
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-141
What Knot to Do: Untwisting the Twisted Catheter Using Kissing-Catheter Technique
By Andrew Parlautan
Presenter
Andrew Parlautan
Authors
Andrew Parlautan1
Affiliation
RSUD Raja Ahmad Tabib, Indonesia1,
View Study Report
TCTAP C-141
Coronary - Complication Management
What Knot to Do: Untwisting the Twisted Catheter Using Kissing-Catheter Technique
Andrew Parlautan1
RSUD Raja Ahmad Tabib, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 59-year-old woman with late onset ST-elevation myocardial infarction (STEMI) was admitted for Percutaneous Coronary Intervention (PCI). On admission, patient complained of epigastric pain and dyspnea on exertion since a day ago. Physical examination revealed clear lung sound on auscultation and no murmur was heard. Her blood pressure was 169/75 mmHg, heart rate 65 beats/minute, oxygen saturation 98% in room air, respiratory rate 20 breaths per minute, and temperature was 36.5 °C.
Relevant Test Results Prior to Catheterization
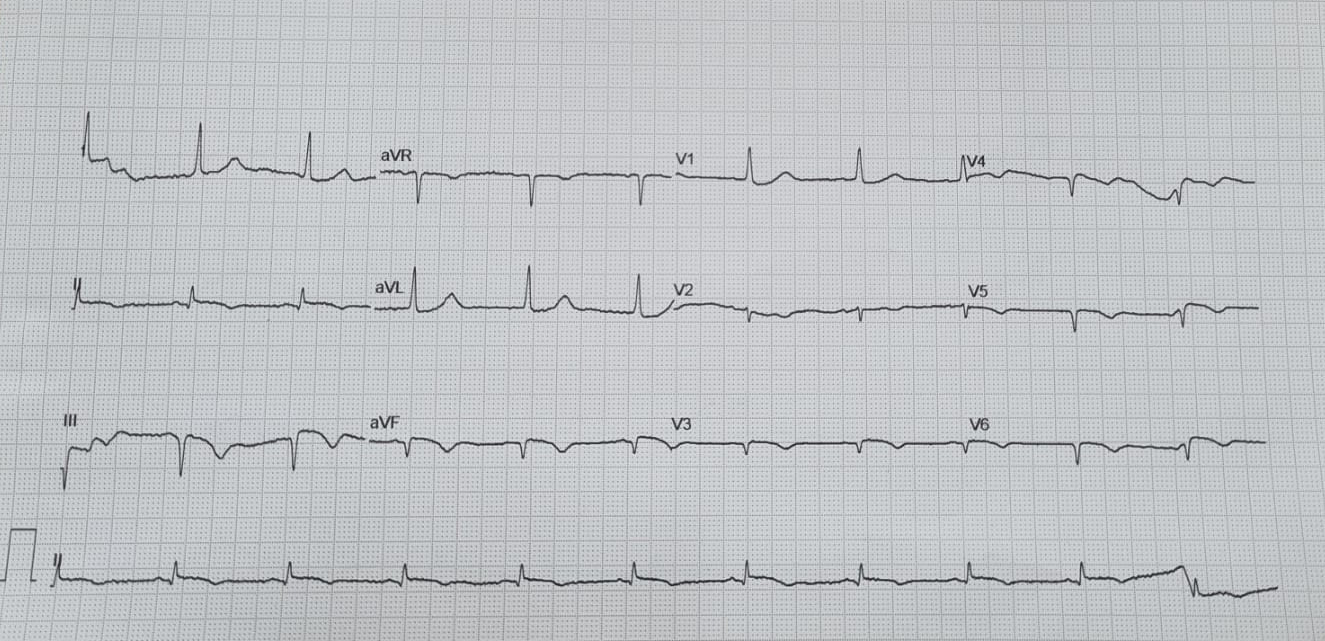
Electrocardiogram (ECG) showed Q waves and ST elevation in lead II, III, aVF. Her laboratory investigation revealed hemoglobin 13.2 g %, total leucocyte counts 10.710 cells/mm3, and platelets 244.000 cells/mm3. The cardiac markers Troponin I was significantly elevated 74.71 ng/ml. Her random blood sugar (RBS) was 161 mg/dl, and creatinine 0.89 mg/dl. Electrolyte was within normal limit. Chest X Ray showed normal heart and lung findings.
Relevant Catheterization Findings
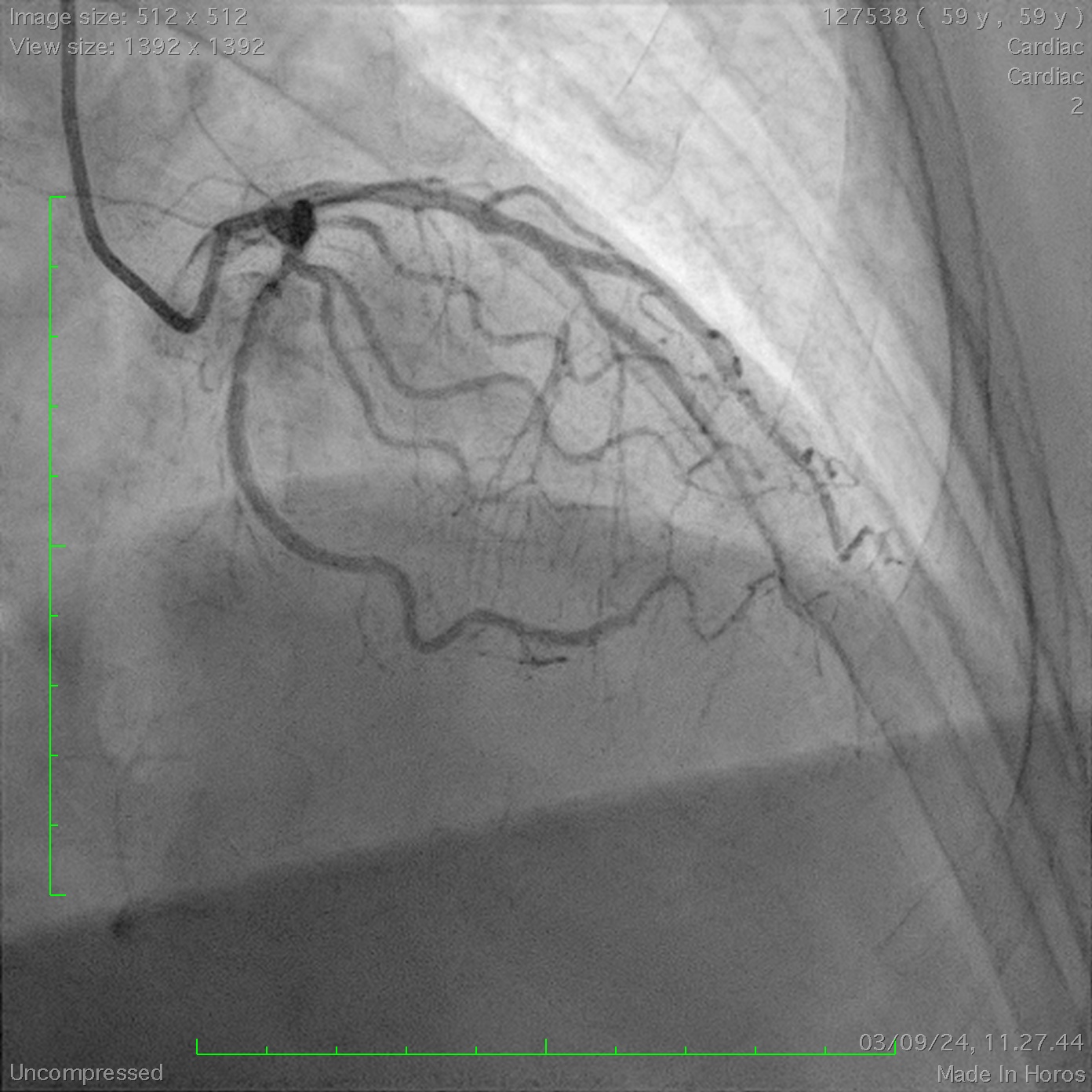
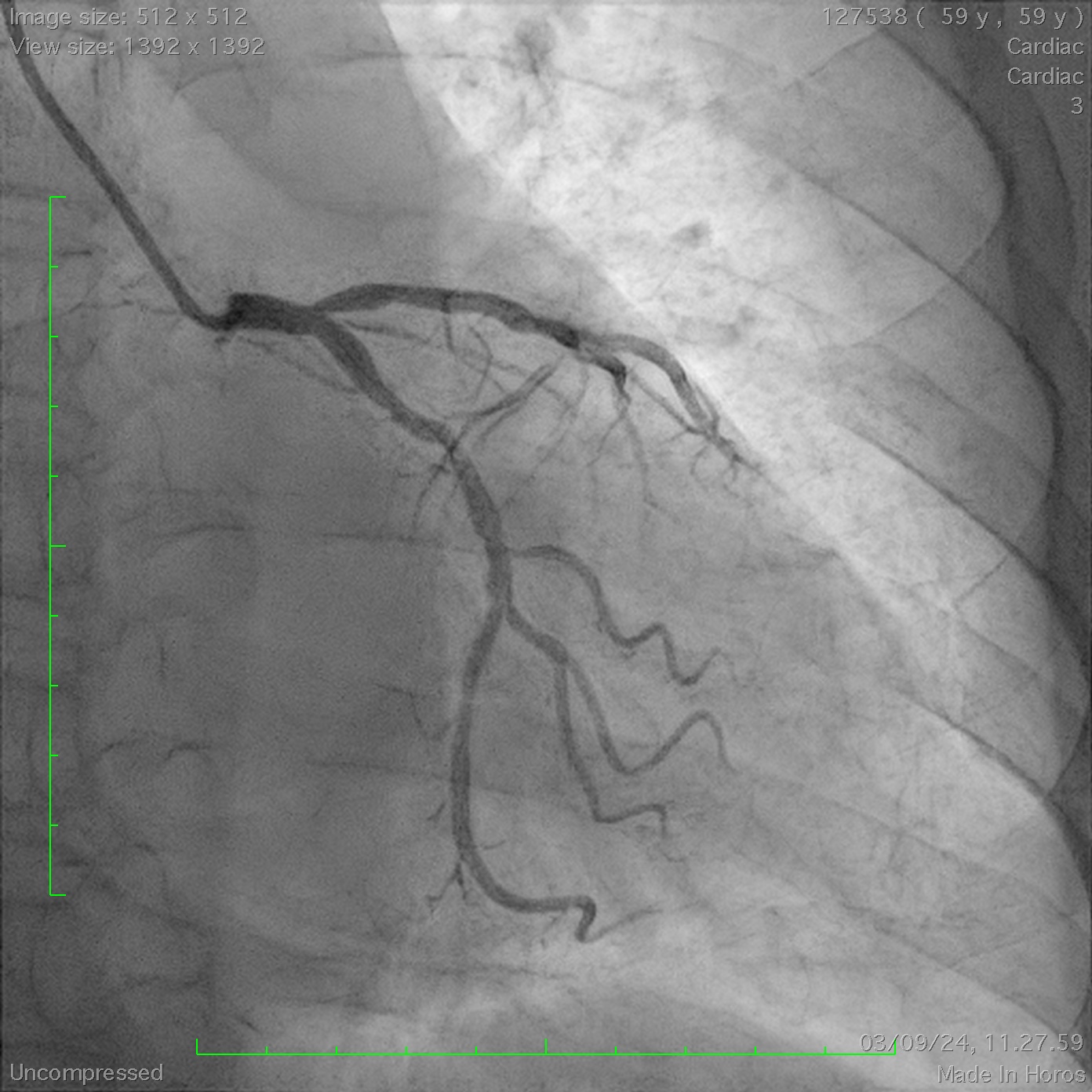
LM: non significant stenosis LAD: moderate stenosis at osteal and mid part of LADLCX: mild to moderate stenosisRCA: total occlusion at proximal part
Interventional Management
Procedural Step
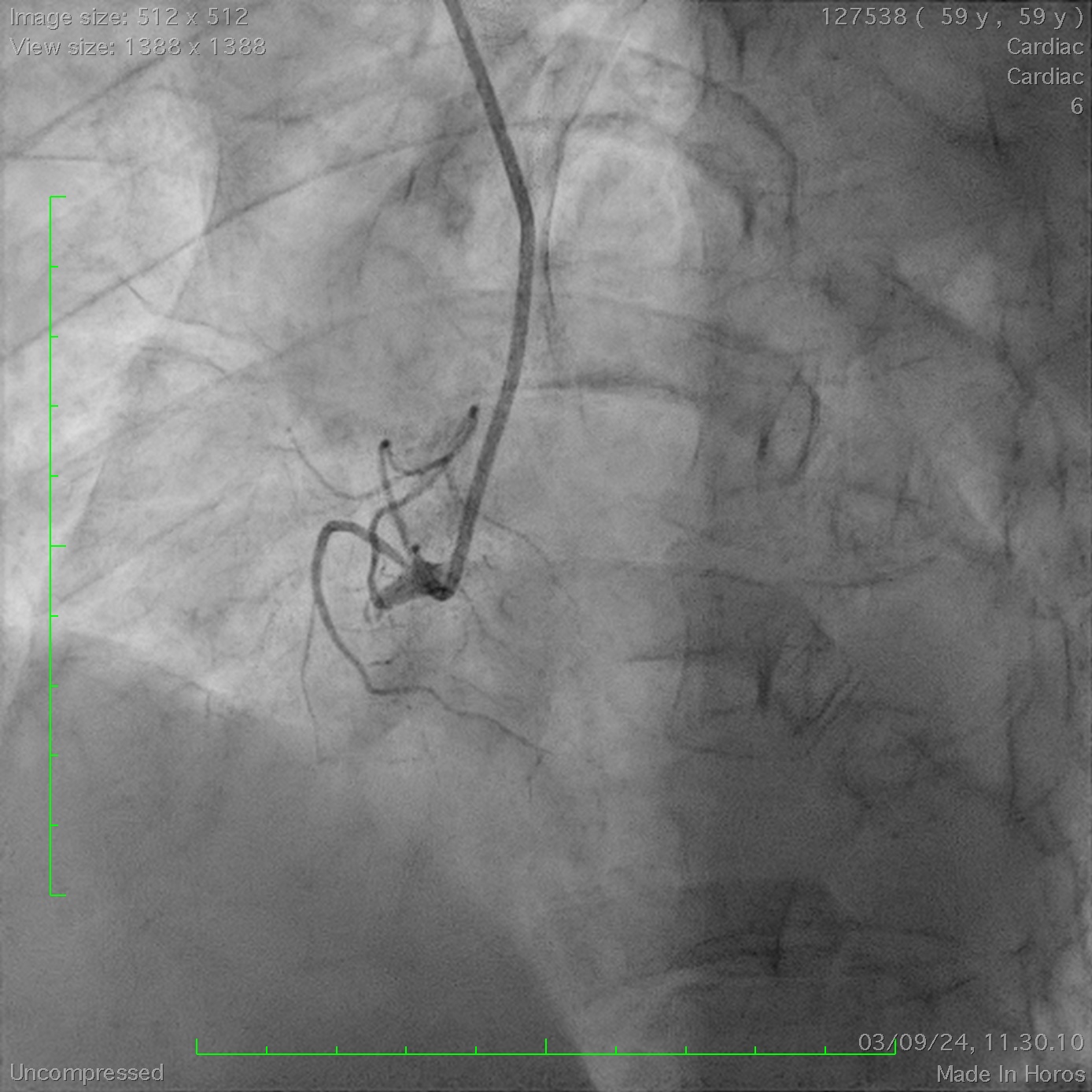
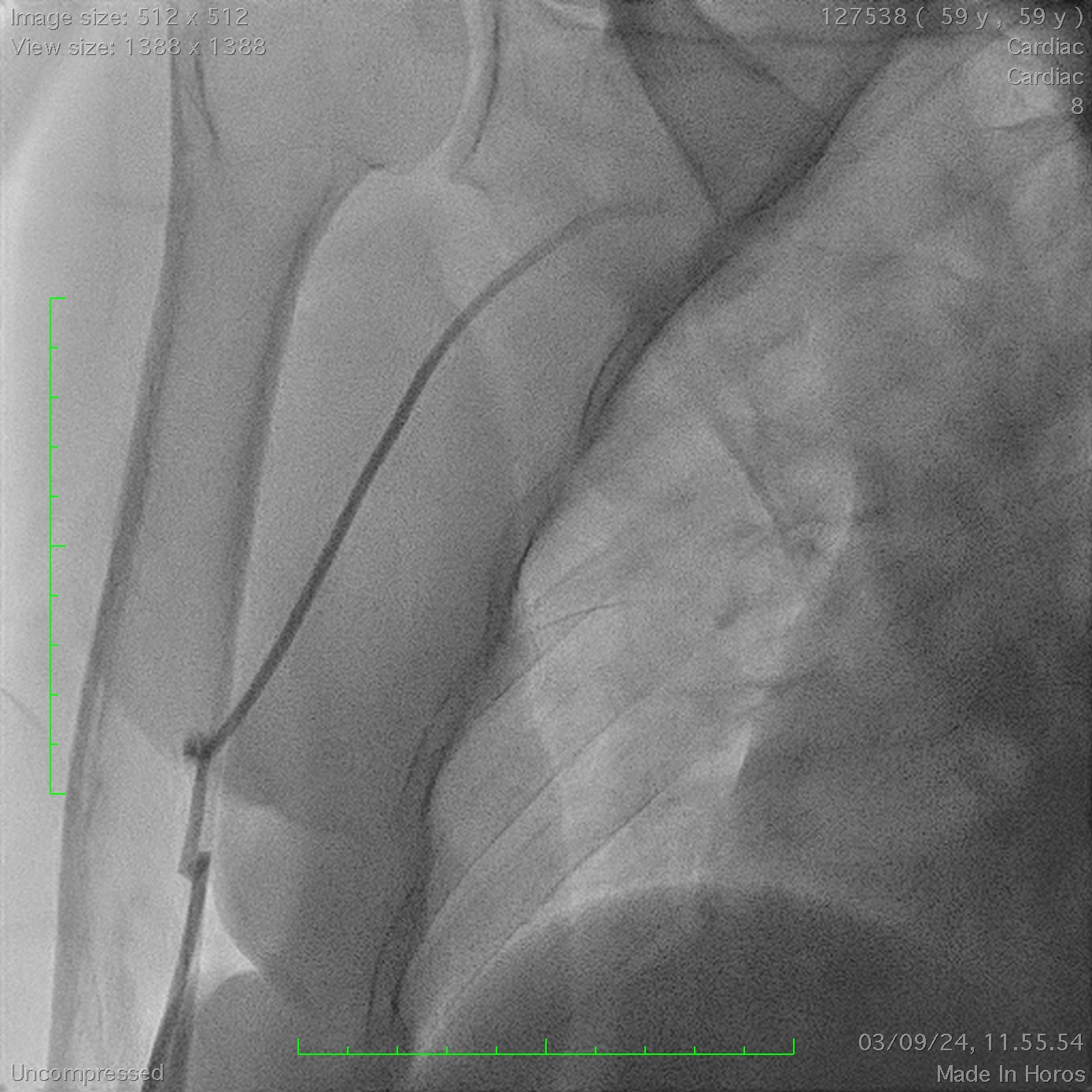
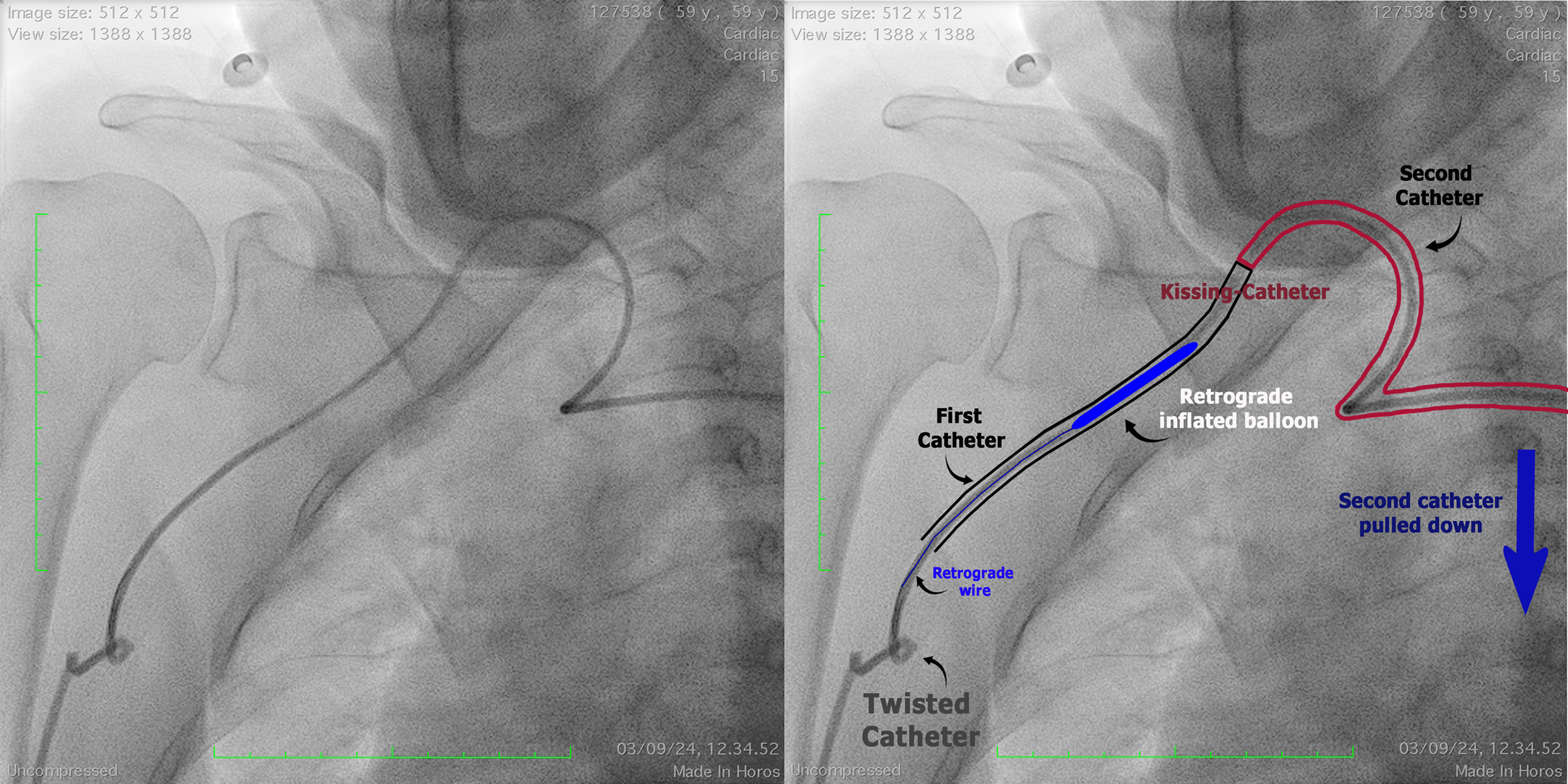
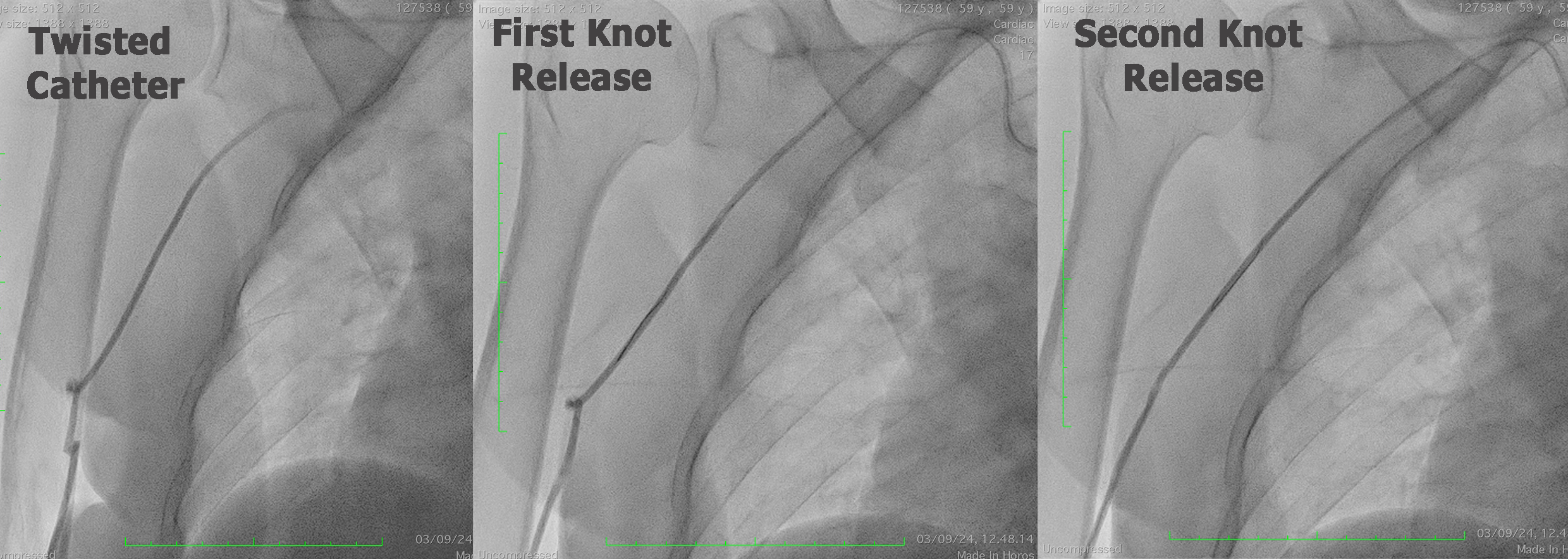
We did diagnostic angiography from right radial artery using IL 6F. LCA showed non-significant stenosis at Left Main, mild to moderate stenosis at LAD and LCX. RCA showed total occlusion at proximal part. Patient was planned for PCI using the same guiding catheter but unfortunately the catheter was disengaged from RCA ostium. Clockwise and anti-clockwise maneuver was unsuccessful, and we realized that the catheter was twisted at brachial artery (figure 1). Some maneuver was done by pulling and rotating to untwist the catheter but unsuccessful.
Case Summary
PCI procedure could also rise some complications and sometimes take us by surprise, like our case that described above. Caution is important when doing a catheter manipulation, especially when some resistance felt. We should not be panic over the unpredicted complication. We should decide precise methods and took steps wisely according to the patient’s condition.