
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-201
Percutaneous Rescue of a Transcatheter Aortic Valve Implantation Nightmare
By Huda Abu-Own, Siu Fung Wong, David Hildick-Smith
Presenter
Siu Fung Wong
Authors
Huda Abu-Own1, Siu Fung Wong1, David Hildick-Smith1
Affiliation
Royal Sussex County Hospital, United Kingdom1,
View Study Report
TCTAP C-201
Structural - Aortic Valve Intervention - Complex TAVR
Percutaneous Rescue of a Transcatheter Aortic Valve Implantation Nightmare
Huda Abu-Own1, Siu Fung Wong1, David Hildick-Smith1
Royal Sussex County Hospital, United Kingdom1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
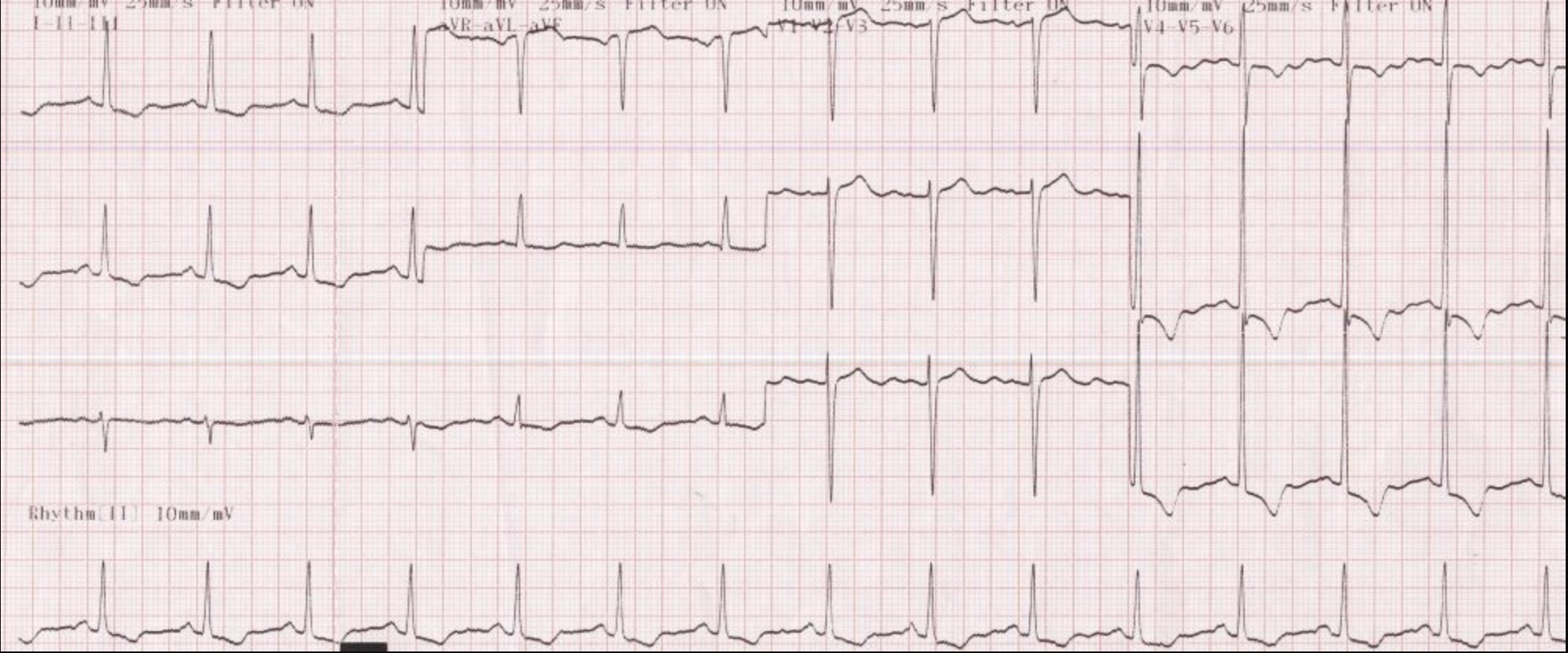
A 77-year-old man presented with activity limiting shortness of breath on exertion suggestive of New York Heart Association Class 2 symptoms of heart failure. Physical examination revealed a harsh ejection systolic murmur and mild peripheral edema. Electrocardiogram showed evidence of left ventricular hypertrophy.
Relevant Test Results Prior to Catheterization
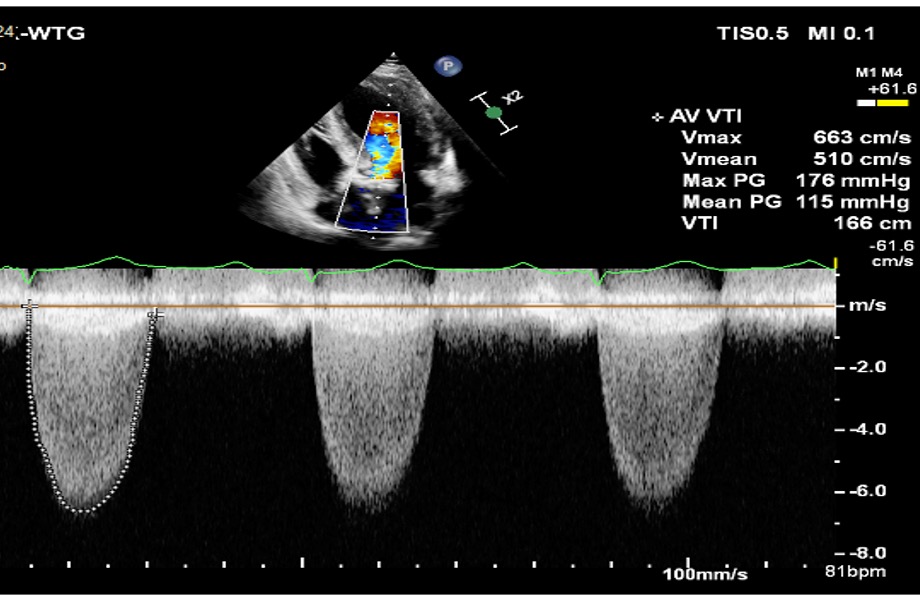
Echocardiography showed a very severe aortic stenosis with peak velocity of 6.6 m/s and a mean gradient of 115 mmHg. The left ventricle was hypertrophied with an ejection fraction of 45%.
Relevant Catheterization Findings
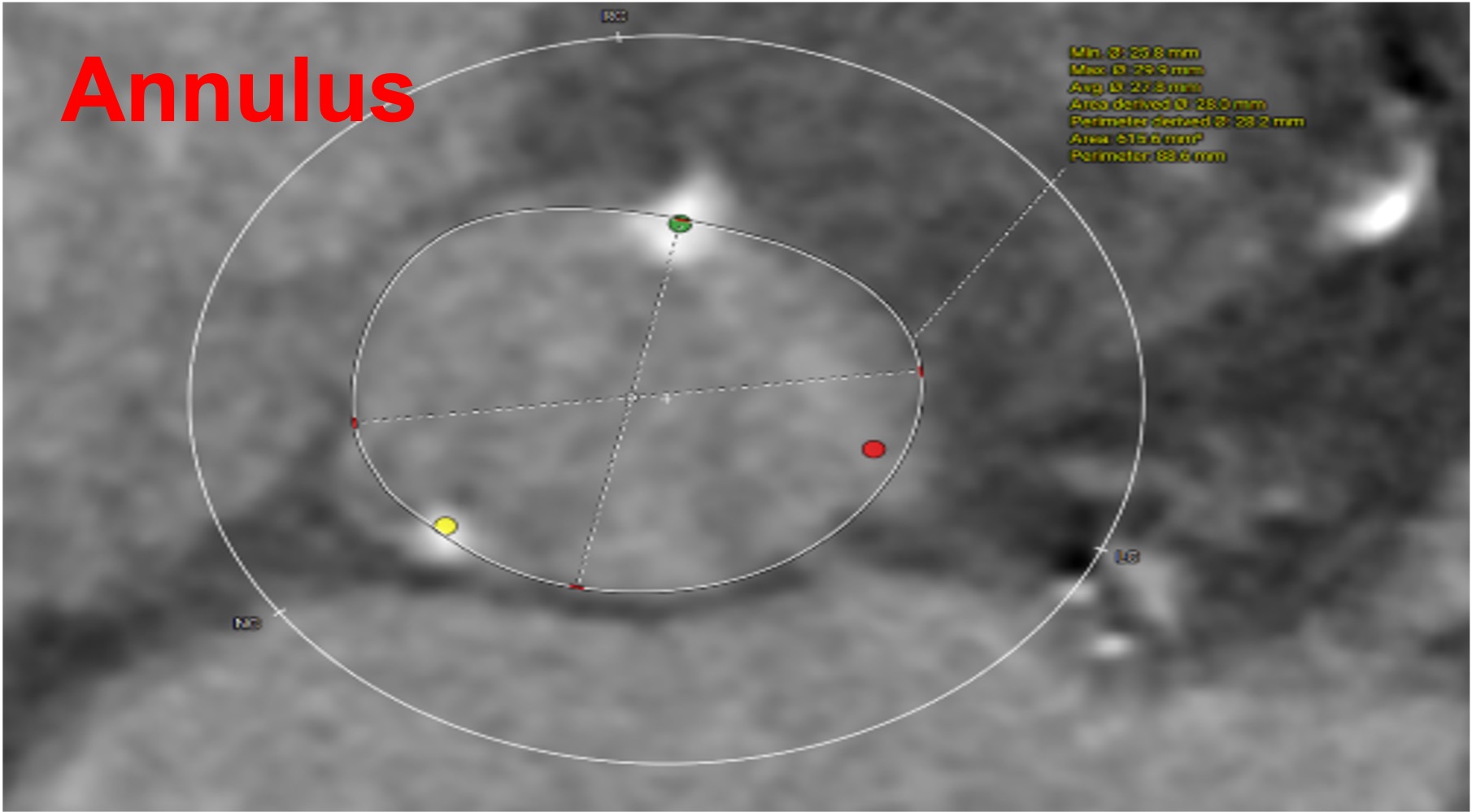
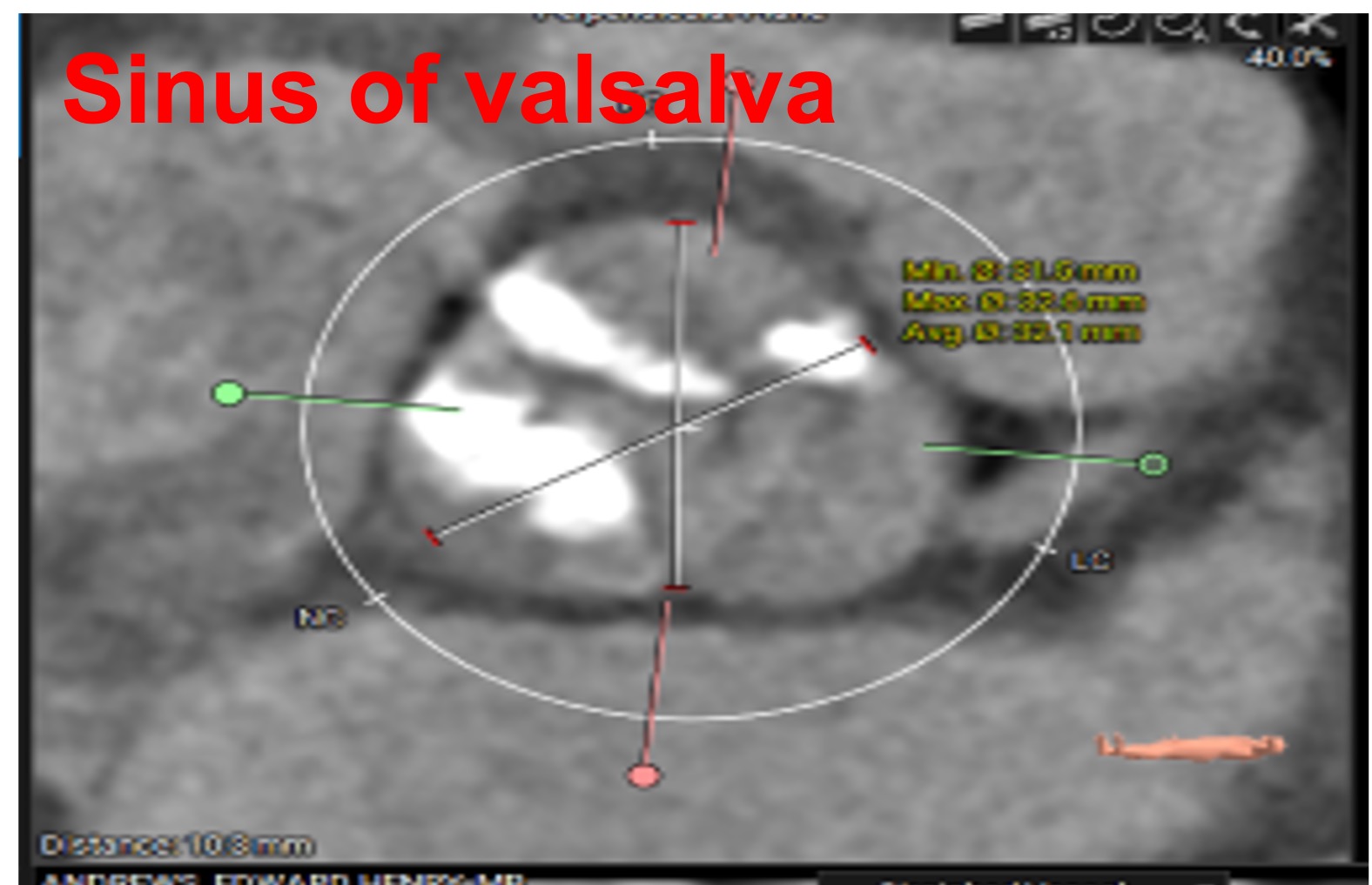
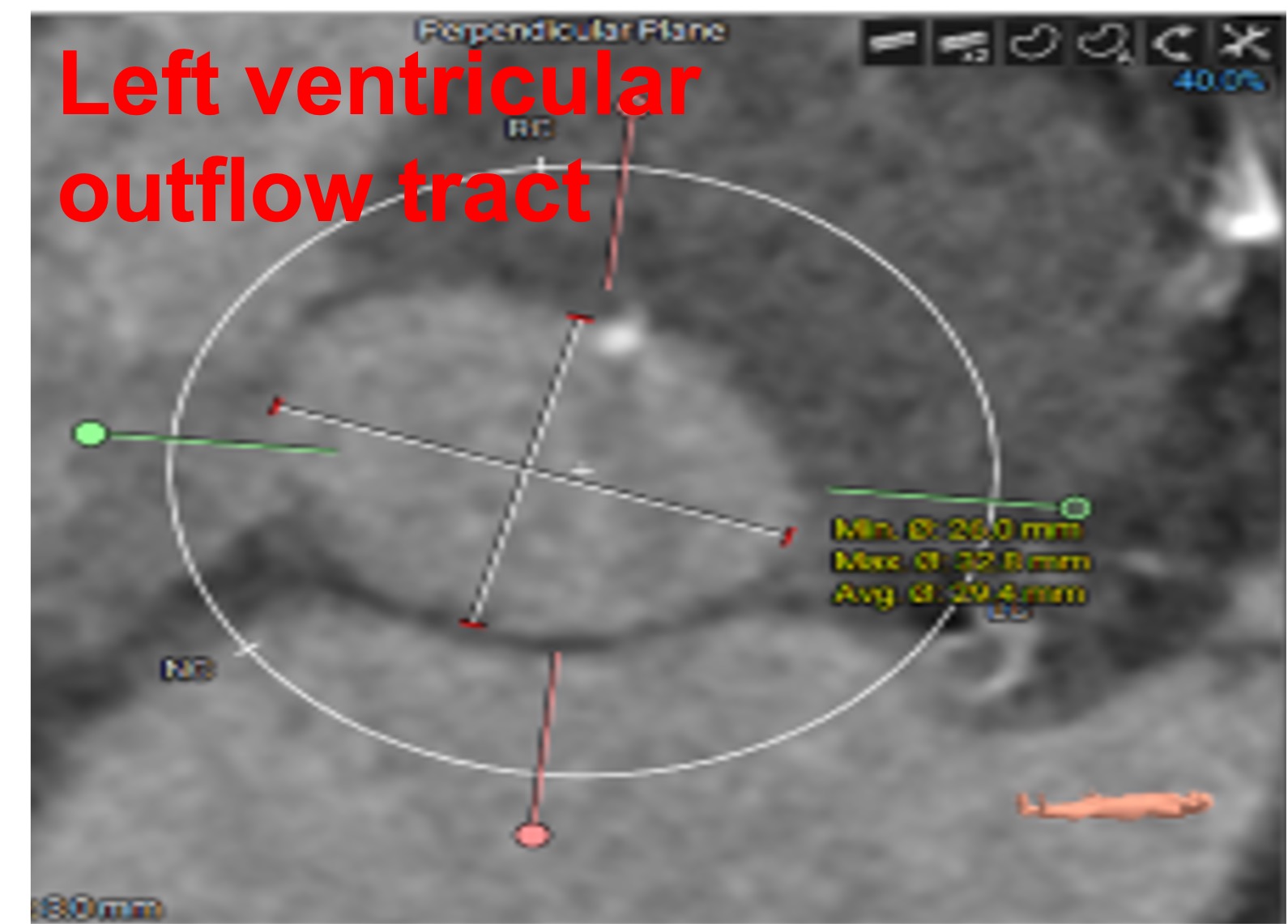
Transcatheter aortic valve implantation (TAVI) was determined after Heart Team meeting. Pre-TAVI computed tomography showed extensive leaflet calcification with 3-dimensional annular area of 615 mm2. A 29 mm Sapien S3 Ultra (Edwards Lifesciences, US) transcatheter heart valve (THV) was chosen.
Interventional Management
Procedural Step
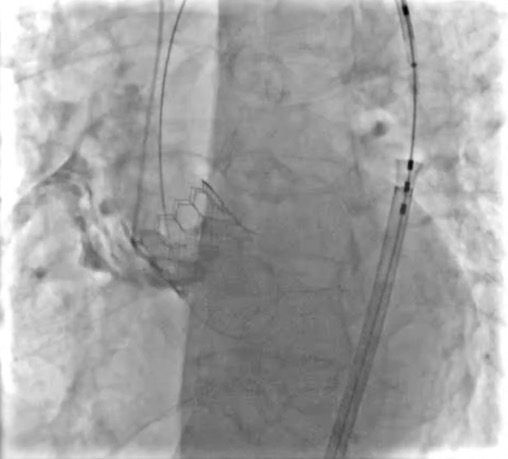
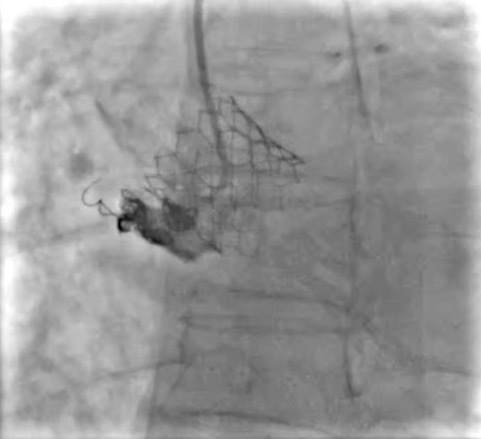
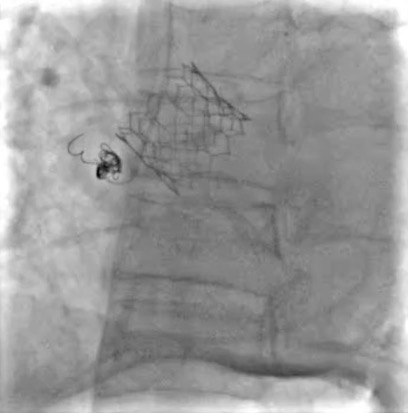
A Sentinel embolic protection device (Boston Scientific, US) was inserted for cerebral protection. Balloon aortic valvuloplasty was performed with a 24 mm True dilatation balloon (BD, US) prior to implantation of the THV, under rapid ventricular pacing over Safari wire (Boston Scientific, US). This was followed by the insertion of the 29 mm Sapien 3 Ultra THV. Patient developed hypotension immediately after THV deployment. Aortography showed annular rupture with contrast extravasation into the pericardium causing cardiac tamponade. Emergent pericardiocentesis was performed. Selective injection of contrast revealed rupture at the right coronary cusp. The leaking channel was subsequently wired with a Runthrough Floppy (Terumo, Japan) coronary wire, followed by introduction of a microcatheter. Two 3/10 and 8/30 mm coils were deployed in the tract of rupture. Complete sealing was achieved with absence of further contrast extravasation on final aortography. The hemodynamic condition of the patient was stabilized with no residual pericardial effusion on echocardiography.
Case Summary
Annular rupture is a rare but life-threatening complication of TAVI with limited treatment options including conservative management with pericardiocentesis, surgical repair, or second valve implantation. While surgical repair carries a high mortality, percutaneous approach such as coiling serves as a timely and viable bailout of such circumstance.