
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-232
Left Subclavian Artery Stenting Followed by DEB Angioplasty to Radial Artery to Palmar Arch
By Sridhar Kasturi, Pardha Saradhi Sivakoti
Presenter
Pardha Saradhi Sivakoti
Authors
Sridhar Kasturi1, Pardha Saradhi Sivakoti1
Affiliation
KIMS Sunshine Hospitals, India1,
View Study Report
TCTAP C-232
Endovascular - Other Endovascular Intervention
Left Subclavian Artery Stenting Followed by DEB Angioplasty to Radial Artery to Palmar Arch
Sridhar Kasturi1, Pardha Saradhi Sivakoti1
KIMS Sunshine Hospitals, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
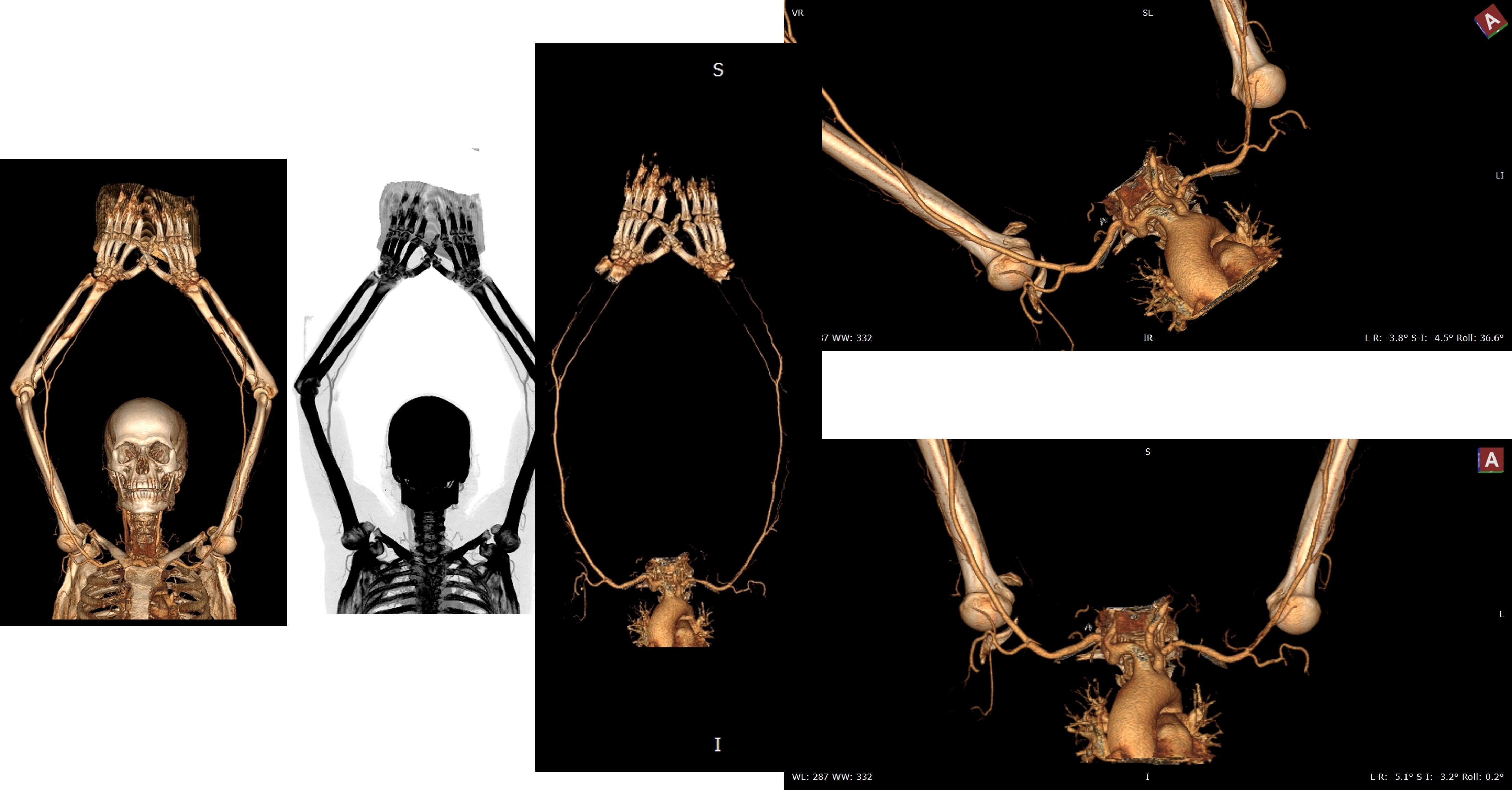
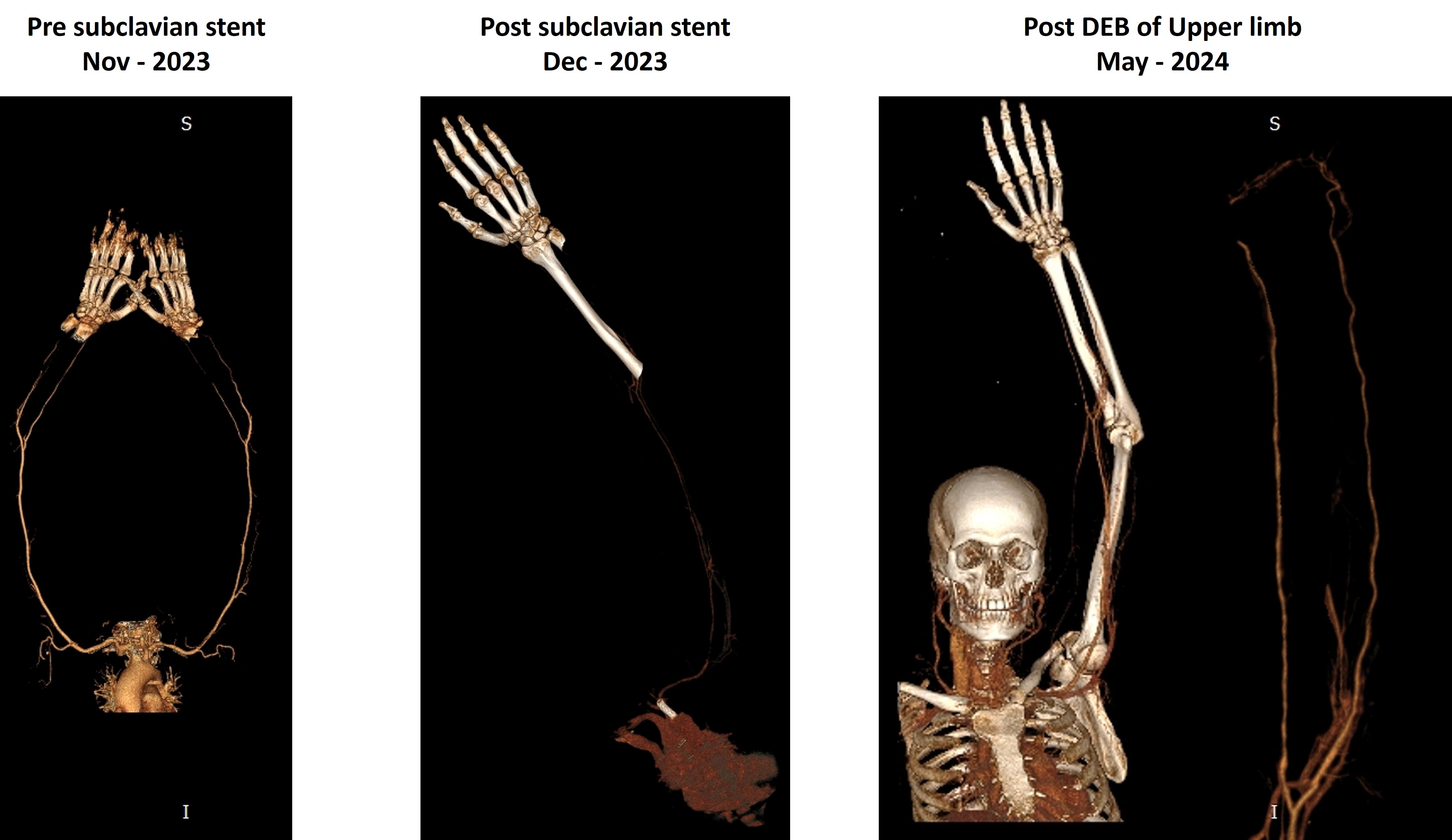
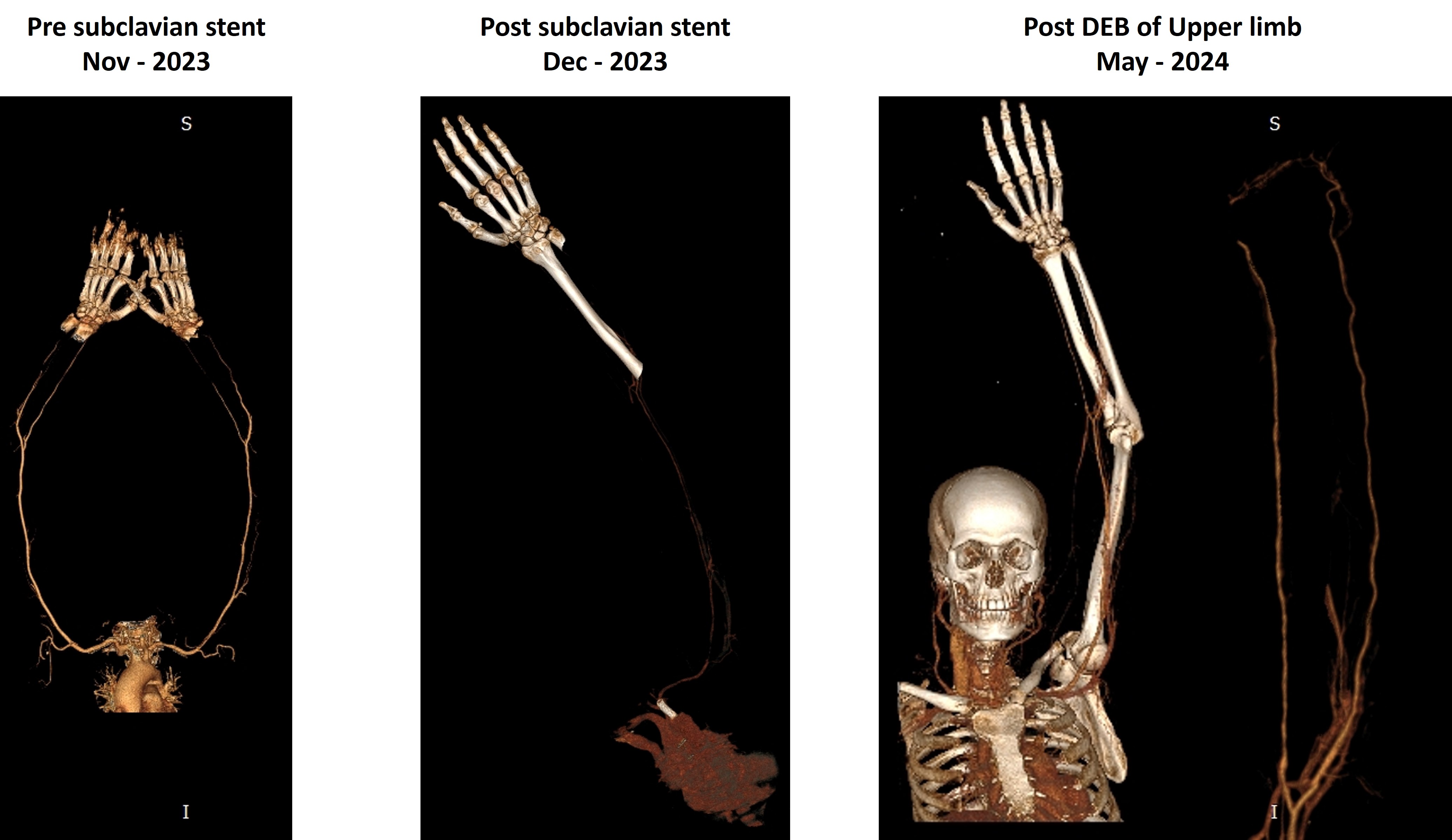
53 Y/M, no comorbidities presented withc/o left upper limb claudication. CT-angio showed narrowing of left subclavian artery and brachial artery narrowing. CAG showed mild CAD and advised medical management for coronaries.
Relevant Test Results Prior to Catheterization
Access through RFA, left subclavian artery engaged with JR 3.5 - 6 Fr guiding catheter. 0.032 Terumo wire crossed and parked distally in left subclavian artery. Terumo wire exchanged with Hi torque command wire.8x29mm Quick link Elite deployed at 10 atms. The final result was good.

Relevant Catheterization Findings
6 months later. Access through right femoral artery using JR 3.5 - 7Fr guiding catheter wire passed through subclavian artery using cook CXT micro catheter SCAD present throughout arterial system. Command wire exchanged with Terumo wire. Lesion dilated with 2.5x80mm Armada 14 vascular Balloon, 4.0x200mm Meril Mozec PEB deployed in left brachial artery, 5.0x200mm Meril Mozec PEB deployed proximally & 2.5x200mm Meril Mozec PEB Balloon. One month follow up CT shows no complications

Interventional Management
Procedural Step
Access through right femoral artery, left subclavian artery engaged with JR 3.5 - 6 Fr guiding catheter. 0.032 Terumowire crossed and parked distally in left subclavian artery.. Terumo wire exchanged with Hi torque command wire.8x29mm Quick link Elite deployed at 10 atms. The final result was good. 6 months later. Access through right femoral artery using JR 3.5 - 7Fr guiding catheter wire passed through subclavianartery using cook CXT micro catheter SCAD present throughout arterial system. Command wire exchangedwith Terumo wire. Lesion dilated with 2.5x80mm Armada 14 vascular Balloon at 08 atms. Then 4.0x10mmArmada 35 Balloon attempted to be passed ti subclavian artery, but shaft did not crossed. Hence JRexchanged for long 70cms femoral sheath over 2.5x08mm Balloon. Then 4.0x10mm Armada Balloon dilatedat 10 atms. 4.0x200mm Meril Mozec PEB deployed in left brachial artery at 06 atms and 2 inflation x 1 minuteeach. Then 5.0x200mm Meril Mozec PEB deployed proximaly at 06 atms x 1 minute each x 2 inflation. Thenterumo wire exchanged for command wire over CXI micro catheter and passed through radial artery, throughpalwar arch into ulnar artery and predilated through otu with 2.5x80mm Armada Balloon at 06 atms. Then2.5x200mm Meril Mozec PEB Balloon deployed at 06 atms x 2 inflations for 1 minute each. Right femoral sheath removed and closed with Angioseal. The final result was good with no complications. One month follow up CT shows no complications
Case Summary
When severe stenoses or short occlusion of the ulnar arteryare identified and appear amenable to angioplasty, we believe such treatment should be attempted. The pro-cedure may relieve the patient’s symptoms, heal necroticlesions, and save the access and the hand without affectingarterial patency.