
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-059
Pyrotechnics in Calcified Vessel Intervention
By Wan Faizal Wan Rahimi Shah, Rosli Mohd Ali
Presenter
Wan Faizal Wan Rahimi Shah
Authors
Wan Faizal Wan Rahimi Shah1, Rosli Mohd Ali1
Affiliation
Cardiac Vascular Sentral Kuala Lumpur, Malaysia1,
View Study Report
TCTAP C-059
Coronary - Complex PCI - Calcified Lesion
Pyrotechnics in Calcified Vessel Intervention
Wan Faizal Wan Rahimi Shah1, Rosli Mohd Ali1
Cardiac Vascular Sentral Kuala Lumpur, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
56 years old gentleman presented to us for NSTEMI. He is an active smoker, with background Diabetes Mellitus, Hypertension and Dyslipidemia. He had exertional angina while exercising 2 weeks prior to presentation. Of note, he informed us of a prior PCI to LCx in 2015 in which balloons burst during intervention. When patient was brought to the cath lab, he had no angina. Physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
Echo revealed LVEF of 51%. There was hypokinesia at the apex. His heart chambers were normal in sizes. There was mild mitral regurgitation. His maximum recorded Troponin level was 1540 ng/L. Hba1c was 6.8%. Other blood investigation results were unremarkable.
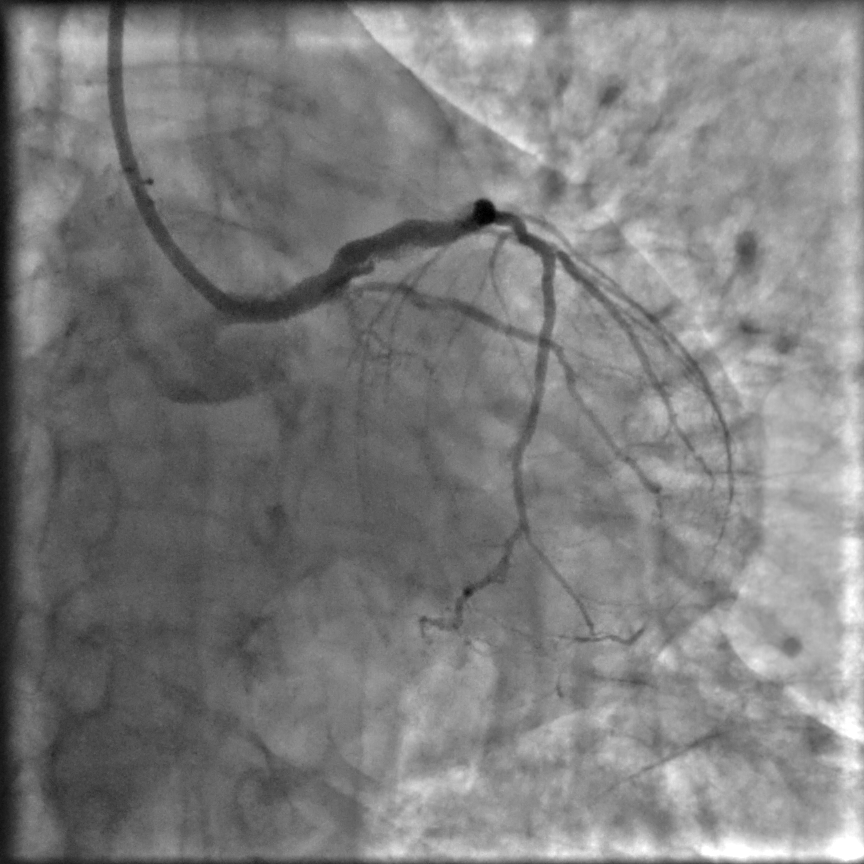
Relevant Catheterization Findings
Coronary angiogram results as below:
LMS - Moderate-severe eccentric stenosis from ostial to distal
LAD - Severe calcification from proximal to midsegmentTight calcified nodule proximal just after large septal branch - minimum CSA of 3.5 mm2Severe mid segment stenosis just distal to D1 bifurcationMyocardial bridge distal segment
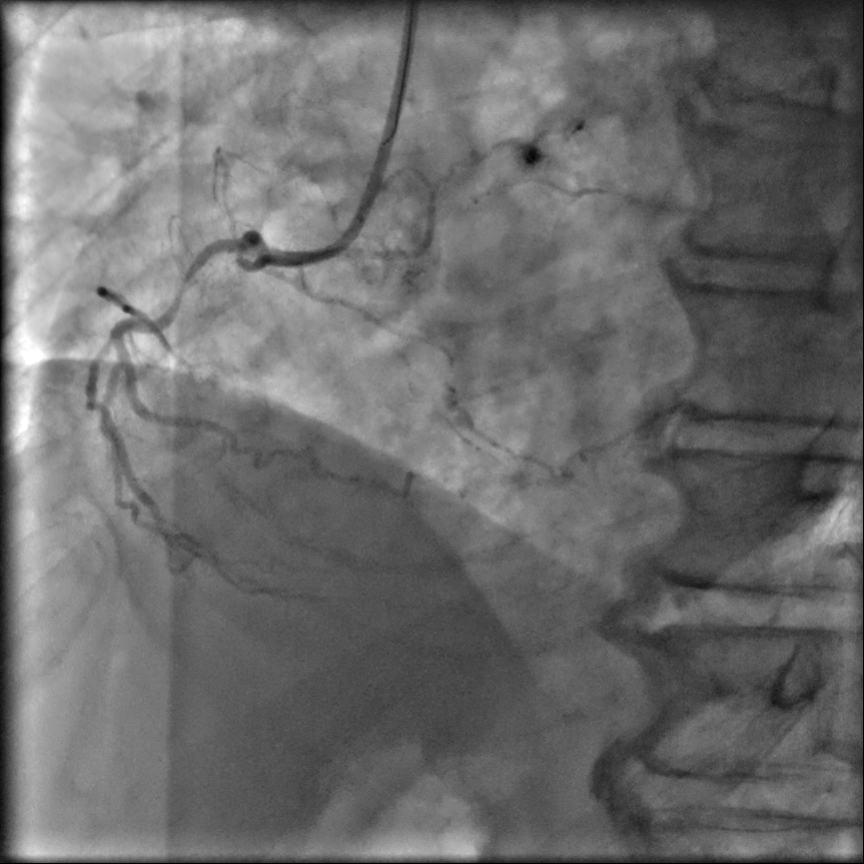
LCx - Dominant vessel with severe calcification. CTO proximal with faint antegrade flow
High OM1 - Severe stenosis in proximal segment
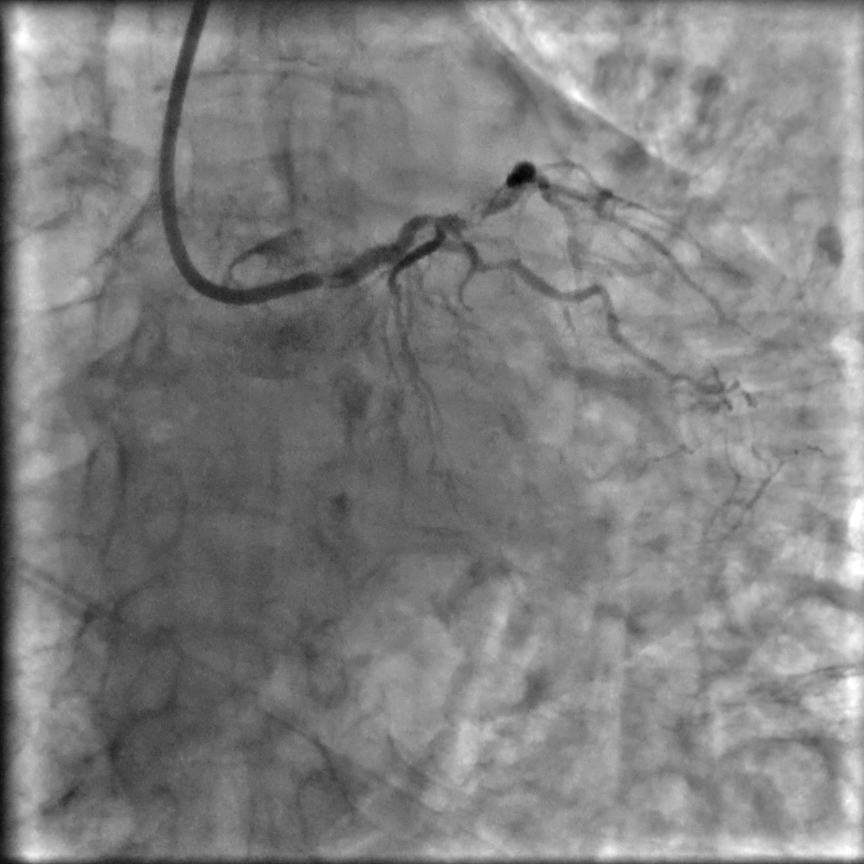
RCA - Smallish with tight mid stenosis
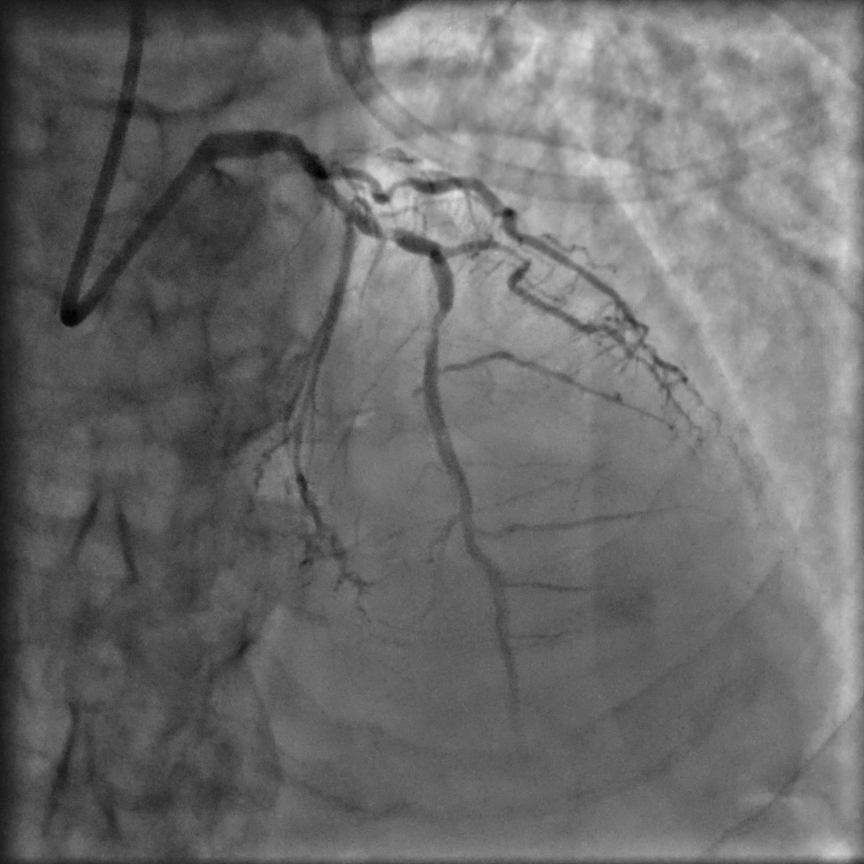

LMS - Moderate-severe eccentric stenosis from ostial to distal
LAD - Severe calcification from proximal to midsegmentTight calcified nodule proximal just after large septal branch - minimum CSA of 3.5 mm2Severe mid segment stenosis just distal to D1 bifurcationMyocardial bridge distal segment
LCx - Dominant vessel with severe calcification. CTO proximal with faint antegrade flow
High OM1 - Severe stenosis in proximal segment
RCA - Smallish with tight mid stenosis
Interventional Management
Procedural Step
PCI to RCAPre-dilated with Emerge 2.0 x 15 mmThen Scoreflex Trio 2.25 x 10 mm at 28 Atm Dissection with significant recoil @ lesion areaStented Synergy XD 2.25 x 20 mm deployed till 20 Atm
PCI to OM1Guide catheter gave good supportPre-dilated with Scoreflex Trio 2.25 x 10 mmDCB Sequent Please Neo 2.25 x 20 mm @ 8 atm for 2 minutesIVUS post DCB done Waited for a while before removing wire PCI to LMS-LADPre-dilated with Emerge 2.0 x 15 mmAttempted to pass IVUS down – unable to negotiate bend @ mid LAD Further pre-dilated with balloons below (Used GuidePlus2 ST extensive to get balloons and stents down)NC Scoreflex Trio 3.0 x 15 mmNC Scoreflex Trio 3.5 x 15 mm- both balloons burst at same location due to the tight calcified nodule proximal LAD IVL Shockwave 3.5 x 12 mm @ 110 pulses before burstIVL Shockwave 4.0 x 12 mm @ 120 pulses but still not expanded well OPNC 3.5 x 10 mm @ max 38 atmLesion finally yielded but complicated by Ellis type II perforationProlonged balloon dilatation with NC Emerge 3.75 x 20 mmThen secured with Papyrus 3.5 x 15 mm at 14 Atm Stented mid LAD with Synergy DES XD 3.0 x 28 mm distal to Covered stentDeployed at 16-18 AtmPost-dilated with 3.25 mm NC balloon at 12-24 Atm Stented LM ostium to LAD with Megatron DES 3.5 x 32 mmPOT with NC Emerge 4.5 x 8 mm at 20 Atm Post-dilated with NC Emerge 3.75 x 20 mm- highest pressure 24 atm @ nodule area Final IVUS run done

PCI to OM1Guide catheter gave good supportPre-dilated with Scoreflex Trio 2.25 x 10 mmDCB Sequent Please Neo 2.25 x 20 mm @ 8 atm for 2 minutesIVUS post DCB done Waited for a while before removing wire PCI to LMS-LADPre-dilated with Emerge 2.0 x 15 mmAttempted to pass IVUS down – unable to negotiate bend @ mid LAD Further pre-dilated with balloons below (Used GuidePlus2 ST extensive to get balloons and stents down)NC Scoreflex Trio 3.0 x 15 mmNC Scoreflex Trio 3.5 x 15 mm- both balloons burst at same location due to the tight calcified nodule proximal LAD IVL Shockwave 3.5 x 12 mm @ 110 pulses before burstIVL Shockwave 4.0 x 12 mm @ 120 pulses but still not expanded well OPNC 3.5 x 10 mm @ max 38 atmLesion finally yielded but complicated by Ellis type II perforationProlonged balloon dilatation with NC Emerge 3.75 x 20 mmThen secured with Papyrus 3.5 x 15 mm at 14 Atm Stented mid LAD with Synergy DES XD 3.0 x 28 mm distal to Covered stentDeployed at 16-18 AtmPost-dilated with 3.25 mm NC balloon at 12-24 Atm Stented LM ostium to LAD with Megatron DES 3.5 x 32 mmPOT with NC Emerge 4.5 x 8 mm at 20 Atm Post-dilated with NC Emerge 3.75 x 20 mm- highest pressure 24 atm @ nodule area Final IVUS run done
Case Summary
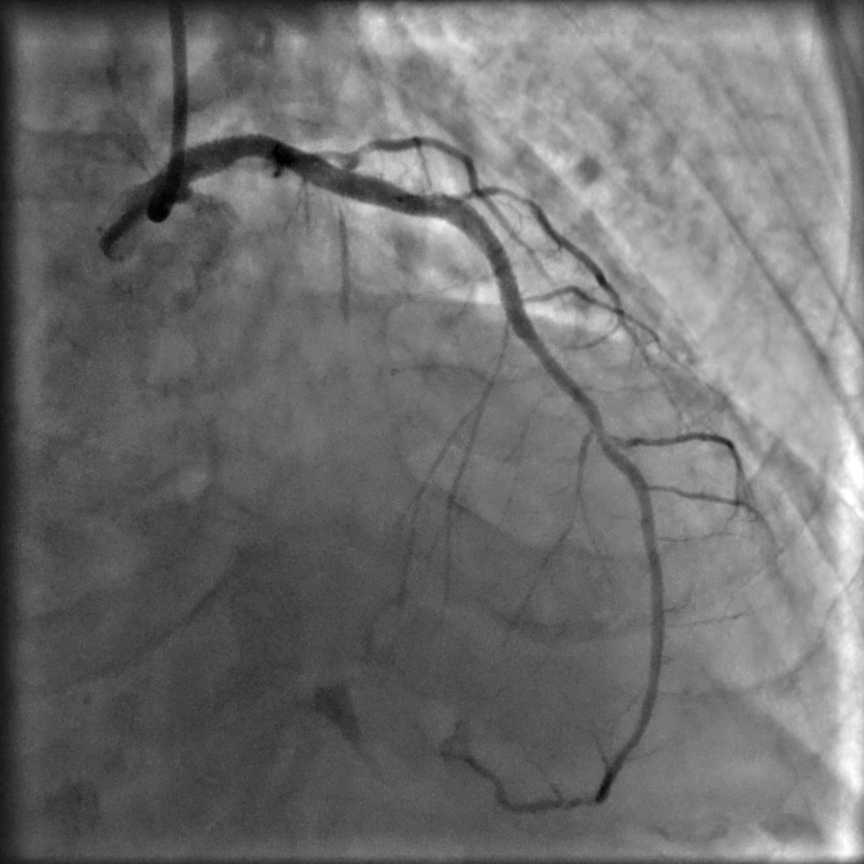
Final ResultsLMS – Good, MSA Body – 12.0 mm2
LAD -Good with TIMI 3 flowSlight under expansion @ nodule proximal to D1Perforation was sealed
MSA areaProximal stent - 11.86 mm2Mid stent - 8.74 mm2Distal stent - 7.1 mm2
High OM (waited till end of PCI procedure. 120 min) - Good with TIMI 3 flow
ConclusionCase depiction of intervention in a large, heavily calcified LAD vessel with also large nodule.Knowledge of all tools are paramount, in terms of strengths and weaknesses.Opted for IVL balloons for plaque modification to negate slow-flow in a large LAD vessel, behaving as last remaining patent vessel.Even with aggressive IVL, there was no perforation. However perforation occured with OPNC balloon.
LAD -Good with TIMI 3 flowSlight under expansion @ nodule proximal to D1Perforation was sealed
MSA areaProximal stent - 11.86 mm2Mid stent - 8.74 mm2Distal stent - 7.1 mm2
High OM (waited till end of PCI procedure. 120 min) - Good with TIMI 3 flow
ConclusionCase depiction of intervention in a large, heavily calcified LAD vessel with also large nodule.Knowledge of all tools are paramount, in terms of strengths and weaknesses.Opted for IVL balloons for plaque modification to negate slow-flow in a large LAD vessel, behaving as last remaining patent vessel.Even with aggressive IVL, there was no perforation. However perforation occured with OPNC balloon.