
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-072
A Case of a Wire That Passed Outside the Stent During CTO PCI of a Stent Occlusion Successfully Recaptured in the True Lumen Using IVUS Guided Rewiring and Tip Detection ADR Techniques
By Takayuki Shimmura, Kei Kawai, Kazuhiro Ashida
Presenter
Takayuki Shimmura
Authors
Takayuki Shimmura1, Kei Kawai1, Kazuhiro Ashida1
Affiliation
Seirei Yokohama Hospital, Japan1,
View Study Report
TCTAP C-072
Coronary - Complex PCI - CTO
A Case of a Wire That Passed Outside the Stent During CTO PCI of a Stent Occlusion Successfully Recaptured in the True Lumen Using IVUS Guided Rewiring and Tip Detection ADR Techniques
Takayuki Shimmura1, Kei Kawai1, Kazuhiro Ashida1
Seirei Yokohama Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
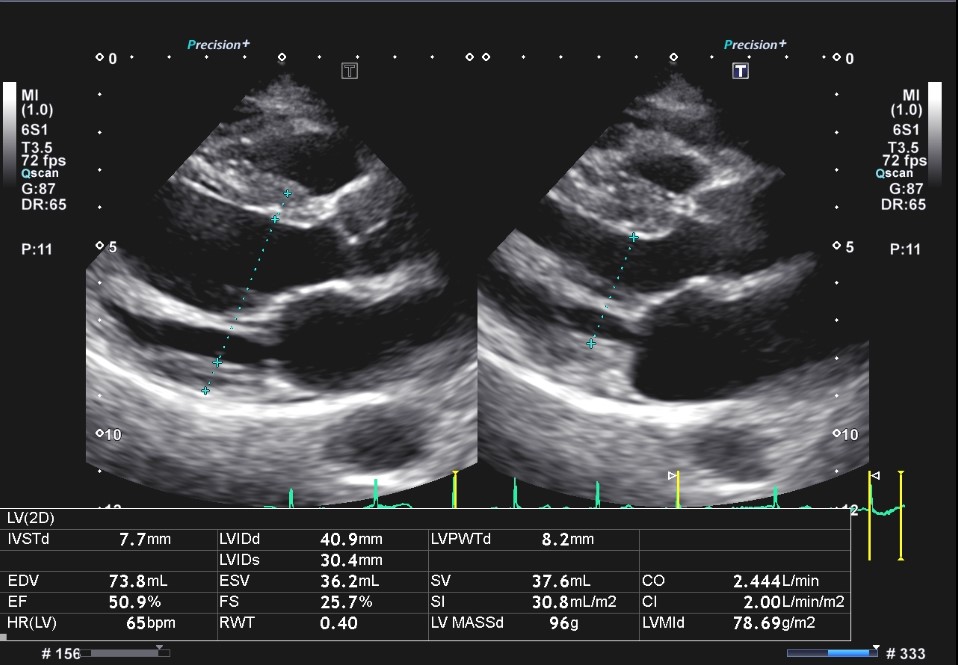
A 70's woman with a history of dyslipidaemia and hypertension underwent coronary CT after treatment for heart failure, which showed a CTO lesion in the RCA. Echocardiographic EF was 39 %, with asynergy in the inferior wall.
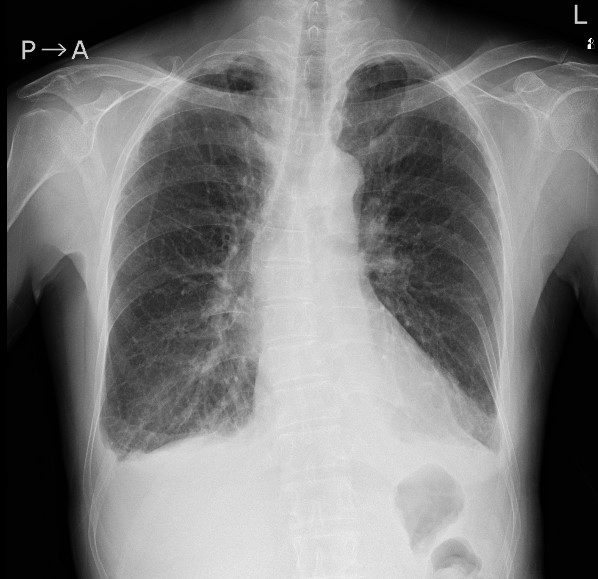
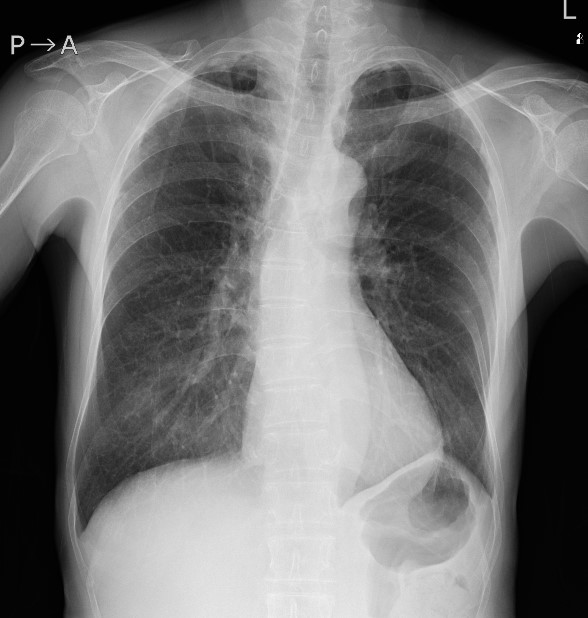
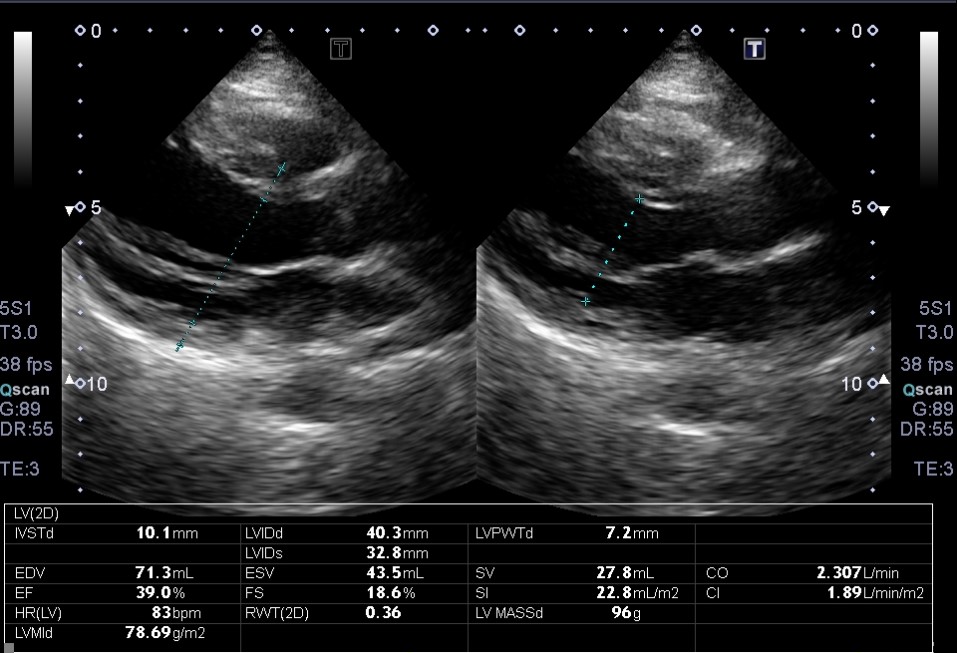
Relevant Test Results Prior to Catheterization
PCI was subsequently performed, with four DES put from proximal to distal RCA.A follow-up coronary CT angiography six months later showed a CTO lesion of the stent occlusion. Echocardiographic EF had improved 39 % to 50 %, and the viability of the inferior wall was judged to be preserved, so the patient underwent re-PCI for in-stent CTO.
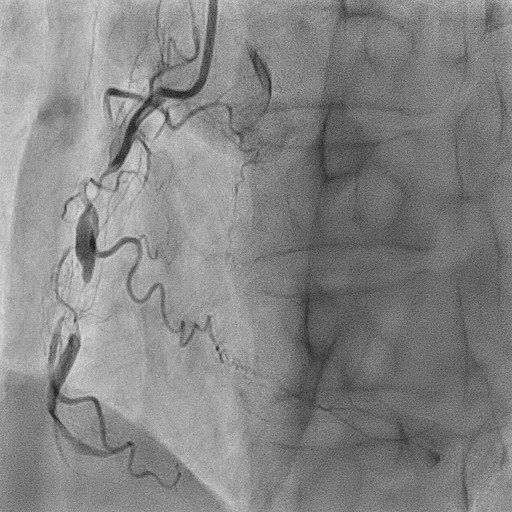
Relevant Catheterization Findings
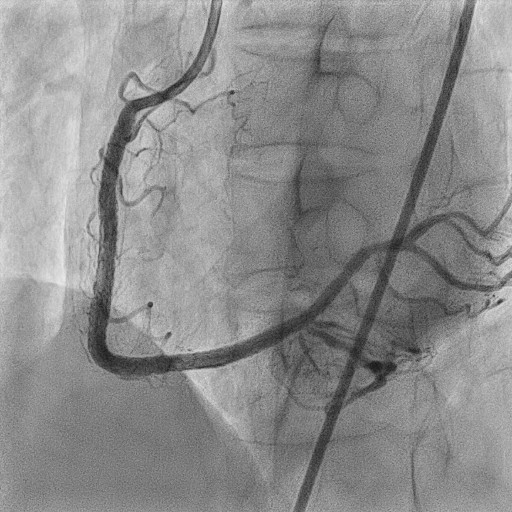
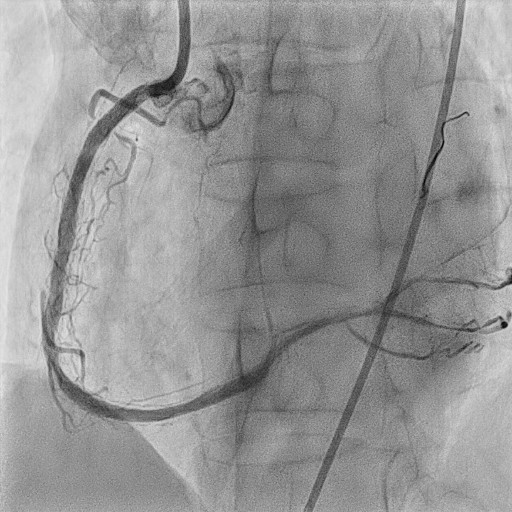
The CAG showed slight contrast seepage at the CTO entrance, so wire manipulation was initiated to landmark the stent on fluoroscopy and track the microchannel.
Interventional Management
Procedural Step
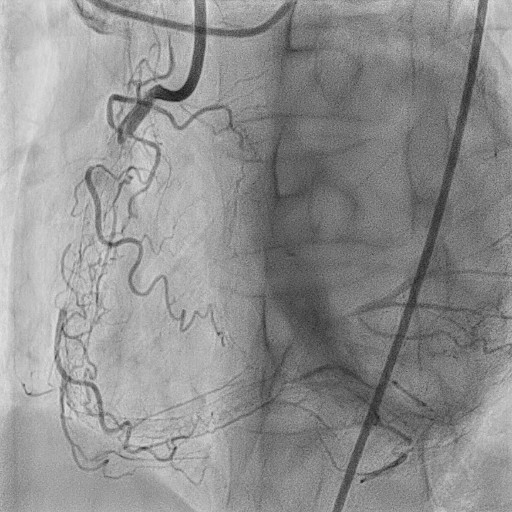
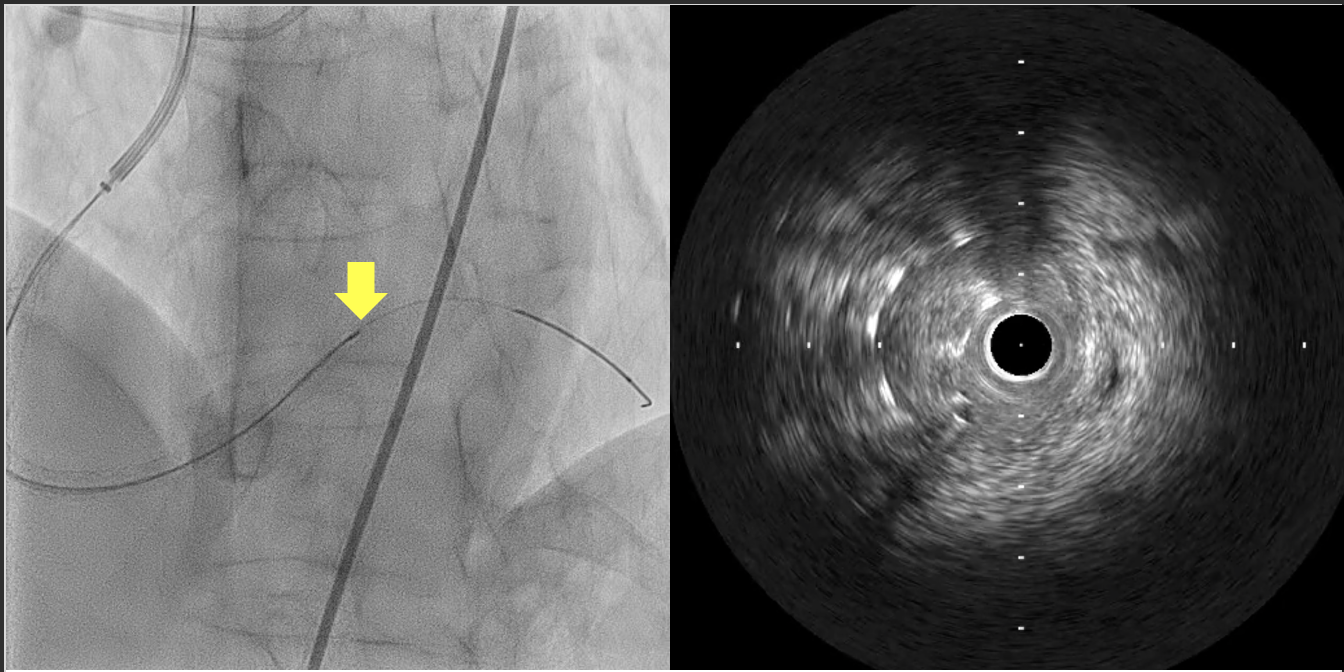
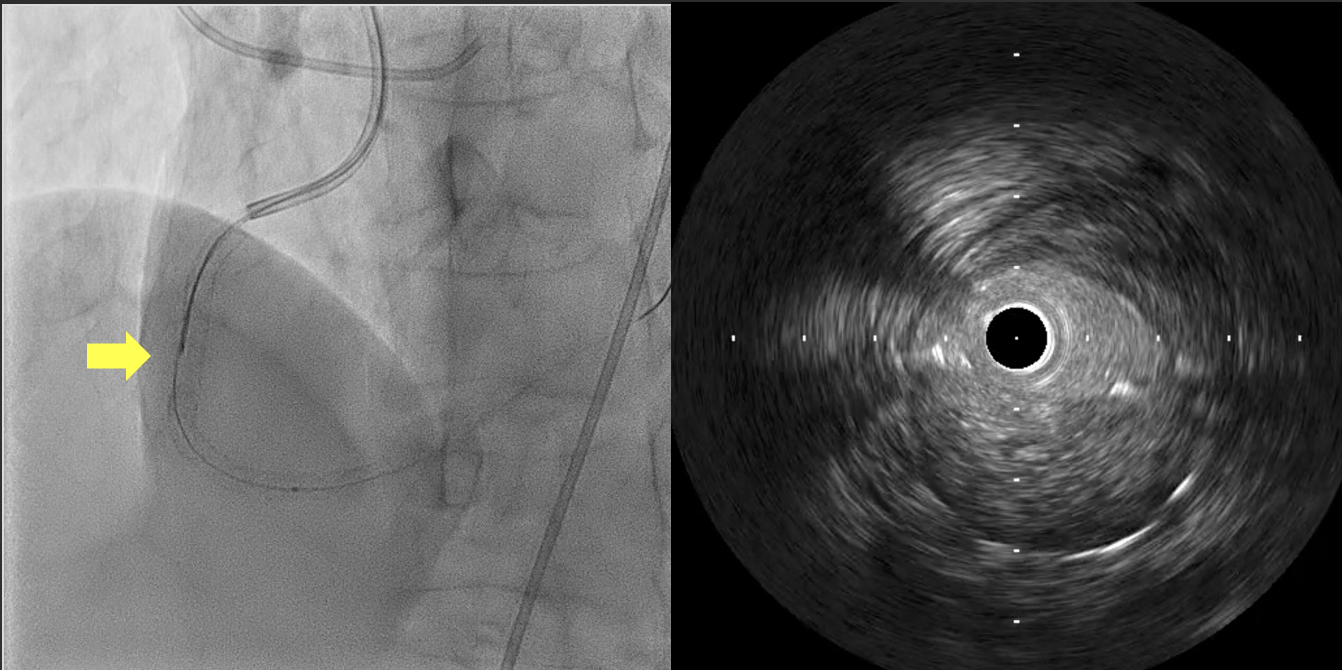
A polymer jacket wire was advanced while confirming previous stents by fluoroscopy from multiple directions, and although the wire advanced to near the CTO exit, but the microcatheter was difficult to pass at two points in the mid and distal RCA. The microcatheter was successfully passed by gradual dilation with a small diameter balloon. After the guide wire and microcatheter passage, IVUS showed that the two sites where the microcatheter was difficult to pass passed outside the previously implanted stent. The distal part was attempted to be rerouted by IVUS guided rewiring and the true lumen was captured. Proximally, the true lumen was successfully captured using the Tip detection ADR technique, and the guidewire was ultimately successfully passed through the true lumen.
Case Summary
IVUS guided rewiring and tip detection ADR have received attention in recent years as effective techniques to pass CTO lesions.We report a case in which the true lumen was successfully recaptured using IVUS guided rewiring and tip detection ADR techniques after a wire had passed outside the stent during CTO treatment of a stent occlusion, with some discussion of the literature.