
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-106
Challenging Intervention for Restenosis of Right Coronary Ostial Stent Excessively Overhanging to the Aorta
By Muhammad Husen Latif
Presenter
Muhammad Husen Latif
Authors
Muhammad Husen Latif1
Affiliation
Siloam Hospital Makassar, Indonesia1,
View Study Report
TCTAP C-106
Coronary - Complex PCI - In-Stent Restenosis
Challenging Intervention for Restenosis of Right Coronary Ostial Stent Excessively Overhanging to the Aorta
Muhammad Husen Latif1
Siloam Hospital Makassar, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 54-year-old female patient presents at emergency room with a chief complaint of typical sharp-substernal chest pain for the past six hours. She has a history of percutaneous coronary intervention (PCI) three years ago due to acute coronary syndrome (ACS) and has been on medical treatment since then. Upon physical examination, the patient is stable, with all findings within normal limits.
Relevant Test Results Prior to Catheterization
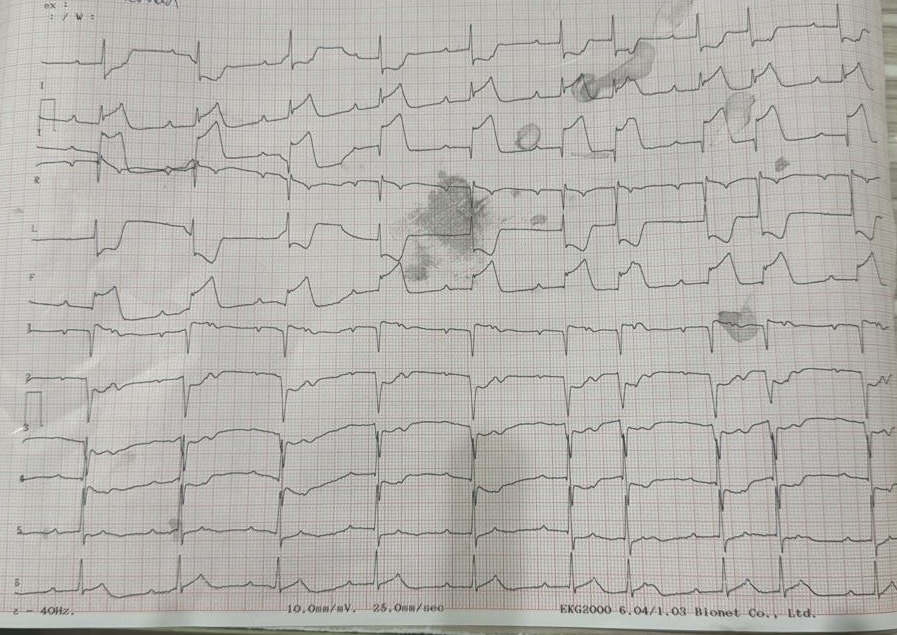
Electrocardiogram shows ST-segment elevations at inferior leads and lab results show a positive troponin test, indicating myocardial injury. Given her symptoms, ECG, and lab results, a coronary angiography is planned to assess the current state of her coronary arteries.
Relevant Catheterization Findings
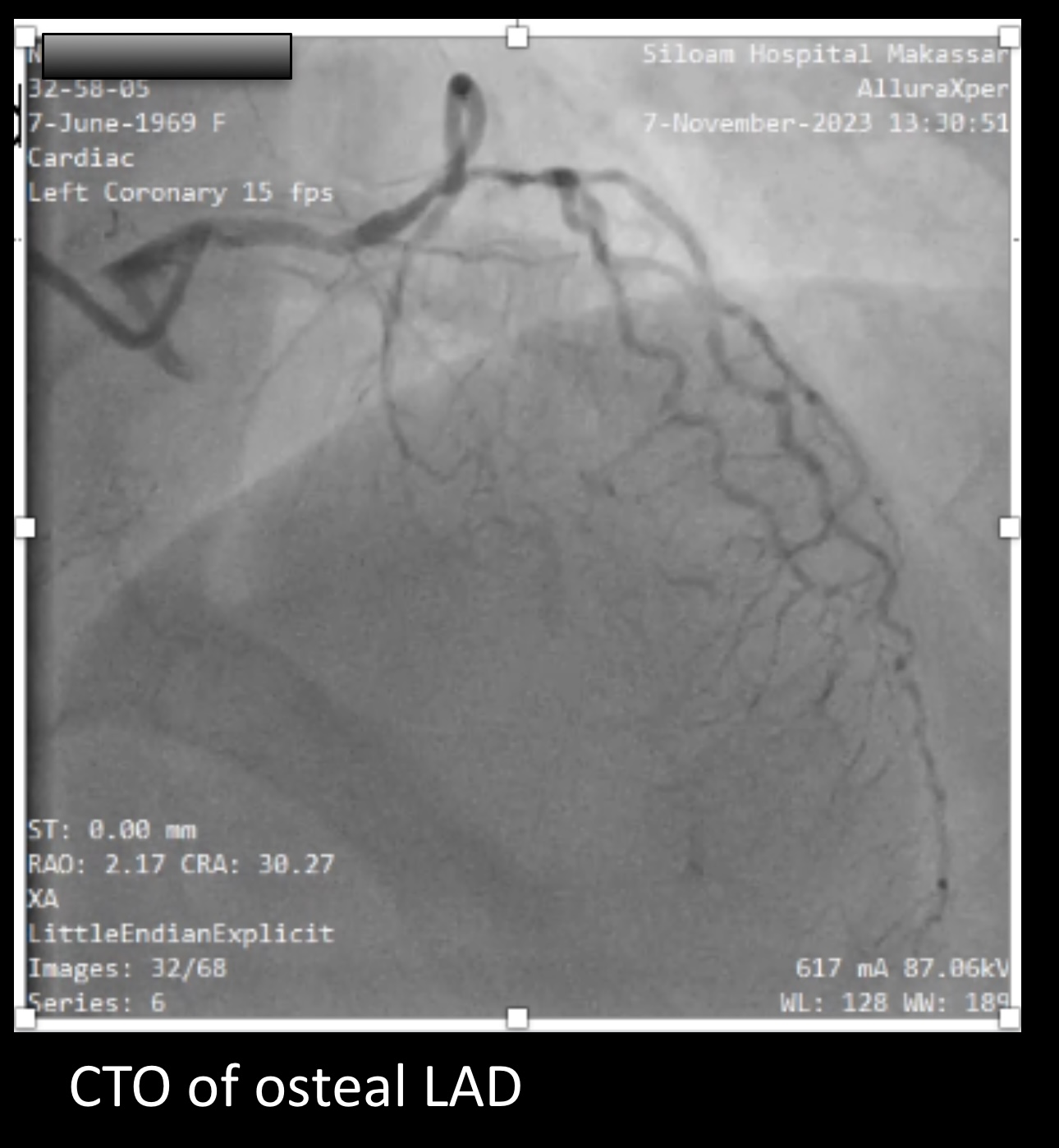
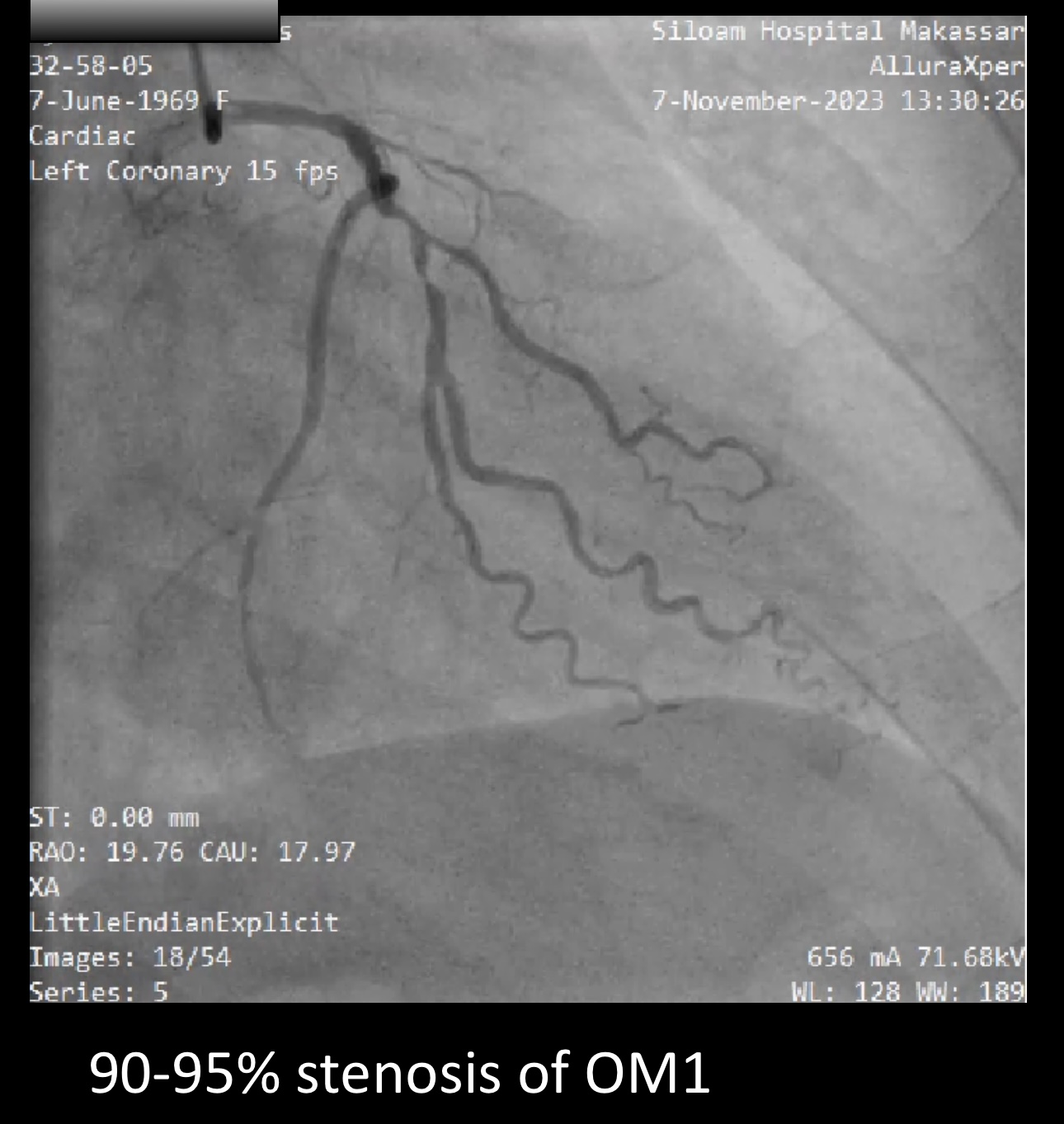
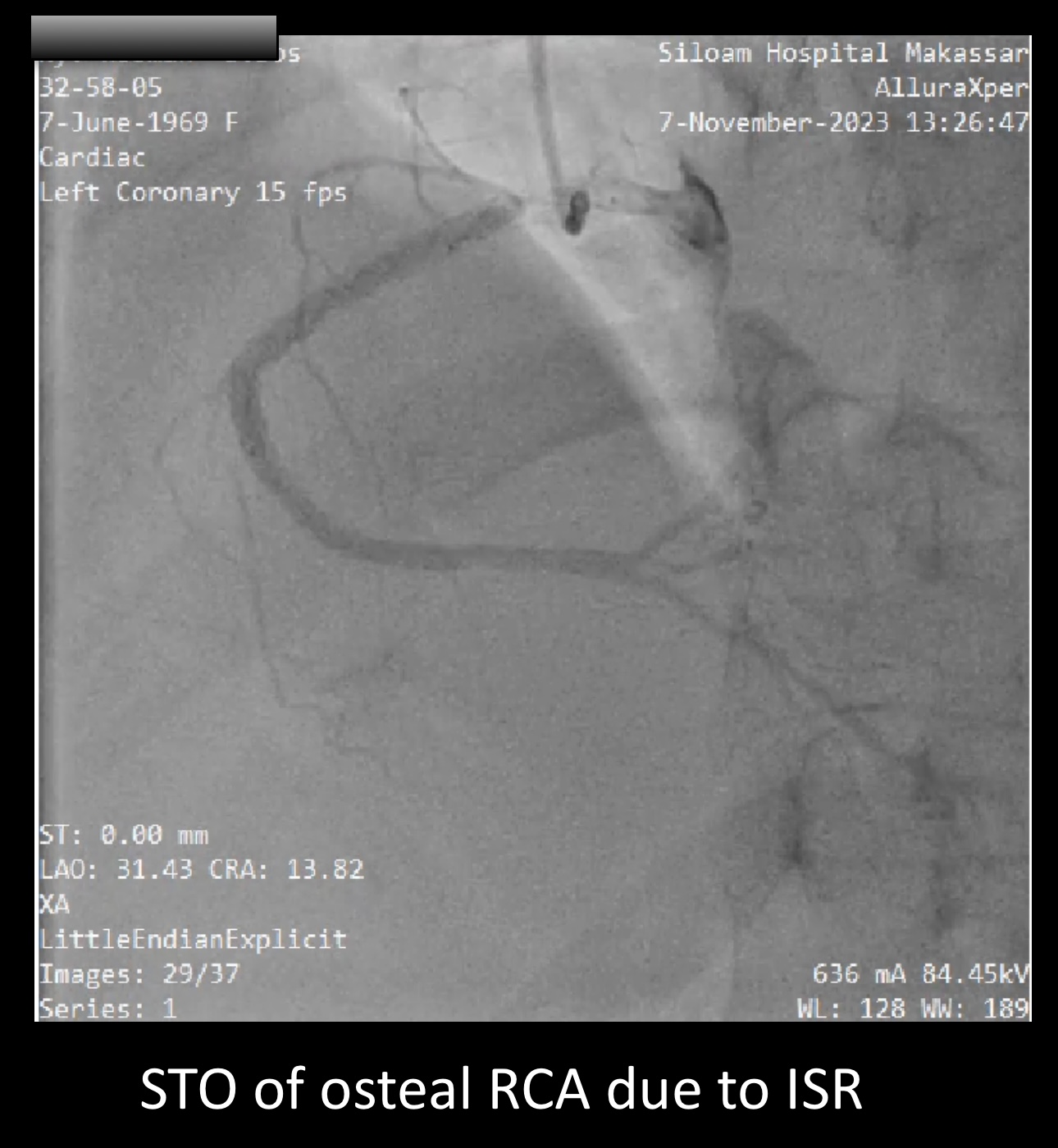
The angiographic examination was performed via transradial access. The left main (LM) artery appeared normal. However, a chronic total occlusion (CTO) was identified at the ostial segment of the left anterior descending artery (LAD). Additionally, there was a 95% stenosis lesion in the first obtuse marginal artery (OM1). Furthermore, subtotal occlusion was noted at the ostial right coronary artery (RCA), classified as In-Stent Restenosis (ISR) type II.
Interventional Management
Procedural Step
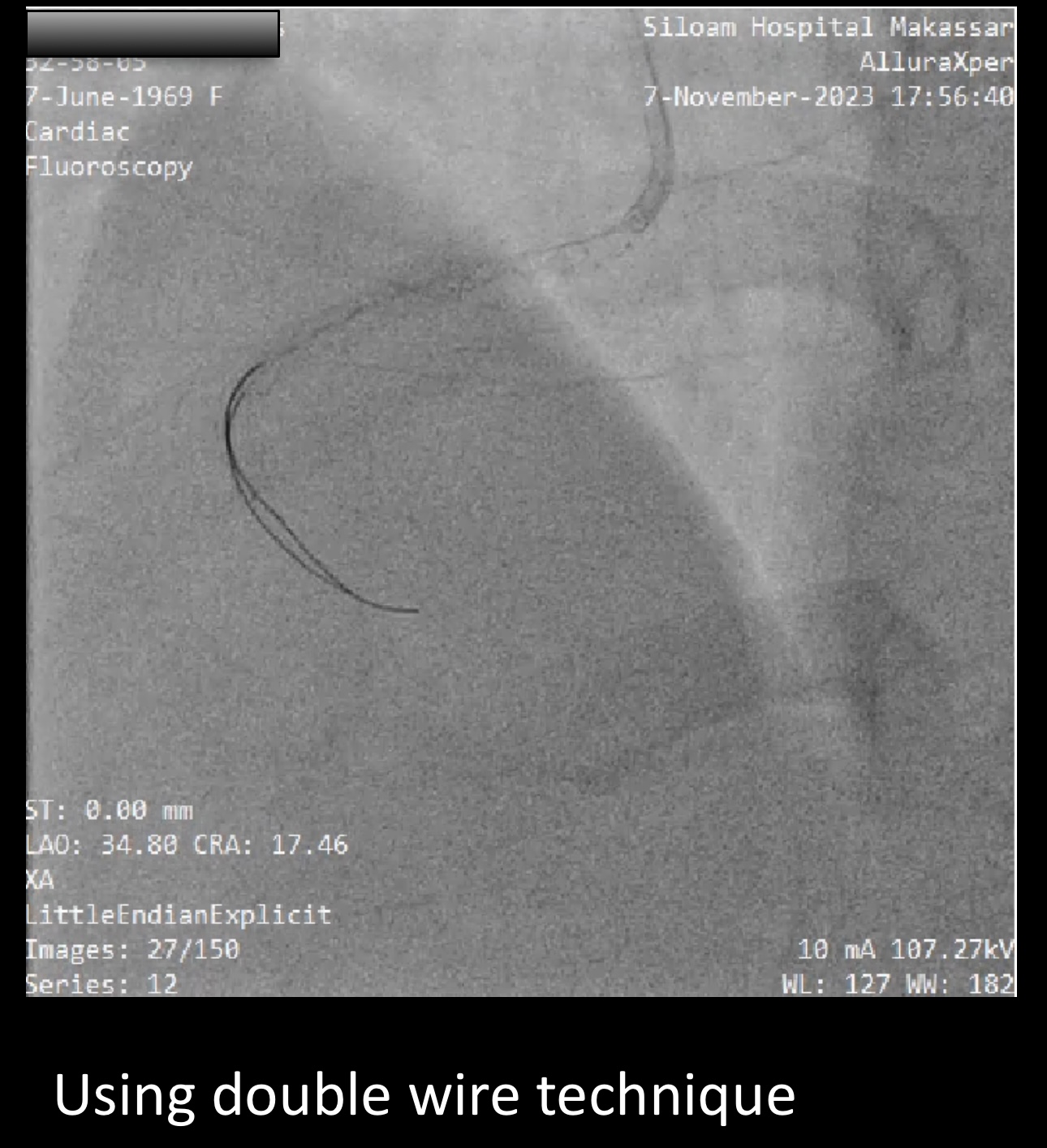
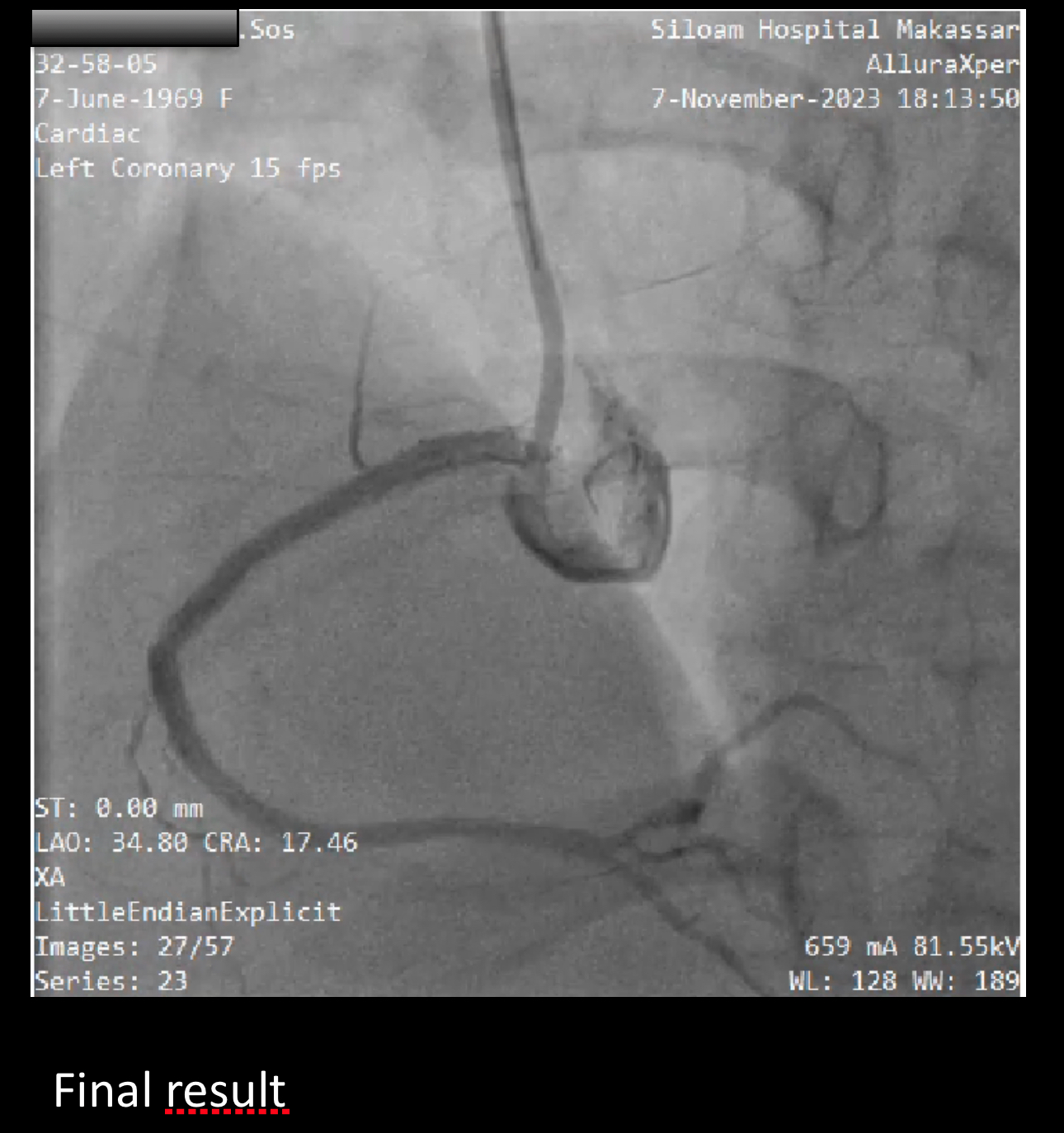
In this case of In-Stent Restenosis (ISR) in the ostial right coronary artery (RCA), we encountered significant challenges during the Percutaneous Coronary Intervention (PCI) procedure. Based on the clinical symptoms, electrocardiogram (ECG) findings, and angiographic results, we decided to proceed with PCI on the RCA. A subtotal stenosis lesion was observed at the ostial RCA, a complication resulting from the ISR of a PCI performed three years prior. The previous stent in the ostial RCA was noted to be partially overhanging into the aorta, complicating the cannulation of the RCA. Despite multiple attempts at cannulation maneuvers, we were unsuccessful. As a result, we opted for a double wire technique. Using a 6F TIG guiding catheter, we attempted to advance a floppy wire to the area of the stent strut located just anterior to the ostial RCA, which would serve as an anchor. The guiding catheter was positioned coaxially with the segment of the stent extending into the aorta, allowing us to maneuver a second wire past the ostial stent. After several attempts, we successfully advanced the second wire through the ostial stent, penetrating the stenotic lesion in the ostial of RCA and continuing into the distal of RCA. Subsequently, we prepared the lesion in the ostial RCA using a non-compliant balloon sized 2.0 mm x 15 mm. A stent measuring 3.5 mm x 9 mm was then deployed in the ostial RCA, and the section of the stent overhanging into the aorta was post-dilated (POT) up to 4 mm.

Case Summary
Performing Percutaneous Coronary Intervention on osteal lesions presents unique challenges, primarily due to the necessity of ensuring that the deployed stent does not extend beyond the ostium. The presence of a stent overhanging in front of the ostial coronary artery complicates cannulation attempts for the subsequent PCI procedures. This case illustrates the importance of meticulous planning and technique, such as employing the double wire method, to navigate these difficulties and ensure successful lesion treatment while minimizing complications. Proper management of osteal lesions is crucial for optimal outcomes in interventional cardiology.