
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-166
An Approach in Chronic Total Occlusion in Octogenarian: Keep It Safe and Simple
By Doreen Sumpat, New Ru Peng, Koshi Matsuo, Wan Azman Wan Ahmad, Imran Zainal Abidin
Presenter
Doreen Sumpat
Authors
Doreen Sumpat1, New Ru Peng2, Koshi Matsuo3, Wan Azman Wan Ahmad2, Imran Zainal Abidin2
Affiliation
Universiti Malaysia Sabah, Malaysia1, Universiti Malaya, Malaysia2, Yao Tokushukai General Hospital, Japan3,
View Study Report
TCTAP C-166
Coronary - DES/BRS/DCB
An Approach in Chronic Total Occlusion in Octogenarian: Keep It Safe and Simple
Doreen Sumpat1, New Ru Peng2, Koshi Matsuo3, Wan Azman Wan Ahmad2, Imran Zainal Abidin2
Universiti Malaysia Sabah, Malaysia1, Universiti Malaya, Malaysia2, Yao Tokushukai General Hospital, Japan3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 80-year old gentleman, ex-smoker, had sigmoid colon cancer with partial colorectal resection. He had hip replacement and benign prostatic hyperplasia, with high PSA. His brother passed away at the age of 50-year old due to ischemic heart disease. He had 3 days of reduced effort tolerance before started to have central chest pain with profuse sweating. However, he only came to hospital 24 hours after the onset of chest pain as it did not resolved fully with resting and was not able to sleep.

Relevant Test Results Prior to Catheterization
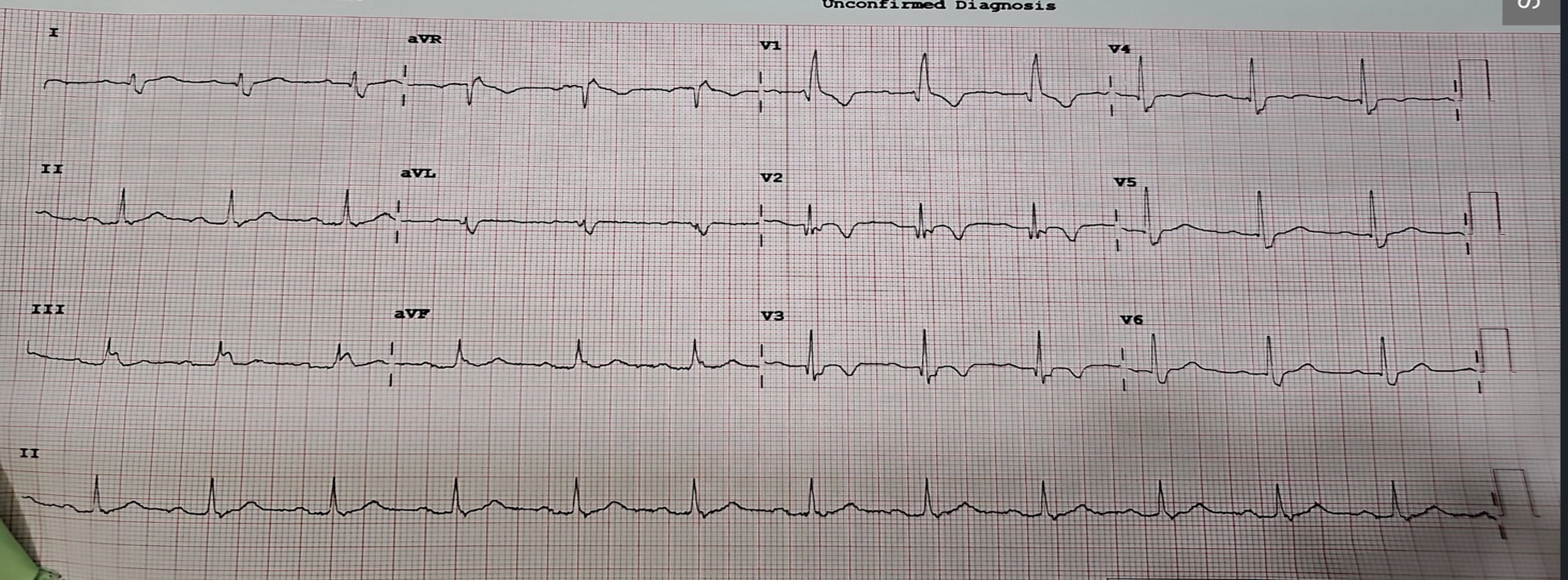
ECG showed Wellens Type B. Serum hs-Troponin and serum LDL were raised. He had hypochromic microcystic anemia with hemoglobin 11.5g/dL. Bedside echocardiogram showed ejection fraction preserved with no hypokinesia.
Relevant Catheterization Findings
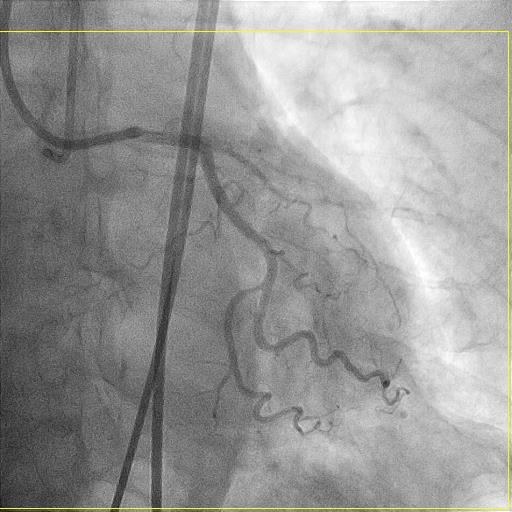
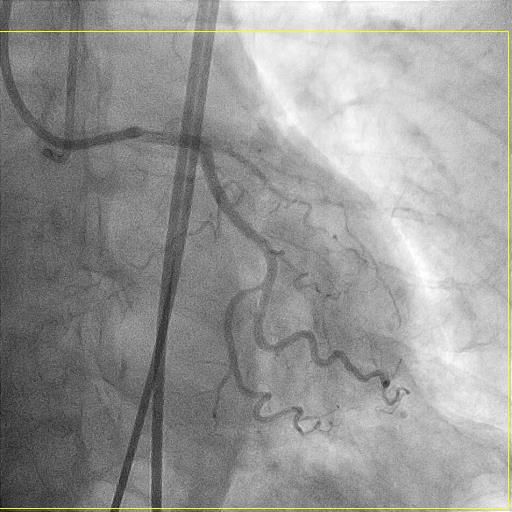
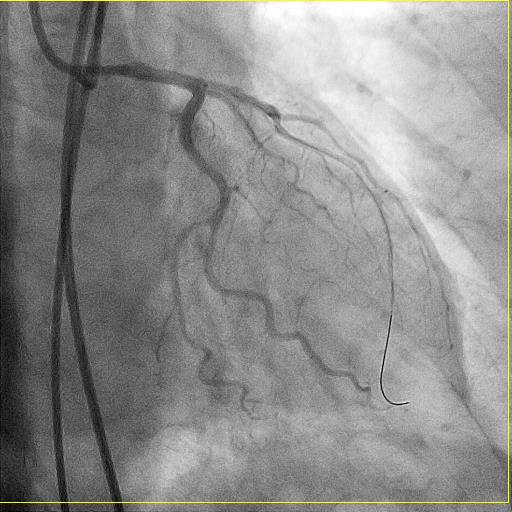
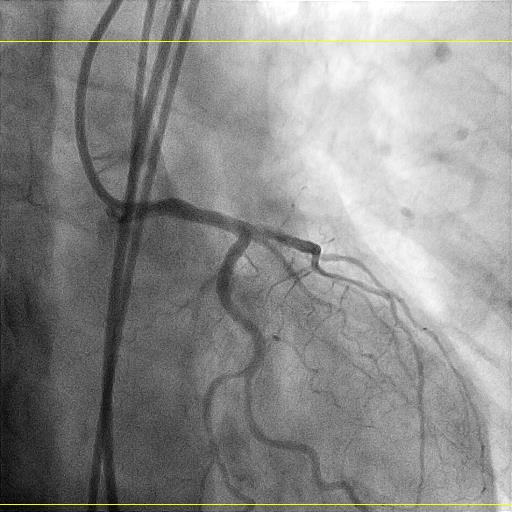
He was treated as NSTEMI and agreeable for coronary coronary intervention. Coronary angiogram showed ostial LAD total occlusion with collateral from RCA. Other coronary arteries were normal with dominant RCA.

Interventional Management
Procedural Step
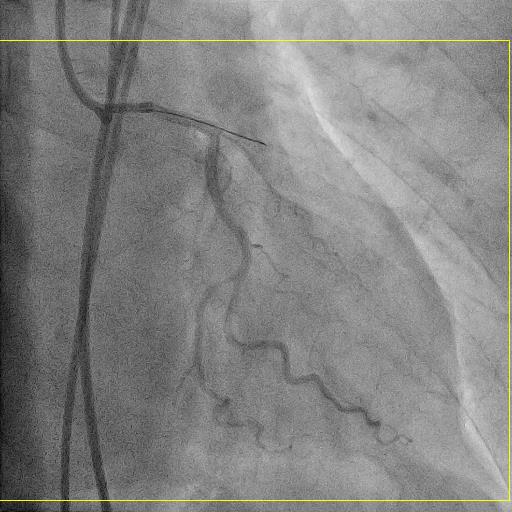
Proceeded with PCI to ostial LAD total occlusion via double femoral puncture to anticipate retrograde approach. 7Fr sheath with 7Fr XB3 SH catheter for antegrade system. 6Fr sheath with 6Fr JR4 for retrograde system. Wired down across ostial LAD total occlusion with Asahi Sion Blue wire with microcatheter support Sasuke. Initial predilation with Genose 2.5 X 15mm up to 8atm. Further predilate with Scoreflex NC 3.0 X 15mm up to 8atm for 20 seconds. Ostial LAD lesion was treated with Magic touch 3.0 X 20mm at 8atm for 60sec. No ECG changes and chest pain. Final result was TIMI 3 flow, no perforation and no dissection. Contrast was 150ml. Patient was able to discharge the next day uneventful.
Case Summary
Despite ostial LAD total occlusion, J-CTO score was 1 with short lesion length. Lesion preparation was done with 2 different types and sizes of balloons. Lesion was prepared with slow predilatation to obtain control dissection. DCB approach in this case was also favorable in view of short DAPT duration in the clinical context of octogenarian and anemia. Therefore, this demonstrate the importance to have knowledge on patient selection with appropriate indication for DCB. It is also vital to be able to define target lesion characteristic such as length and complexity. Lesion preparation with patience and precision are upmost important to get immediate and long term good result.