
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-044
DK Crush Stenting in the Saphenous Vein Graft
By Bu-Yuan Hsiao
Presenter
Bu-Yuan Hsiao
Authors
Bu-Yuan Hsiao1
Affiliation
Taipei Medical University Hospital, Taiwan1,
View Study Report
TCTAP C-044
Coronary - Complex PCI - Bifurcation
DK Crush Stenting in the Saphenous Vein Graft
Bu-Yuan Hsiao1
Taipei Medical University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
The 68 y/o male patient has the past history of Hypertensive cardiovascular disease, and Hyperlipidemia.He received CABG (LIMA to LAD, SVG to OM, SVG to RCA) in 2004.He received regular follow-up in our CVS OPD. But he suffered effort angina for several times in recent one month.These symptoms subsided when taking a rest. He did not have orthopnea or symptoms of heart failure.
Relevant Test Results Prior to Catheterization
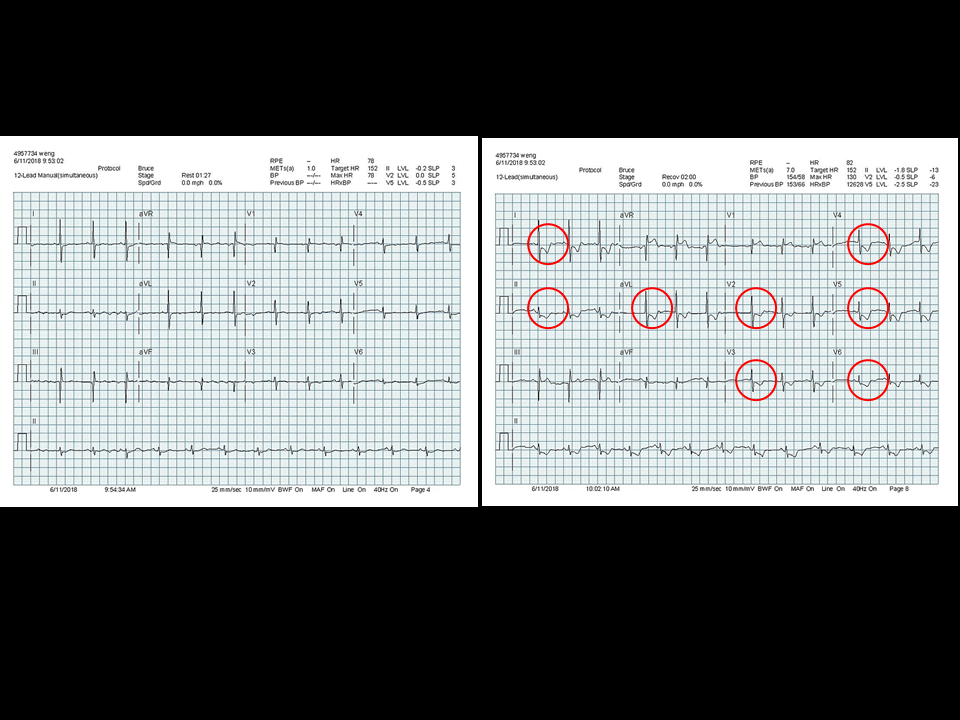
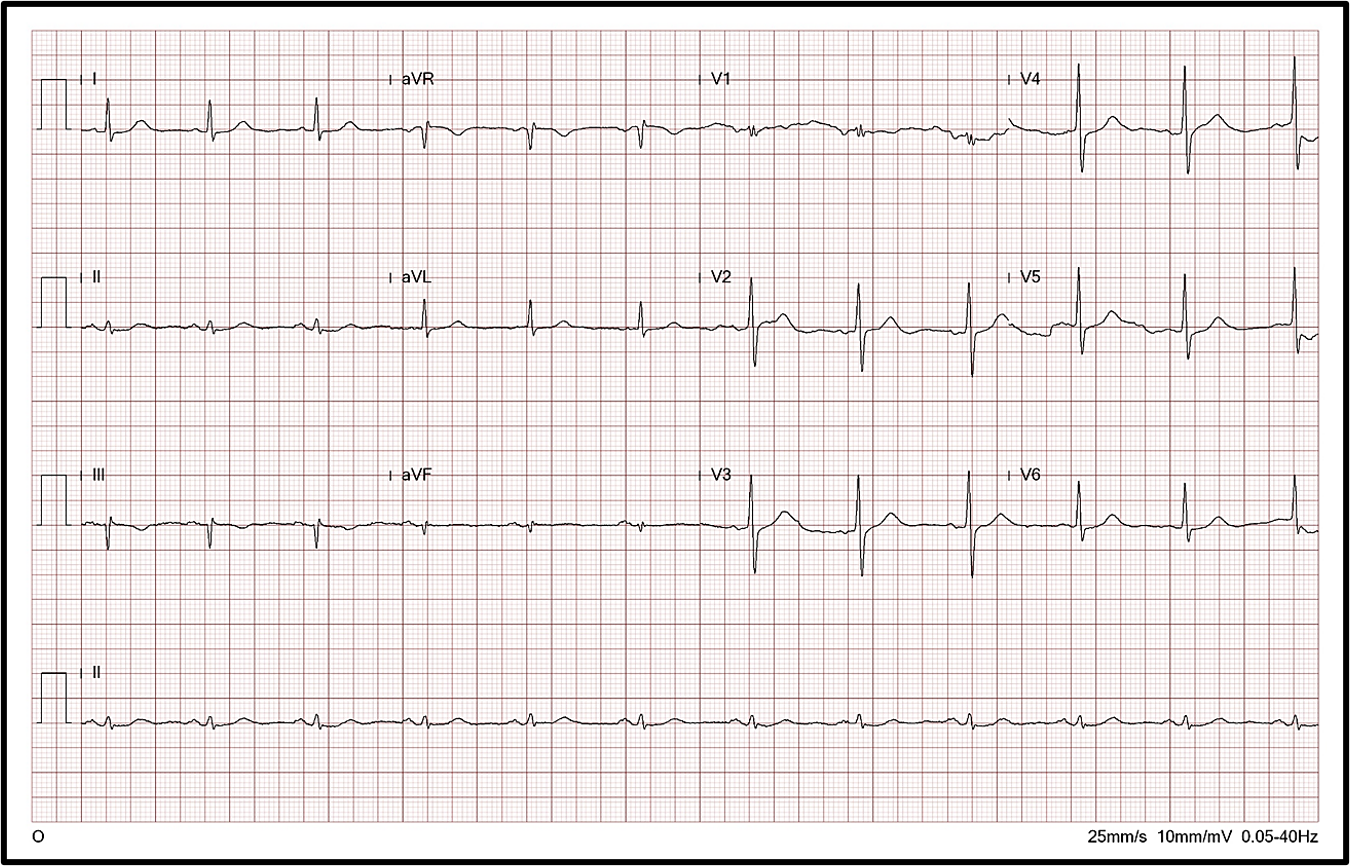
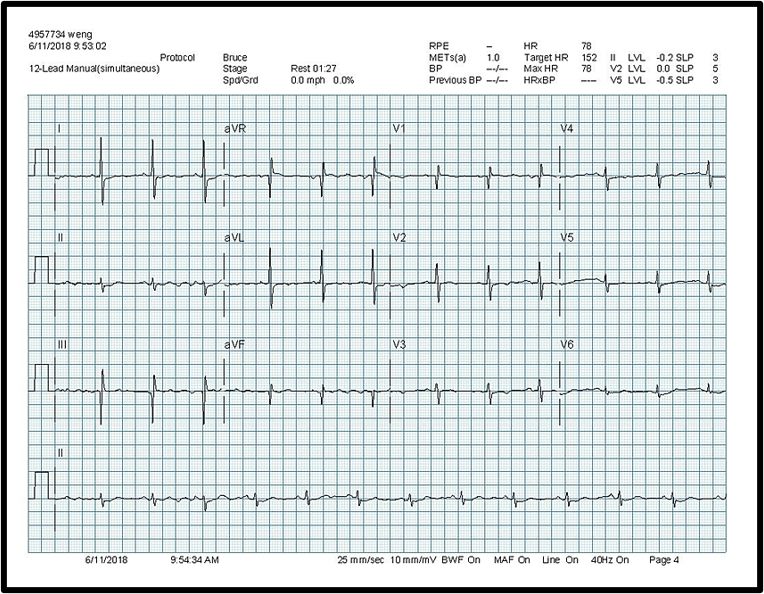
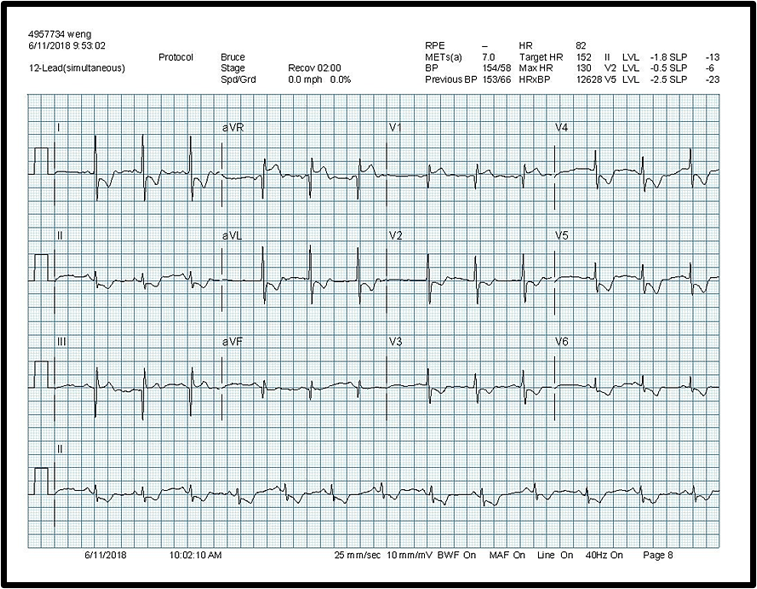
ECG showed sinus rhythm, but no ischemic changes.Treadmill Stress Testing: Strongly positive.Echocardiography: Preserved global systolic function.
Relevant Catheterization Findings
LM: D/3 50~60% eccentric narrowing.LAD: Orifice 80% stenosis, P/3 75% stenosis, M/3 total occlusion.LCx: Orifice 50% stenosis, P-M/3 tandem lesions with 85-95% stenosis.RCA: P/3 CTO.LIMA to LAD: Failure.SVG to OM: Failure.SVG to RCA: Bifurcation lesions (Medina 1,1,1) with 90~95% stenosis.
Interventional Management
Procedural Step
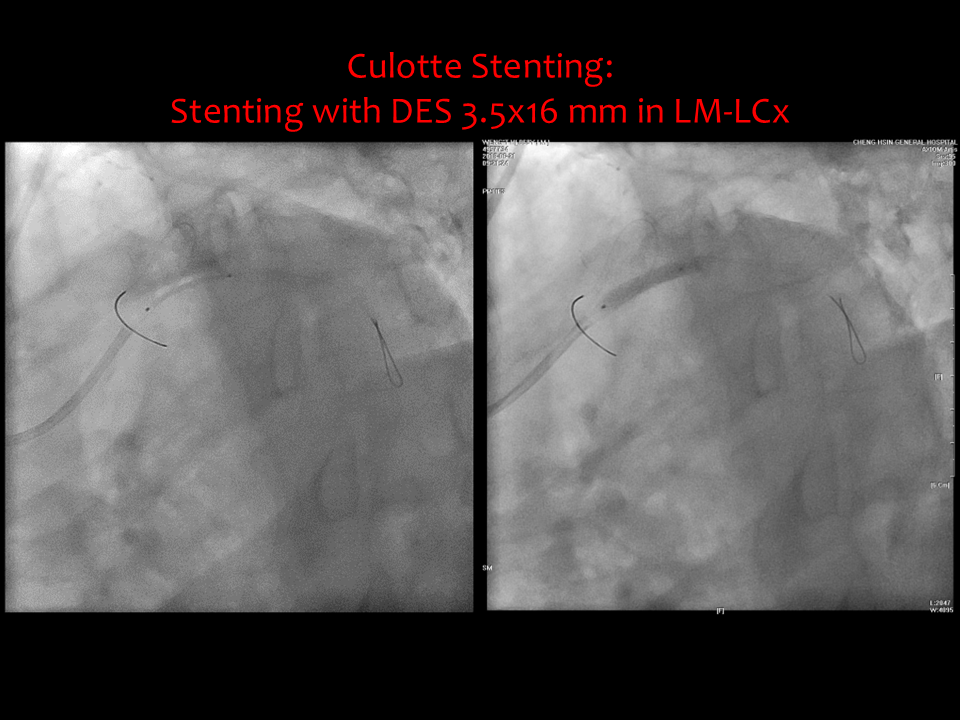
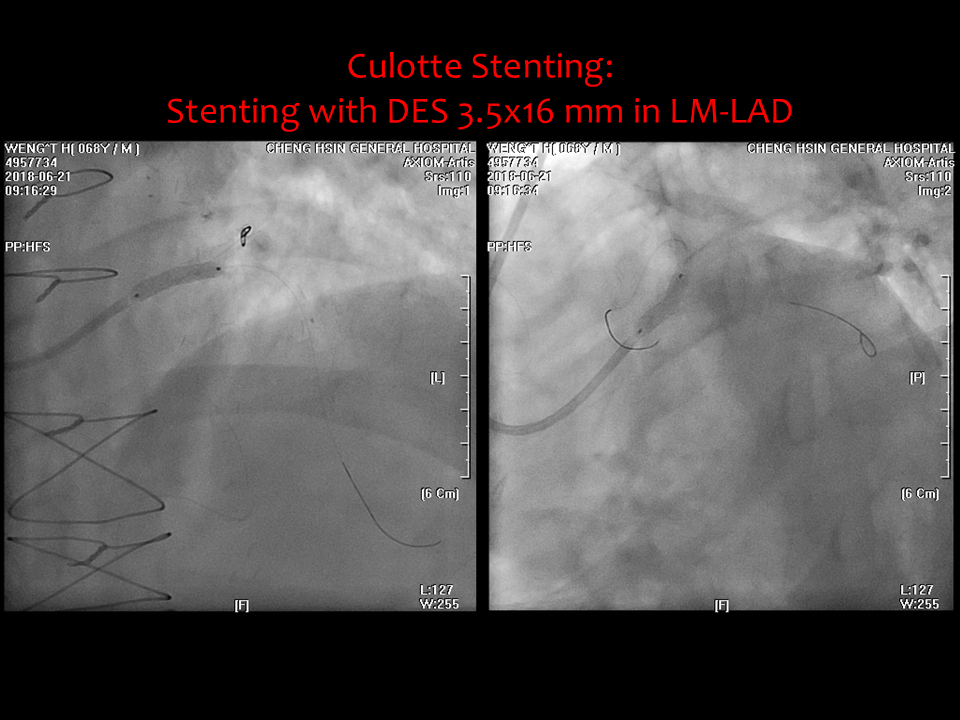
(1) POBA followed by stenting with DES 2.75x30 mm in LCx.(2) Stenting with DES 2.75x26 mm in the proximal LAD.(3) Culotte Stenting: Stenting with DES 3.5x16 mm in LM-LCx, Stenting with DES 3.5x16 mm in LM-LAD. And followed by kissing balloon technique.(4) DK Crush Technique with DES 3.0x12 mm and DES 3.0x24 mm in the SVG. (a) I introduced Spider Fx from SVG to PDA first.
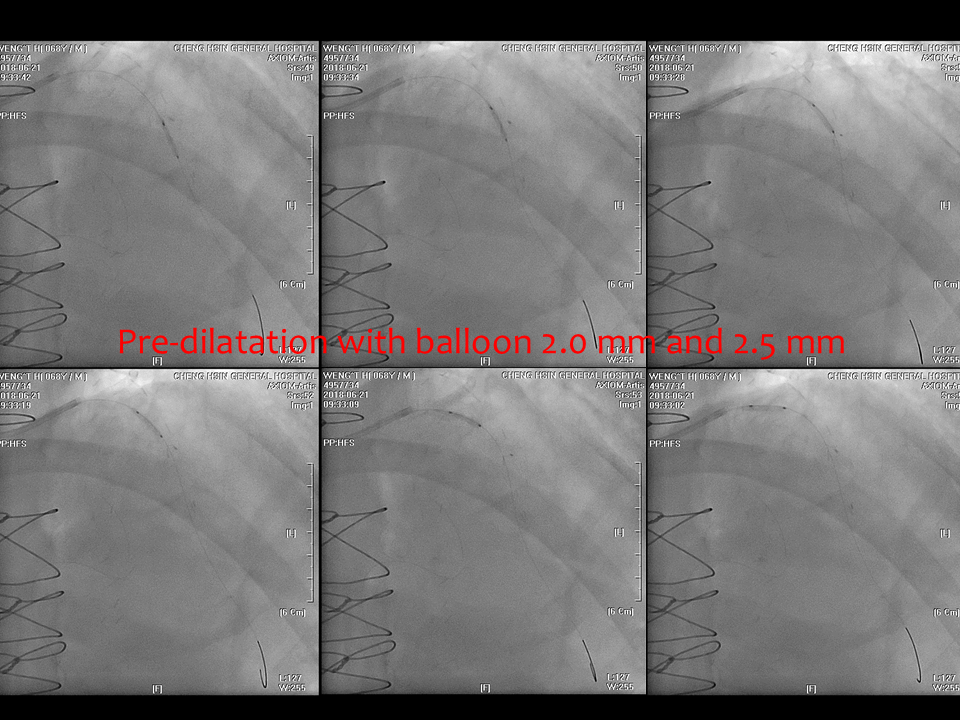
(b) Then I performed POBA with balloon 3.0x15 mm for the bifurcation lesions.
(c) Stenting with DES 3.0x12 mm in the PDA followed by 1st kissing.
(d) Stenting with DES 3.0x24 mm in the PDA followed by 2nd kissing.
(e) POT with balloon 3.5x12 mm.
Case Summary
(1) The DK Crush stenting technique proved to be an effective and reliable approach for complex SVG lesions post-CABG, achieving excellent revascularization with sustained side branch patency and reduced restenosis risks. (2) Its success underscores the importance of meticulous planning and technical expertise, demonstrating its value in addressing challenging cases. (3) These findings highlight the potential of DK Crush as a preferred strategy in SVG interventions and emphasize the need for further long-term studies to validate its broader clinical application.