
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-149
Successful Rotational Atherectomy and Intravascular Lithotripsy in the Setting of Extensive Coronary Dissection: A Case of Failed Balloon Angioplasty in a Non Dilatable Calcified Lesion
By Raj Pratap Singh, Himanshu Rana
Presenter
Himanshu Rana
Authors
Raj Pratap Singh1, Himanshu Rana1
Affiliation
Graphic Era Institute, India1,
View Study Report
TCTAP C-149
Coronary - Complication Management
Successful Rotational Atherectomy and Intravascular Lithotripsy in the Setting of Extensive Coronary Dissection: A Case of Failed Balloon Angioplasty in a Non Dilatable Calcified Lesion
Raj Pratap Singh1, Himanshu Rana1
Graphic Era Institute, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
•65yearold female, known case of Systemic Hypertension.
•
•Chestdiscomfort on exertion since one year.
•PhysicalExam: Unremarkable.
•
•ECG:Sinus Rhythm, q waves inferior leads, Twaveinversion I and aVL.
•
•Echo:Regional wall motion abnormality of inferior and anterior wall, moderate LVsystolic dysfunction, EF-35%
Relevant Test Results Prior to Catheterization
Patientswith LHCC undergoing PCI:
•lesslikely to receive complete revascularization (48% vs. 55.6%; p < 0.001).
•
morelikely to die subsequently (10.8% vs. 4.4%; p < 0.001Relevant Catheterization Findings
Right coronary artery beingsupplied by collaterals from the left anterior descending and left circumflexartery


Interventional Management
Procedural Step
Right coronary artery was engaged with7Fr JR 3.5 GC and wired with 014 Fielder XT wire.
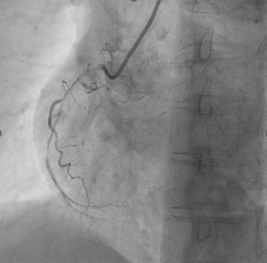
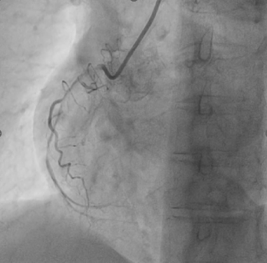
Pre-dilationwith 1.5x15mm compliant balloon. (Balloon didn’t go beyond this point).Changed to workhorse wire insidemicrocatheter by trapping the wire. Coronary dissection NHLBI- Type D/F seenwith reduced antegrade flow
2.0x12mmcompliant balloon didn’t cross proximal RCA, dilated at 10 atmand it ruptured.
With rotational speed of 170 000 rpmrotational atherectomy was started with 1.5mm burr in Ostioproximal RCA with small pecking motion and short runs (total duration of 3 minutes 42seconds, 20 seconds runs)
Intermittent checks were done tolook for any complications
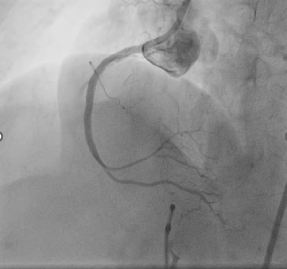
Finallywe were able to cross the tight part in proximal RCA followed by mid RCA
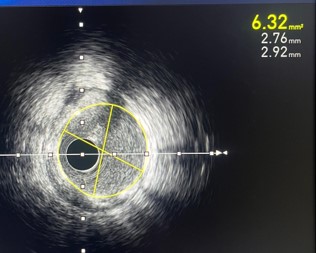
Post rotational atherectomyangiogram and IVUS run taken
In view of 300-360 degrees ofcalcium arc and not good MLAs in mid and proximal RCA post ROTA we decided todo Intravascular lithotripsyIntravascular lithotripsy with 3.0x12mm balloon done in mid and proximal RCA
DES 2.75x28 deployed in mid-distalRCA
DES 3.0x38 deployed in ostioproximal-midRCA
Cracksin proximal RCA calcium arc
.

Pre-dilationwith 1.5x15mm compliant balloon. (Balloon didn’t go beyond this point).Changed to workhorse wire insidemicrocatheter by trapping the wire. Coronary dissection NHLBI- Type D/F seenwith reduced antegrade flow
2.0x12mmcompliant balloon didn’t cross proximal RCA, dilated at 10 atmand it ruptured.
With rotational speed of 170 000 rpmrotational atherectomy was started with 1.5mm burr in Ostioproximal RCA with small pecking motion and short runs (total duration of 3 minutes 42seconds, 20 seconds runs)
Intermittent checks were done tolook for any complications
Finallywe were able to cross the tight part in proximal RCA followed by mid RCA
Post rotational atherectomyangiogram and IVUS run taken
In view of 300-360 degrees ofcalcium arc and not good MLAs in mid and proximal RCA post ROTA we decided todo Intravascular lithotripsyIntravascular lithotripsy with 3.0x12mm balloon done in mid and proximal RCA
DES 2.75x28 deployed in mid-distalRCA
DES 3.0x38 deployed in ostioproximal-midRCA
Cracksin proximal RCA calcium arc
.
Case Summary
• Undilatable calcified lesions athigher inflation pressures can result in balloon rupture and potentiallysignificant dissection.