
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-183
Navigating PCI in Heart Failure
By Rhuban Sundran, Shaiful Yahaya
Presenter
Rhuban Sundran
Authors
Rhuban Sundran1, Shaiful Yahaya1
Affiliation
Institut Jantung Negara, Malaysia1,
View Study Report
TCTAP C-183
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Navigating PCI in Heart Failure
Rhuban Sundran1, Shaiful Yahaya1
Institut Jantung Negara, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
48 year old male presented to clinic in a wheelchair with gross ascites and peripheral oedema. He complained of orthopnoea and shortness of breath, NYHA class 4. Sleeps most in the chair sat upright. 3 admissions to a peripheral hospital with similar symptoms. He had no known medical illness but had family history of coronary artery disease.
RR: 26BP: 130/70HR: 94Decreased air entry till midzone bilaterally, raised JVP.Diagnosis of acute decompensated heart failure and planned for admission.
RR: 26BP: 130/70HR: 94Decreased air entry till midzone bilaterally, raised JVP.Diagnosis of acute decompensated heart failure and planned for admission.
Relevant Test Results Prior to Catheterization
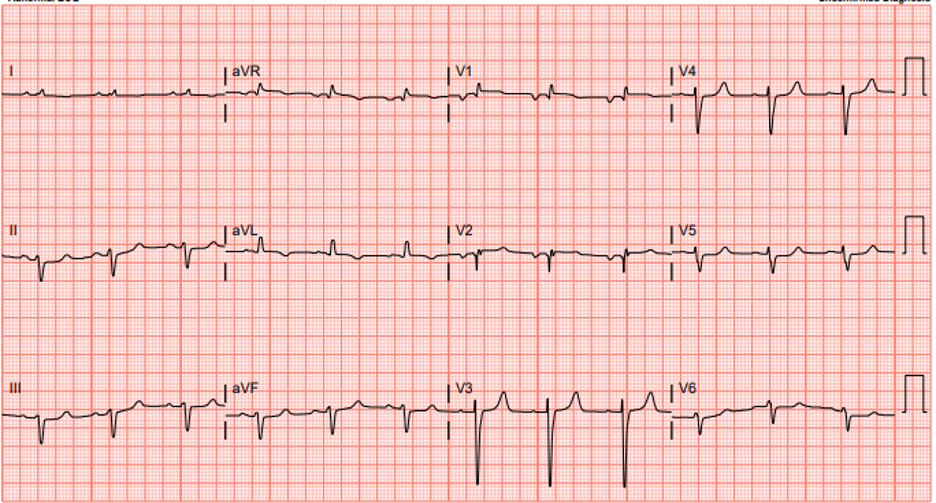
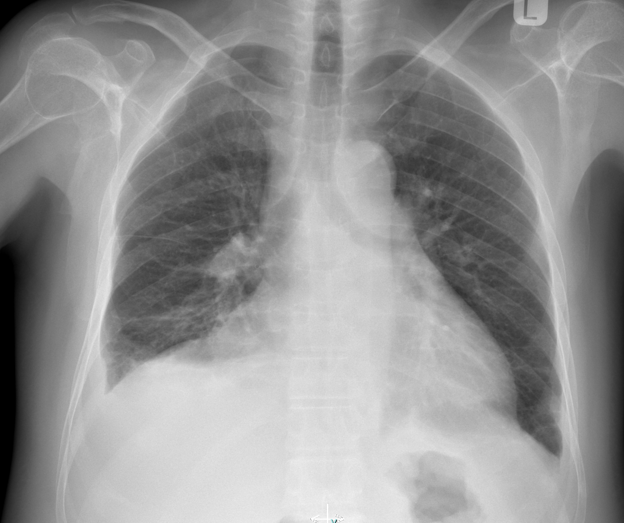
Chest x ray - fluid overload with bilateral pleural effusionECG - Sinus rhythm, narrow complex with left axis deviation
Blood investigationCreatinine 358urea 22eGFR 16proBNP >35000
ECHOEF 16%, LVIDd 5.6cm, LVIDs 4.4cm, largest effusion of 1.1cm with no chamber collapse, PASP 57/30mmHg
Technetium viability scan - moderate area of reduced tracer uptake in LAD/LCx territories but all segments viable.

Blood investigationCreatinine 358urea 22eGFR 16proBNP >35000
ECHOEF 16%, LVIDd 5.6cm, LVIDs 4.4cm, largest effusion of 1.1cm with no chamber collapse, PASP 57/30mmHg
Technetium viability scan - moderate area of reduced tracer uptake in LAD/LCx territories but all segments viable.
Relevant Catheterization Findings
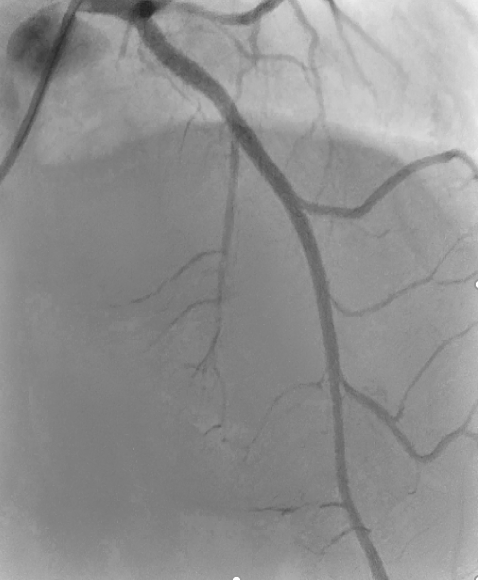
Coronary angiogramLMS: normalLAD: CTO proximal with retrograde from RCARamus: Severe proximal stenosisLCx: normalRCA: Dominant. Normal
Only single shot of the RCA was taken as diagnostic as planned to use dual puncture to tackle CTO. Decision made in order to minimize contrast use given CKD stage 4.

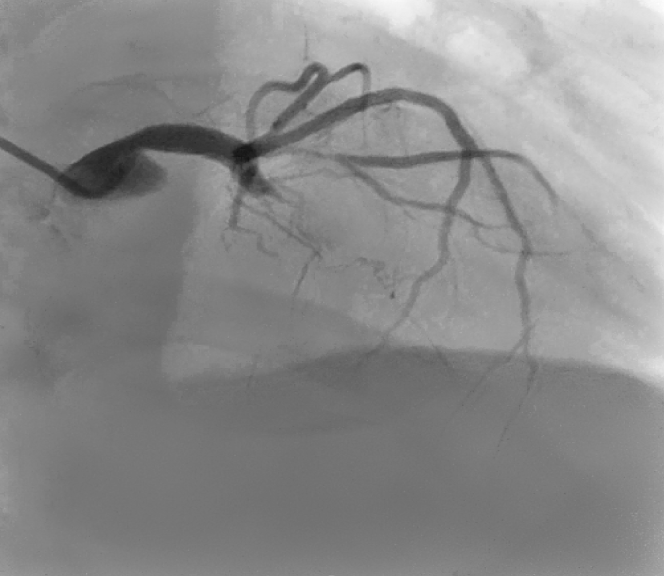
Only single shot of the RCA was taken as diagnostic as planned to use dual puncture to tackle CTO. Decision made in order to minimize contrast use given CKD stage 4.
Interventional Management
Procedural Step
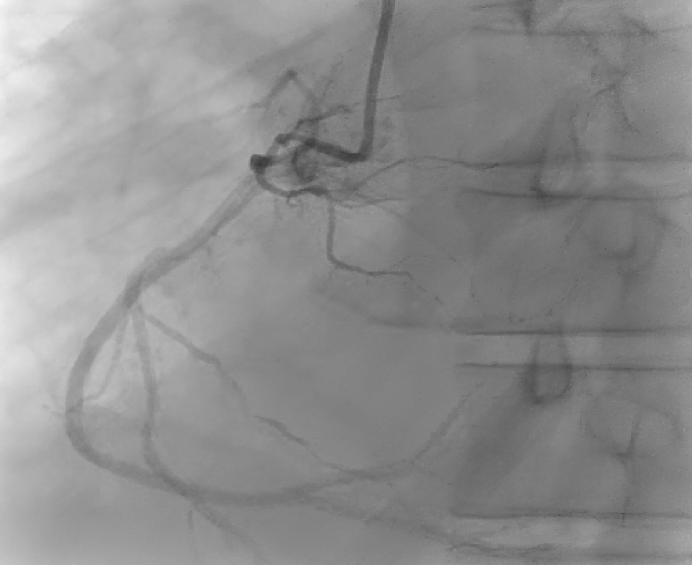
PCI CTO LADEBU 3.5 6Fr via RFA into LCAJR 3.5 6Fr via RRA into RCA (retrograde shot)
Fielder XT crossed lesion with caravel microcatheter supportWire exchanged to Sion BluePredilation: 2.0mmx15 Semi compliant balloon @ 8atm, NC 2.5mmx15@12atmIVUS: Fibrocalcified plaque, distal vessel size 3.0mm, proximal vessel size 4.0mmPredilation: 3.5mmx15 NC scoreflex @ 18atmStent: 3.0x48mm @ 12atm, postdilated with NC 4.0x15mm@18atmIVUS: Stent well opposed and expanded with no edge dissectionsGood final results
PCI Ramus IntermediatePredilated 2.0mmx15 semi compliant balloon @6atm, DCB 2.25x15mm @7atm for 45secondsFinal result showed no dissections with TIMI 3 flowNo immediate complicationsFemoral puncture sealed with proglide 6Fr

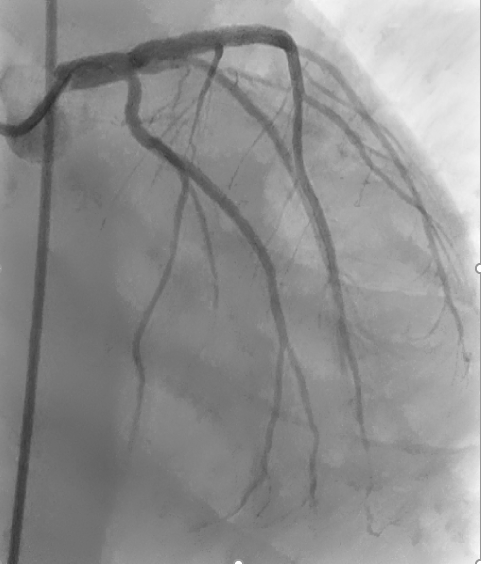
Fielder XT crossed lesion with caravel microcatheter supportWire exchanged to Sion BluePredilation: 2.0mmx15 Semi compliant balloon @ 8atm, NC 2.5mmx15@12atmIVUS: Fibrocalcified plaque, distal vessel size 3.0mm, proximal vessel size 4.0mmPredilation: 3.5mmx15 NC scoreflex @ 18atmStent: 3.0x48mm @ 12atm, postdilated with NC 4.0x15mm@18atmIVUS: Stent well opposed and expanded with no edge dissectionsGood final results
PCI Ramus IntermediatePredilated 2.0mmx15 semi compliant balloon @6atm, DCB 2.25x15mm @7atm for 45secondsFinal result showed no dissections with TIMI 3 flowNo immediate complicationsFemoral puncture sealed with proglide 6Fr
Case Summary
This case required multiple aspects to be tackled prior to angiogram and angioplasty. Prior to even counselling for the procedure, the patient had very poor EF of 16% and CKD stage 4. Limitations in initiating GDMT due to CKD. Patient was offloaded and was finally able to lie flat losing 12kg in the process. Viability scan in the form of technetium 99 was chosen due to kidney function and myocardium was shown to be viable. Counselling regarding the very high possibility of dialysis was given before embarking on coronary intervention.
Patient had good results and did not require dialysis. Most recent EF is 35% and GDMT is slowly being optimized. In high risk patients, planning is vital.
Patient had good results and did not require dialysis. Most recent EF is 35% and GDMT is slowly being optimized. In high risk patients, planning is vital.