
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-030
Optimizing Thrombectomy Outcomes in Percutaneous Coronary Intervention: The Role of Specialized Catheters in Treating Resistant Coronary Thrombi
By Ching-Ping Chao, Yi-Ching Lin, Wen-Po Chuang
Presenter
Wen-Po Chuang
Authors
Ching-Ping Chao1, Yi-Ching Lin1, Wen-Po Chuang1
Affiliation
Far Eastern Memorial Hospital, Taiwan1,
View Study Report
TCTAP C-030
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Optimizing Thrombectomy Outcomes in Percutaneous Coronary Intervention: The Role of Specialized Catheters in Treating Resistant Coronary Thrombi
Ching-Ping Chao1, Yi-Ching Lin1, Wen-Po Chuang1
Far Eastern Memorial Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
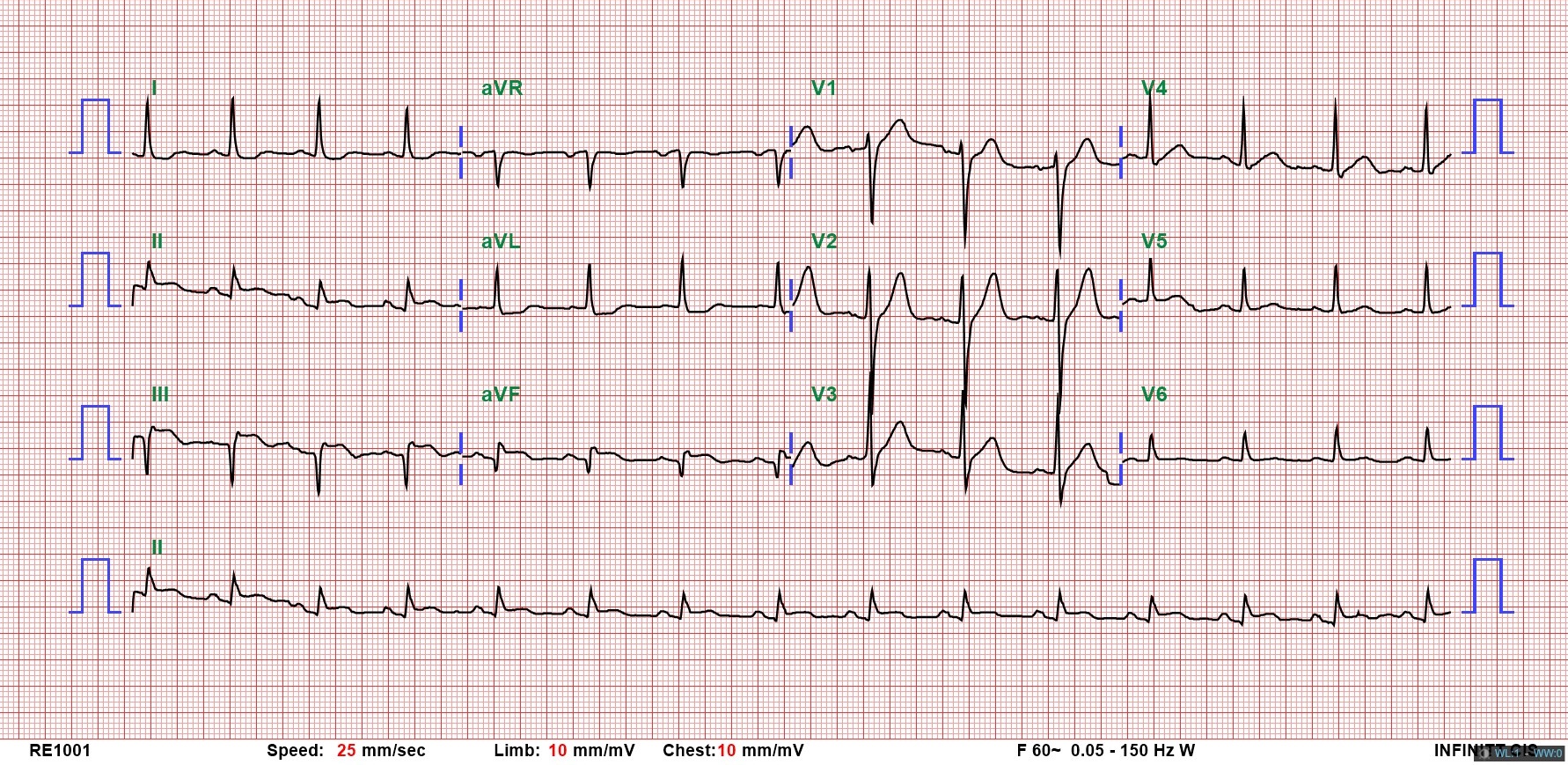
This 63-year-old male had coronary artery disease, status post angioplasty and stenting to the left anterior descending and right coronary artery (RCA). He presented to the ER with chest pain since the previous night. Examination showed stable vitals. ECG revealed sinus rhythm and Q-S pattern in leads II, III, and aVF. Elevated cardiac enzymes and echocardiography with fair ejection fraction without RWMA confirmed NSTEMI. He was admitted to the ICU, and coronary angiography planned.
Relevant Test Results Prior to Catheterization
In 2023, prior to the current admission, the patient was hospitalized for percutaneous coronary intervention (PCI) due to coronary artery disease. At that time, CAG revealed total occlusion of the mid-RCA. Consequently, plain old balloon angioplasty and stenting with a Resolute Onyx™ drug-eluting stent (4.5 mm × 30 mm; Medtronic, USA) were performed to the distal RCA and posterior descending artery. Additionally, ectasia of the left circumflex artery and RCA was observed.
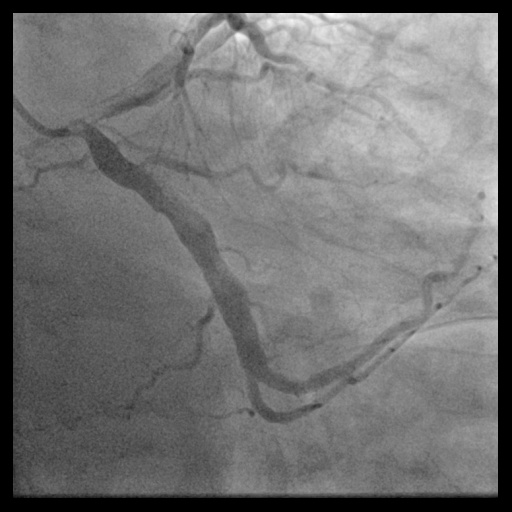
Relevant Catheterization Findings
Access via a 7 Fr in 6 Glidesheath Slender (Terumo, Japan) in the right radial snuffbox. CAG revealed total mid-RCA occlusion. Intracoronary Tirofiban was given. A Sion Blue ES wire (ASAHI, Japan) reached the distal RCA. Aspiration with Thrombuster II and ST01 catheters removed minimal debris. Thrombus fragmentation with Ryurei and Accuforce balloons and Pronto V4 achieved TIMI 2 flow, but thrombus persisted. The patient received Enoxaparin, dual antiplatelets, and Tirofiban infusion for 3 days.


Interventional Management
Procedural Step
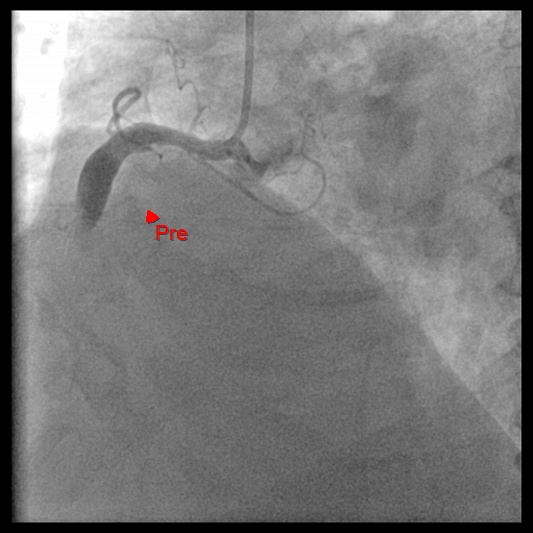
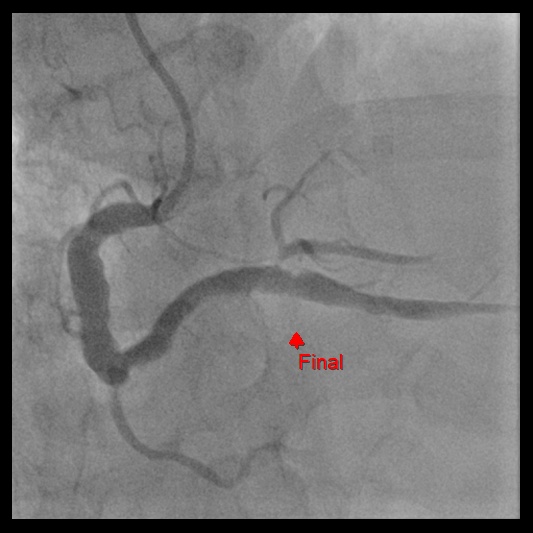
After 3 days of anticoagulation, follow-up CAG via the right radial artery with a 7 Fr in 6 Glidesheath Slender revealed a persistent thrombus along the RCA. A 7.0 Fr AL 1.0 Medtronic Launcher guiding catheter advanced an ASAHI Fielder FC 0.014” wire into the distal RCA. IVUS (Boston Scientific, USA) revealed extensive thrombus and an aneurysmal RCA segment. Regular aspiration catheters were ineffective, pushing thrombus away rather than aspirating it. A 5 Fr JR 4.0 catheter with an angulated tip enabled direct thrombus extraction. Continuous suction successfully removed a large elastic thrombus, which was extracted with the AL1 catheter. The sheath was replaced, and the guidewire reinserted. Repeated aspiration and thrombus fragmentation using a 5.0 mm x 15 mm NC Emerge balloon cleared the mid-RCA thrombus but failed for the distal thrombus. A 7.0 Fr KANEKA Thrombuster II catheter also failed to remove distal thrombus. A second vascular access via the right femoral artery with an 8 Fr Terumo Glidesheath Slender enabled use of the Penumbra ACE68 catheter (Penumbra Inc., Alameda, CA, USA), known for its large lumen and excellent trackability. The ACE68 catheter successfully aspirated the distal thrombus. To restore patency, a 5.0 mm x 12 mm Medtronic Resolute Onyx stent was deployed in the mid-RCA, followed by post-dilation with a 6.0 mm x 12 mm NC Emerge balloon at 20 atm. Final angiography confirmed TIMI grade 3 flow, achieving full reperfusion.



Case Summary
This case highlights the challenges of PCI in ACS with refractory thrombus, offering four key lessons. First, mechanical thrombectomy is crucial when thrombi resist pharmacologic treatment, requiring combined approaches. Second, a Terumo Glidesheath Slender 7 Fr in a 6 Fr sheath enables effective aspiration with a 7 Fr catheter from the right snuffbox, demonstrating radial access potential. Third, angulated catheters like JR 4.0 provide superior access to large, off-track thrombi in aneurysmal arteries. Finally, the Penumbra catheter, with its large lumen and excellent trackability, effectively removes distal thrombi when other methods fail, expanding its cardiovascular applications.