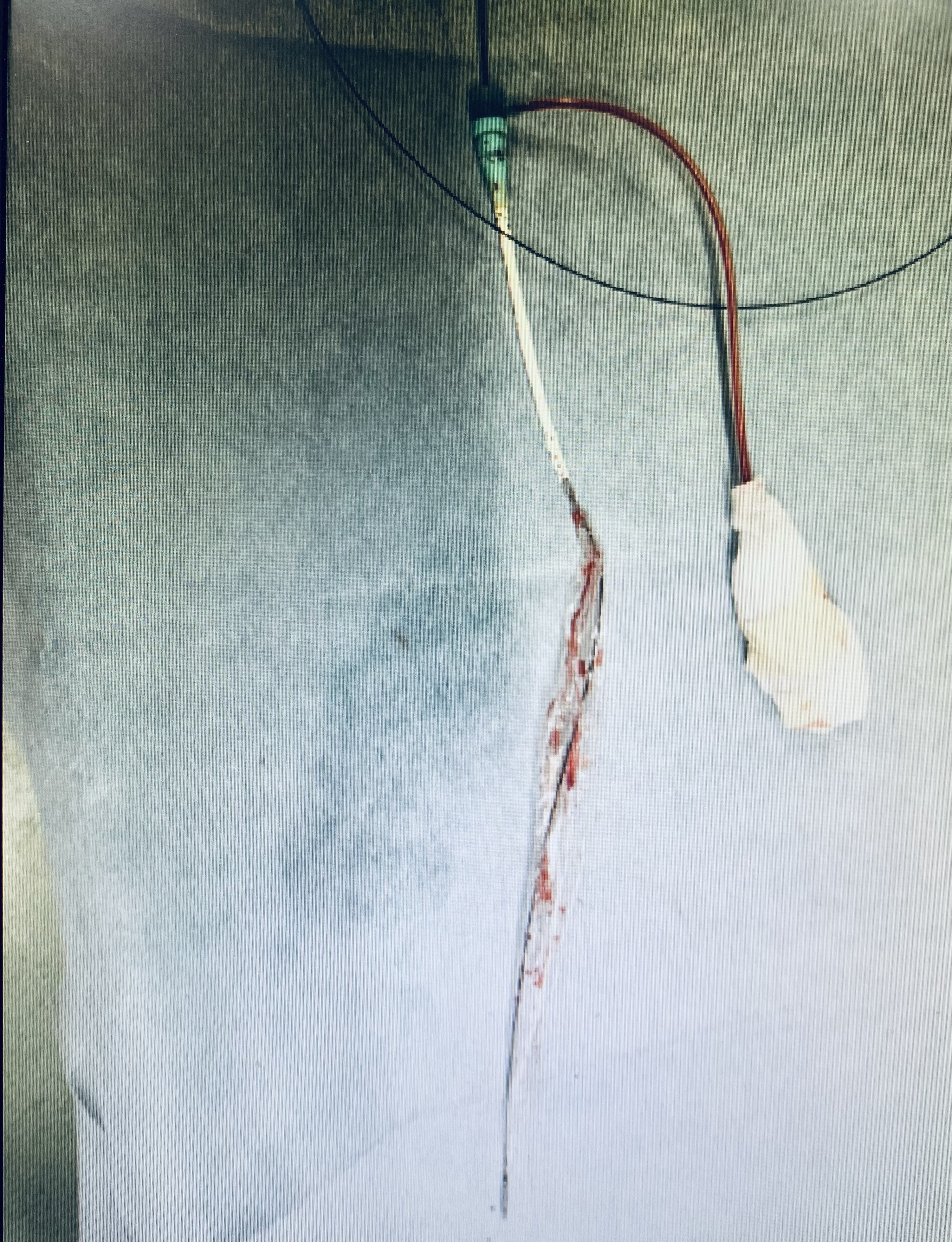
Emergency coronary angiography revealed three-vessel disease. The management plan involved stabilizing hemodynamics with intra-aortic balloon pumping (IABP) placement, followed by elective coronary artery bypass grafting. The IABP was deployed successfully from the right femoral artery (FA) . However, after patient transfer for CT imaging, frequent alarms prompted reassessment. CT and fluoroscopy revealed caudal displacement of the IABP tip. To facilitate repositioning of the IABP, a guidewire was introduced; however, it failed to traverse the caudal tip of the balloon, instead exhibiting an abnormal trajectory. Upon further advancement, it became evident that the caudal portion of the balloon had formed a loop. Manual attempts to retract the IABP into the sheath achieved partial retrieval, but the loop persisted. Radial or brachial artery access and snare-assisted loop release were considered but deprioritized to maintain IABP placement. A 6 Fr guiding sheath was introduced via the left FA, contralateral access, and intravascular ultrasound (IABP) confirmed a common FA diameter of approximately 6 mm. Balloon inflation was utilized to stabilize the cranial segment of the IABP balloon, enabling controlled traction on the caudal portion to facilitate its removal. A 5.0×40 mm balloon inflated at 2 atm enabled partial IABP advancement, though the loop remained. Full resolution was achieved by inflating the balloon to 6 atm, allowing complete retrieval of the IABP into the sheath.

Case Summary
This case highlights a rare complication of IABP malfunction due to loop formation. Successful resolution was achieved through an approach combining contralateral access, IVUS guidance, and balloon anchor. Contributing factors likely included catheter deformation due to patient obesity, and displacement of the catheter during bed transfers for CT imaging. The significance of this case lies in the effective management of a complex device-related complication without the need for surgical intervention, underscoring the importance of advanced bailout techniques in similar scenarios.