
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-156
Nightmare Perforations in a Case of Chronic Total Occlusion Percutaneous Coronary Intervention
By Florimond Joseph Jr. Garcia
Presenter
Florimond Joseph Jr. Garcia
Authors
Florimond Joseph Jr. Garcia1
Affiliation
The Medical City, Philippines1,
View Study Report
TCTAP C-156
Coronary - Complication Management
Nightmare Perforations in a Case of Chronic Total Occlusion Percutaneous Coronary Intervention
Florimond Joseph Jr. Garcia1
The Medical City, Philippines1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
We are presented with a 74 year old, female, Filipino who is a known hypertensive, dyslipidemic and with a history of multiple CVD infracts. She came in with a chief complaint of cough with dyspnea for 3 days. On arrival at the emergency room, the patient was in shock and in respiratory distress. She was managed as ACS NSTEMI and angiogram revealed 3 Vessel Disease. PCI of the LAD and LCX was performed and Complex CTO procedure of the RCA was planned after 2 days.
Relevant Test Results Prior to Catheterization
Cardiac Troponin I was elevated. Normal LV cavity with hypokinesia of the mid ventricular walls and akinetic apical walls. Left Ventricular ejection fraction was reduced at 35-40%. 12L ECG showed non-specific ST-T wave changes. Coronary Angiogram of the LAD and LCX post PCI showed good stent apposition with TIMI III Flow and no perforations or dissections.
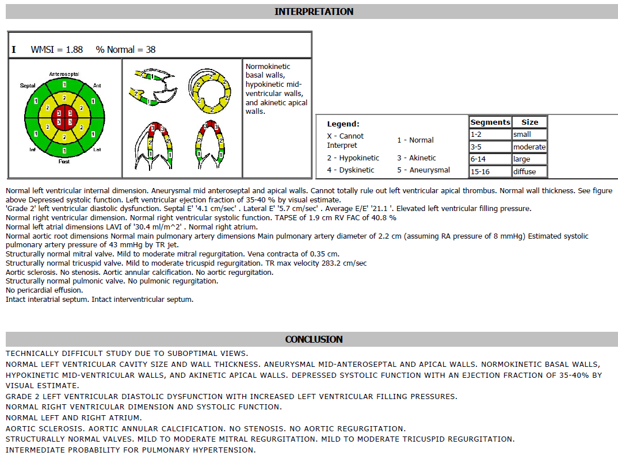
Relevant Catheterization Findings
The left main artery is absent. The LAD arises from its own ostium, is a good sized type III vessel with a 99% mid segment thrombotic occlusion. The LCX arises from its own ostium and has a 70% proximal thrombotic occlusion with calcifications. The distal LCX is diffusely diseased with a 60% occlusion. The RCA is totally occluded at the ostium but visualized via left to right collaterals. Post PCI of the LAD and LCX shows good stent apposition with TIMI III Flow.
Interventional Management
Procedural Step
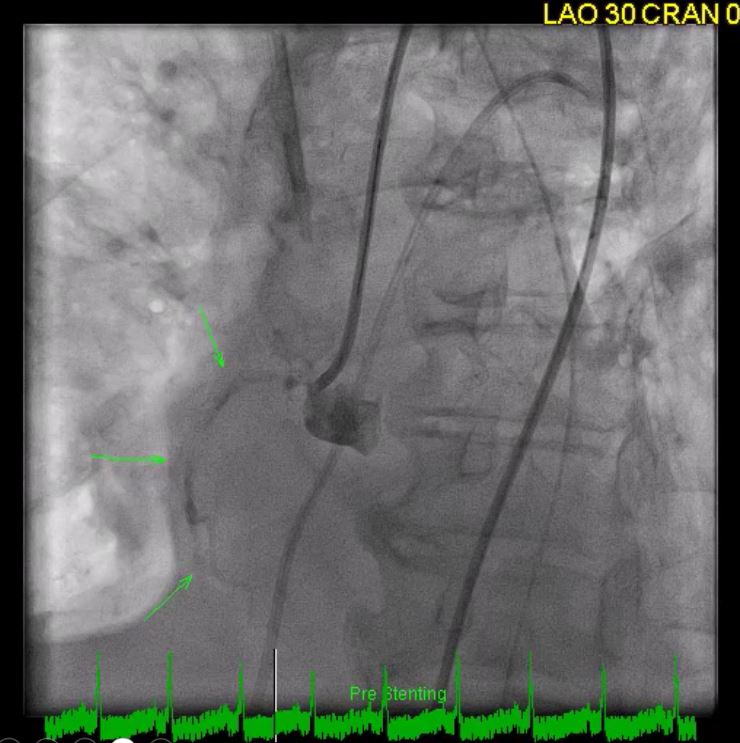
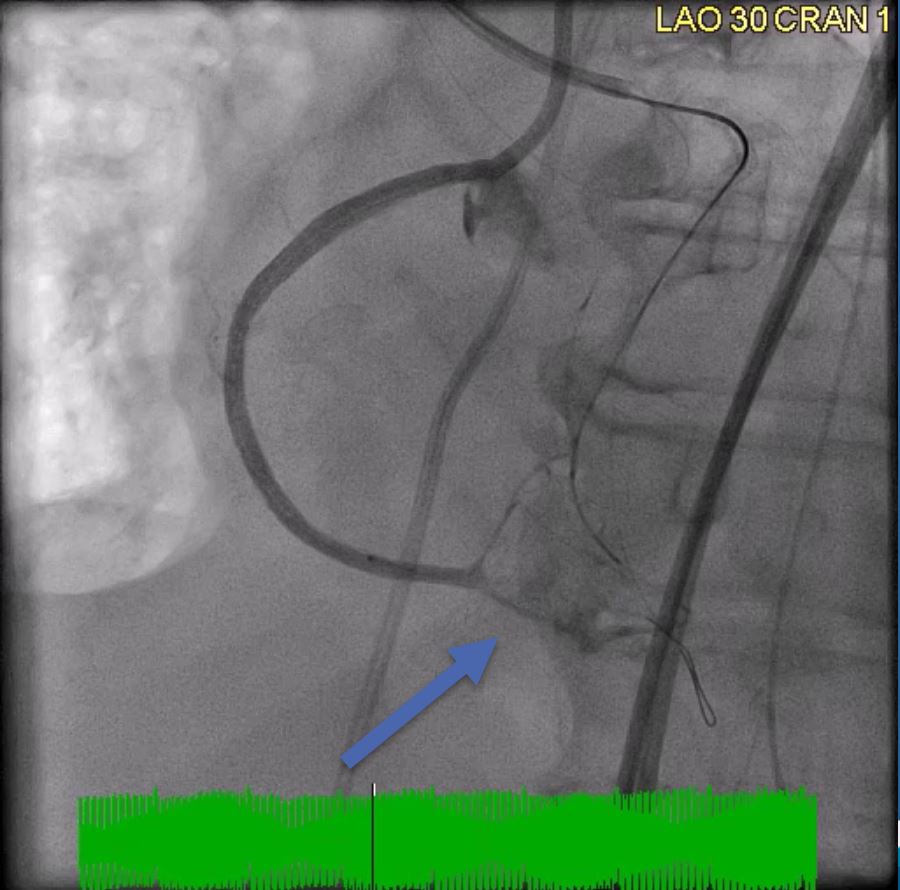
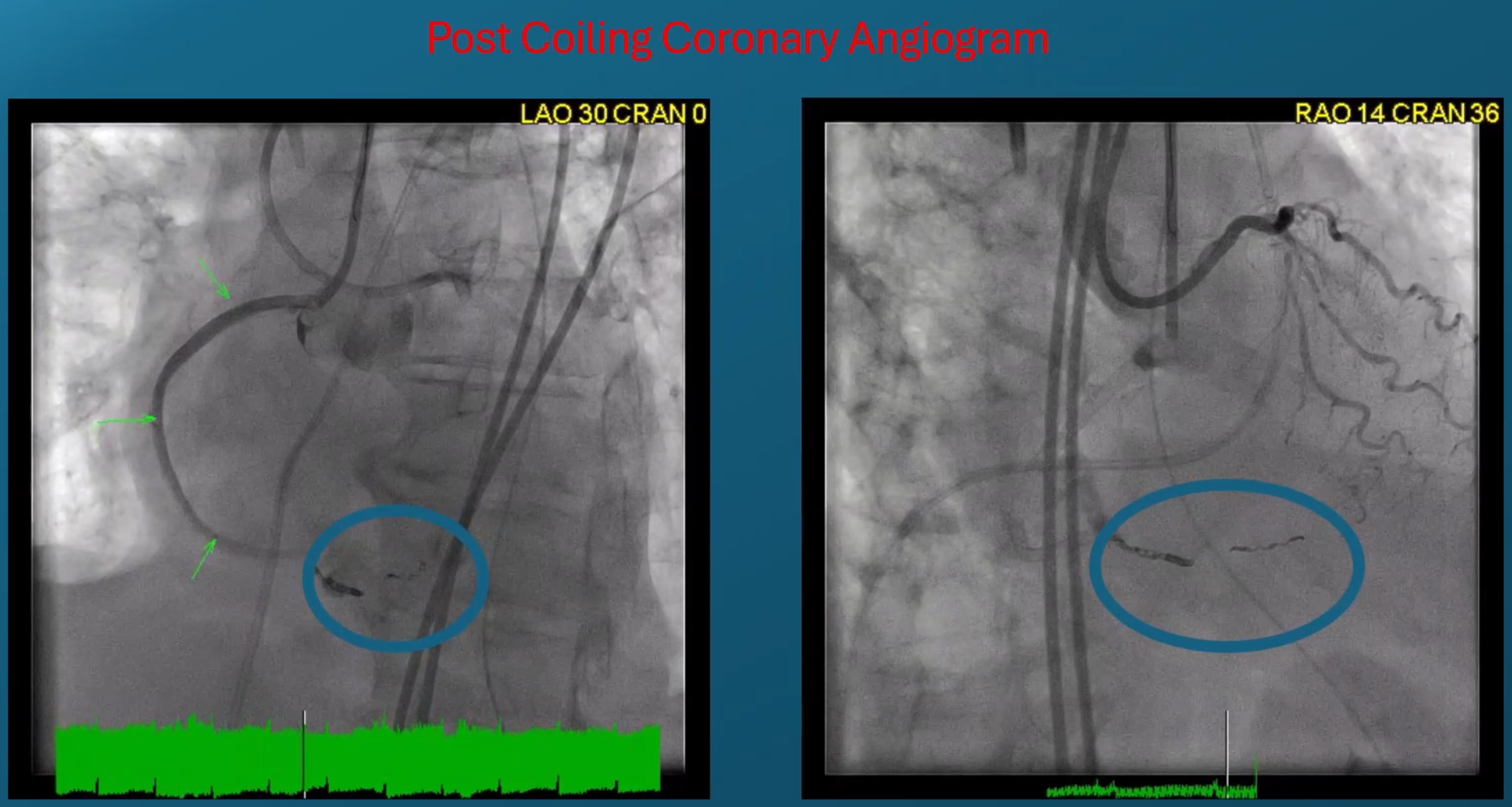
Antegrade PCI of the RCA was attempted but failed. We then shifted to retrograde PCI of the RCA and was successful. However, the patient developed shock and POCUS 2D echo showed development of moderate pericardial effusion with tamponade. On angiogram, there were multiple perforations seen at the septal collaterals and the posterior descending artery. Prolonged balloon inflation efforts were unsuccessful and there were no available small sized covered stents and would take 2 hours to arrive. The team decided to do coronary coiling of the perforations. Coronary coiling was successful with no progression of pericardial effusion and resolution of the hypotension was achieved.
Case Summary
Chronic total occlusion percutaneous coronary intervention has many possible complications. Interventional cardiologists, though experienced, should be knowledgeable on these complications despite their rarity. Bailout strategies should always be in place prior to doing the procedure by planning well and properly knowing the character of equipment used. The team should always be aware of the available tools and equipment for these possible complications.