
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-116
Tackling Complex Left Main Disease: A Challenging Case of Hairline Left Main PCI in RVD Positive Patients, When Surgeon Turndown
By Ahmad Firdaus Zakaria, Huzairi Sani, Khairul Shafiq Ibrahim, Ahmad Bakhtiar Bin Radzi, Raja Ezman Raja Shariff, Rizmy Najmie Khir, Sazzli Kasim
Presenter
Ahmad Firdaus Zakaria
Authors
Ahmad Firdaus Zakaria1, Huzairi Sani1, Khairul Shafiq Ibrahim1, Ahmad Bakhtiar Bin Radzi1, Raja Ezman Raja Shariff1, Rizmy Najmie Khir1, Sazzli Kasim1
Affiliation
Universiti Teknologi Mara, Malaysia1,
View Study Report
TCTAP C-116
Coronary - Complex PCI - Left Main
Tackling Complex Left Main Disease: A Challenging Case of Hairline Left Main PCI in RVD Positive Patients, When Surgeon Turndown
Ahmad Firdaus Zakaria1, Huzairi Sani1, Khairul Shafiq Ibrahim1, Ahmad Bakhtiar Bin Radzi1, Raja Ezman Raja Shariff1, Rizmy Najmie Khir1, Sazzli Kasim1
Universiti Teknologi Mara, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
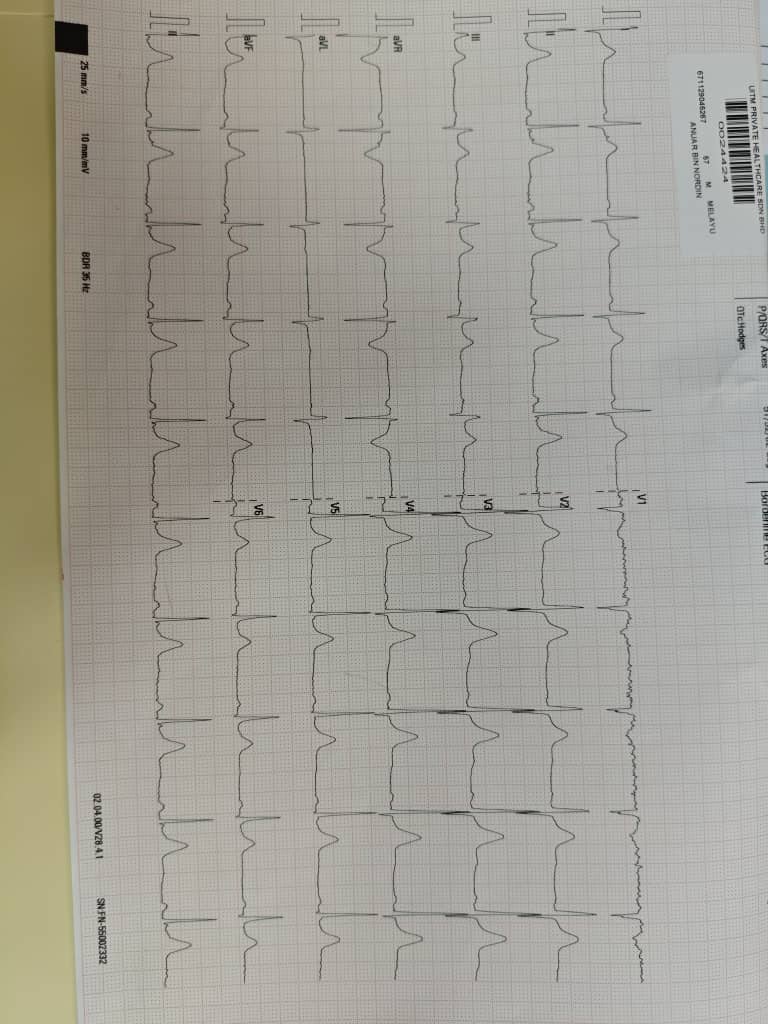
56 years old gentlemen with underlying Hypertension and Dyslipidemia . He is known case of RVD positive patient currently on HAART treatment with CD4 of 1000 and virologically suppressed. He present with acute onset of central chest pain asscoiated with diaphoresis , ECG did show : SR , mild ST elevation at III, AVF with ST depression 1, AVL Peak troponin of 375. He was diagnosed as NSTEMI
Relevant Test Results Prior to Catheterization
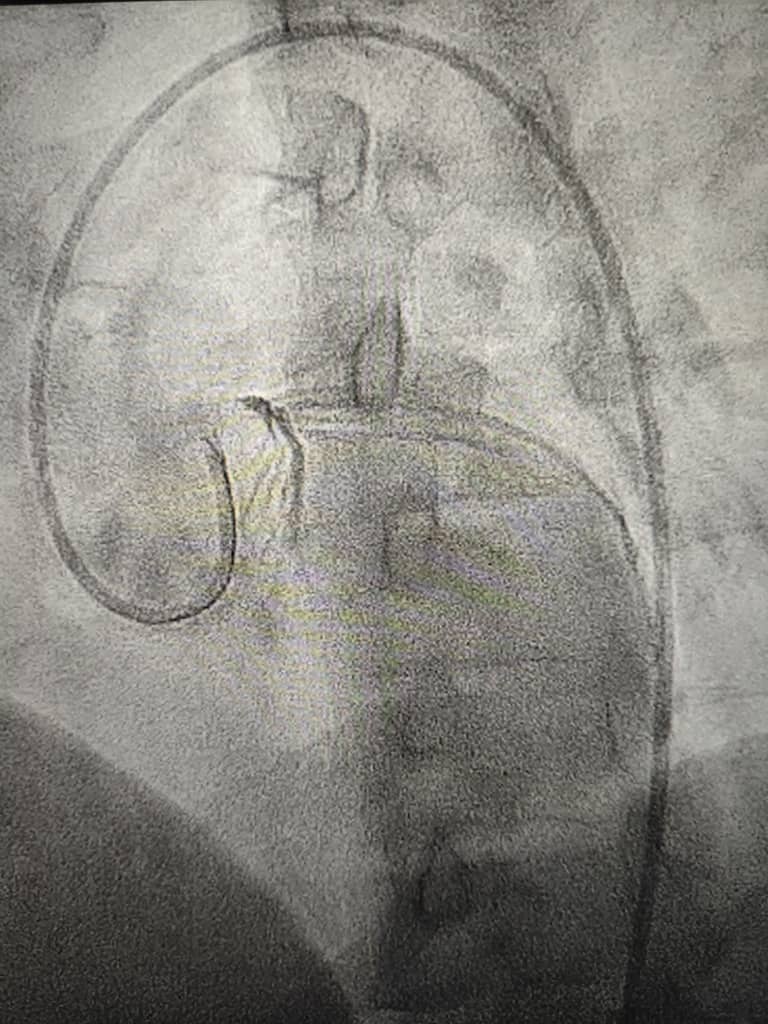
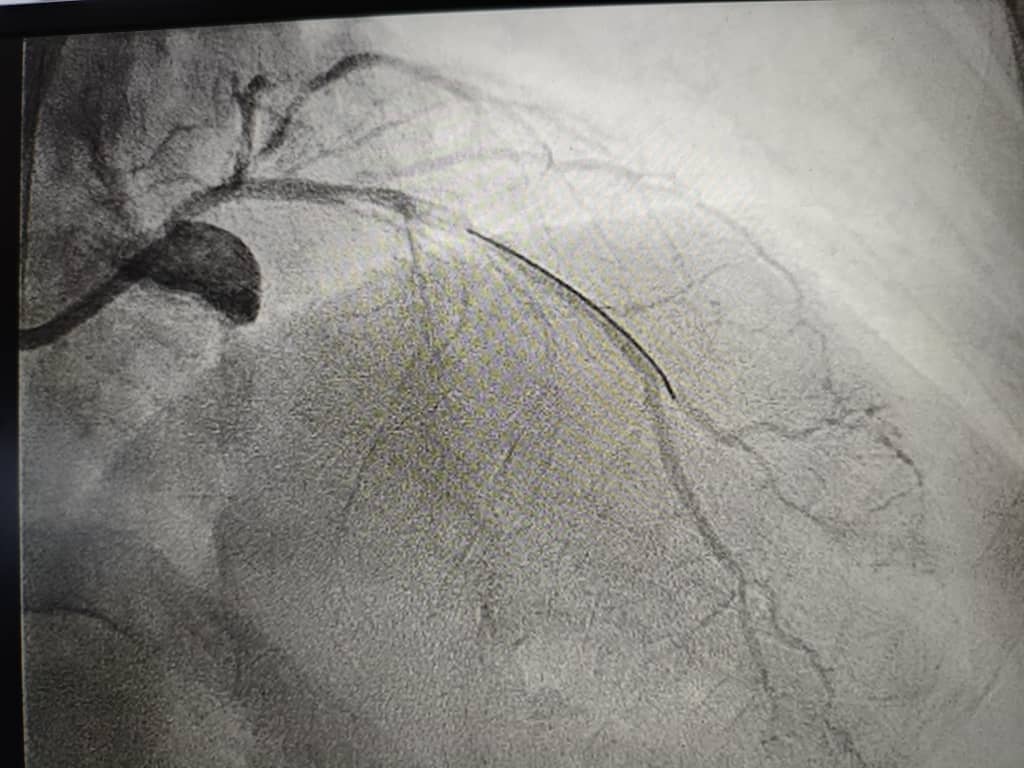
Echocardiogram fairly normal with LVEF : 59% , No RMWA , No LVH , Normal RV function TAPSE : 2.35cm, PASP : 21mmHg.coronary angiogram which show 3VD with severe Left Main stenosis, grey LAD , mild irregular LCX, Ostium 95% , RCA diffused disease.Due to severity of the disease and LM disease , he was referred to cardiothoracic surgeon for urgent CABG . However due to his RVD status ,multiple surgeon turned down this cases. He had persistent pain thus we bring him into ICL for high risk PCI.
Relevant Catheterization Findings
coronary angiogram which show 3VD with severe Left Main stenosis, grey LAD , mild irregular LCX, Ostium 95% , RCA diffused disease.

Interventional Management
Procedural Step
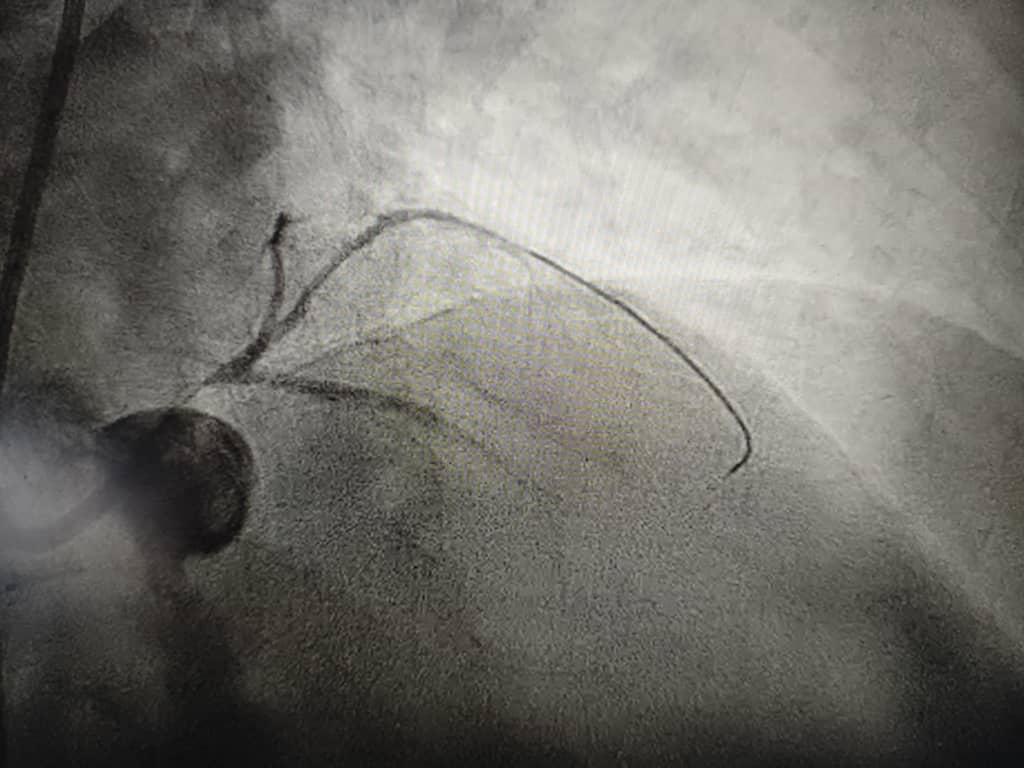
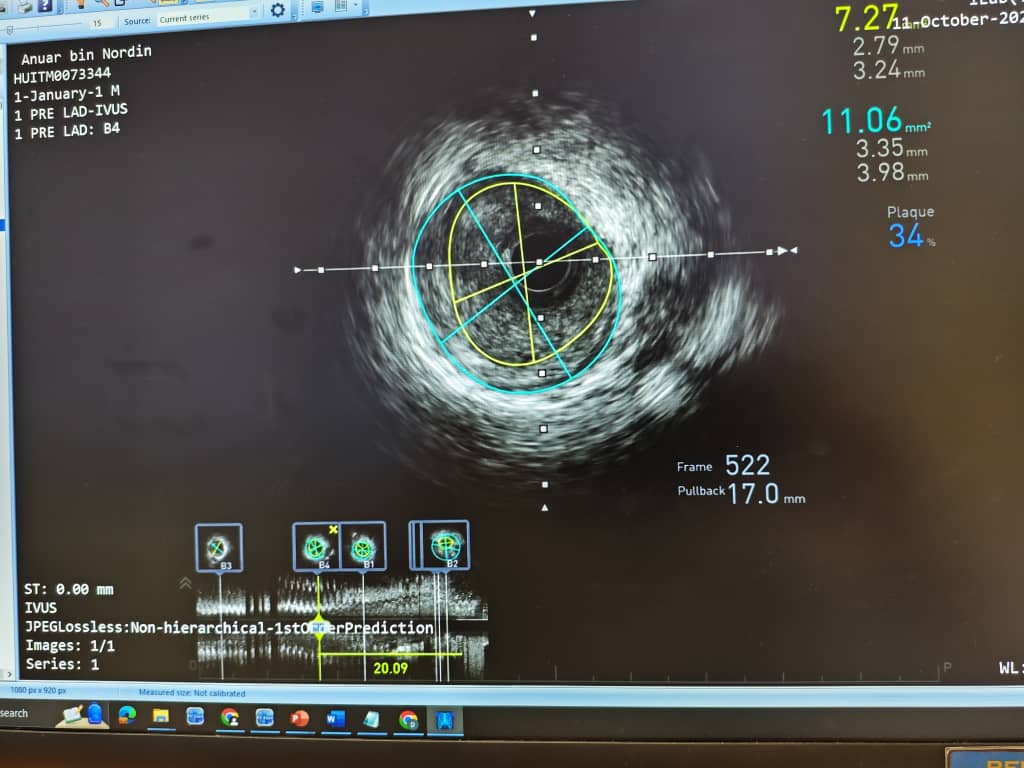
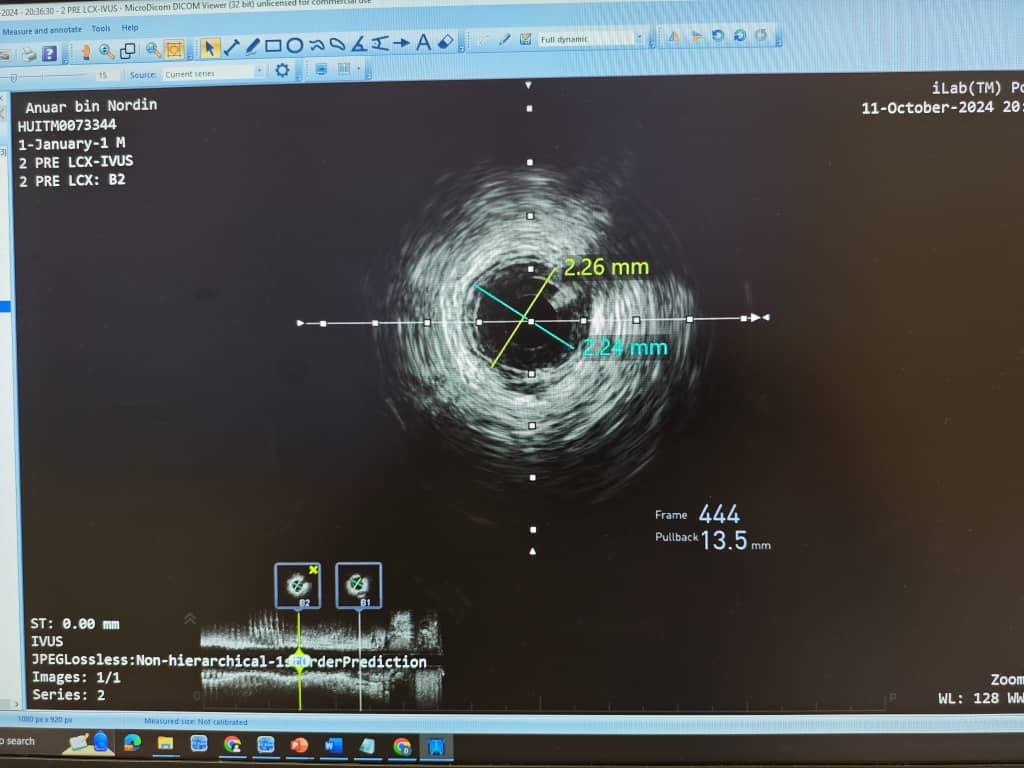
Using Right femoral approach we planned for PCI to LM - LAD. Guide EBU 3.5 7fr wired to LAD . We have problem engaging LM due to verysevere disease. Using wire engagement Asahi Sion Blue finally we manage to wireguided engagement ostial LAD. Then future wired LCx and big OM1. Initialpredilated wolverine Emerge 2.5x14mm from LM into LAD 6- 22atm . After predilatation ofLAD more anatomical view obtained. Then predilated 2.0x15mm 6 to 22atm. LM till LCx. DEB LMat LCx Restore DEB 2.25x20mm using IVUS showed small vessel size. Then PCI to LM-LAD Desyne 3.0x23mm at 9-17 carefully guided by spider view. Post dilatation mozel NC 3.5x8 high pressure. IVUS showed good opposition at LM to LAD .one struct out in aorta. TIMI 3 flow
Case Summary
ConclusionThis case highlights the complexity of severe hairline LMCA disease. This case also highlights the potential of PCI as an alternative to CABG in specific situations involving severe LMCA disease. Continued advancements in technology and techniques may further expand the role of PCI in treating this complex condition.