
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-001
A Challenging Case Report: Cardiac CT and IVUS in the Acute Management of Spontaneous Coronary Artery Dissection
By Noriyuki Wakana, Shigeki Takai, Takeshi Sugimoto, Hiroyuki Yamada
Presenter
Noriyuki Wakana
Authors
Noriyuki Wakana1, Shigeki Takai1, Takeshi Sugimoto1, Hiroyuki Yamada1
Affiliation
Kyoto Tanabe Central Hospital, Japan1,
View Study Report
TCTAP C-001
Coronary - ACS/AMI
A Challenging Case Report: Cardiac CT and IVUS in the Acute Management of Spontaneous Coronary Artery Dissection
Noriyuki Wakana1, Shigeki Takai1, Takeshi Sugimoto1, Hiroyuki Yamada1
Kyoto Tanabe Central Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
The patient is a 39-year-old male. He experienced persistent chest pain for three hours and was urgently transported to our hospital.After his arrival, his chest pain showed some reduction. His past medical history was nothing and no coronary risk factors.
Relevant Test Results Prior to Catheterization
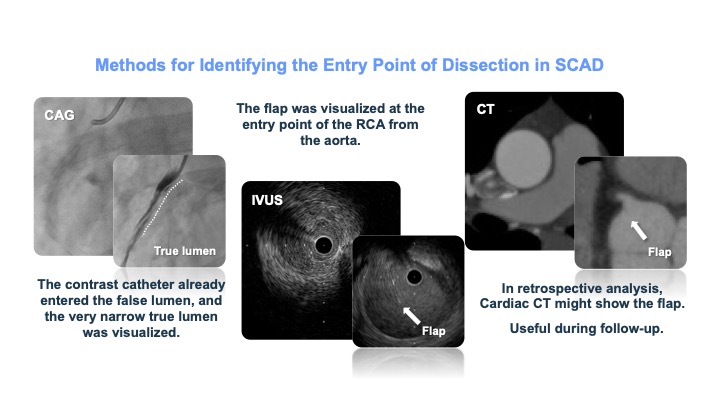
A cardiac CT was performed, revealing a narrowing of the right coronary artery. Suspecting SCAD, we considered observation, but due to worsening chest pain and ST elevation in leads II, III, and AVF on the ECG, and the patient going into shock, we performed an emergency CAG.
Relevant Catheterization Findings
Dissection was observed from the proximal part near the entrance of the right coronary artery. Treatment was initiated by inserting an IABP.
Interventional Management
Procedural Step
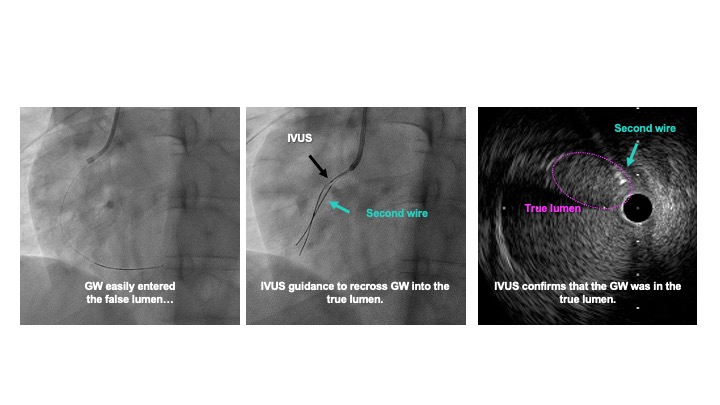
A 39-year-old male experienced persistent chest pain for three hours and was urgently transported to our hospital. Upon arrival, his chest pain reduced. Considering his young age, lack of significant coronary risk factors, and improved symptoms, we suspected CSA or SCAD and performed coronary CT first. The CT revealed narrowing and suspected dissection in the distal right coronary artery, but blood flow to the distal region was maintained. Observation was initially chosen.However, the patient suddenly experienced severe chest pain again and went into shock, with ST elevation in leads II, III, and aVF on ECG. Emergent coronary angiography (CAG) showed dissection from the proximal part of the right coronary artery. We inserted an IABP and proceeded with PCI. The guidewire initially entered the false lumen but, using IVUS guidance, we successfully repositioned it into the true lumen. After confirming the true lumen with IVUS, we performed dilation with a perfusion balloon, achieving TIMI II blood flow. The patient’s chest symptoms and ECG improved, and PCI was completed successfully.
Case Summary
We experienced a case of SCAD in a young patient. Although the treatment was challenging due to the dissection from the proximal part near the entrance of the right coronary artery, we succeeded in repositioning the wire using IVUS guidance.