
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-144
Management of Life Threatening Guidewire-Induced Coronary Perforation Using Handmade Coil
By Puspita Sari Bustanul Watoni, Masrul Syafri, Muhammad Syukri
Presenter
Puspita Sari Bustanul Watoni
Authors
Puspita Sari Bustanul Watoni1, Masrul Syafri1, Muhammad Syukri1
Affiliation
RSUP Dr. M. Djamil Hospital, Indonesia1,
View Study Report
TCTAP C-144
Coronary - Complication Management
Management of Life Threatening Guidewire-Induced Coronary Perforation Using Handmade Coil
Puspita Sari Bustanul Watoni1, Masrul Syafri1, Muhammad Syukri1
RSUP Dr. M. Djamil Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 60-year-old female, admitted from outpatient clinic with CCS class III stable angina pectoris for 6 months. Her cardiovascular risk factors were hypertension and diabetes. Her vital signs upon arrival were blood pressure of 140/80 mmHg and heart rate of 65 bpm. There were no abnormal lung sounds and her peripheral perfusion was normal.
Relevant Test Results Prior to Catheterization
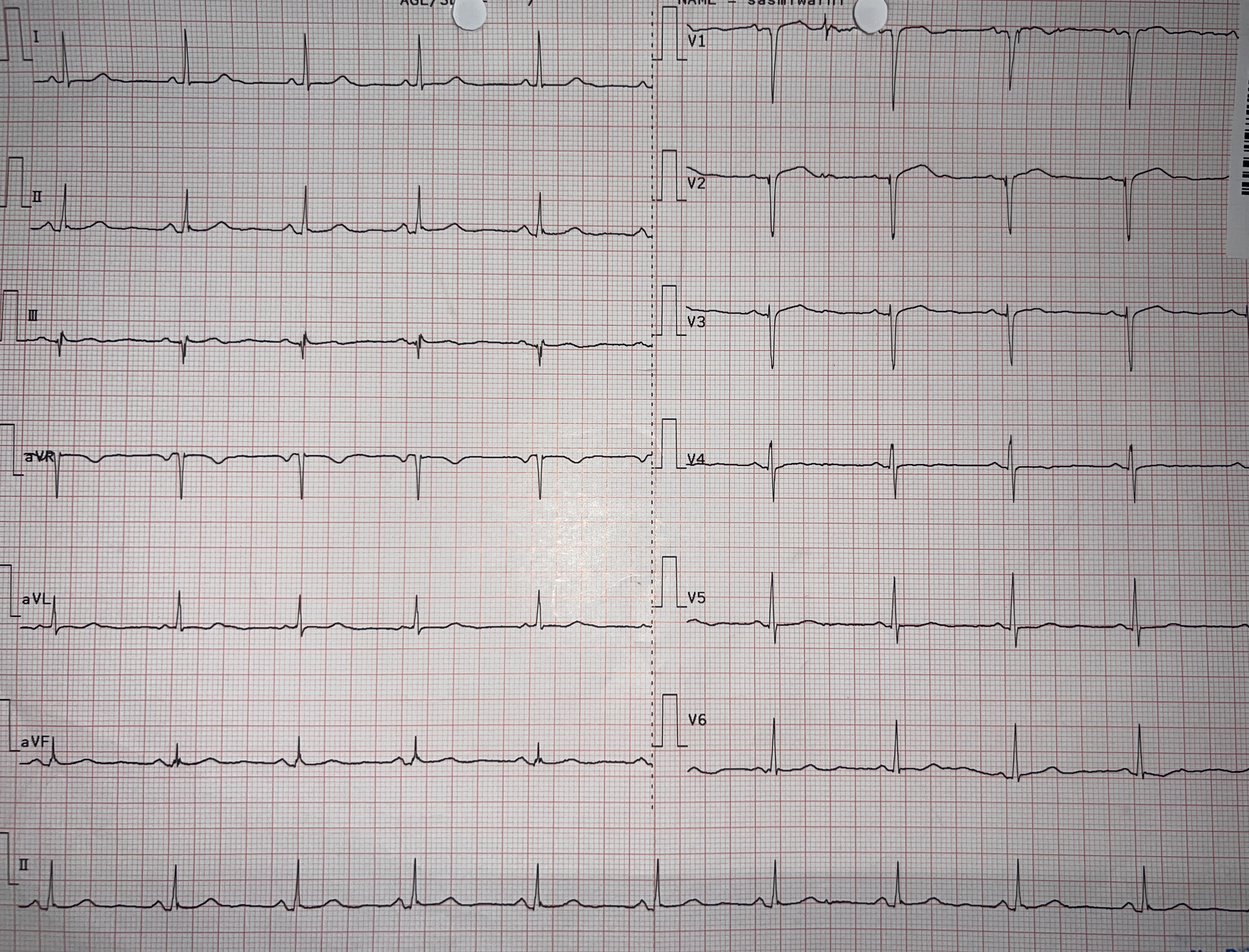
Her ECG showed normal sinus rhytm with poor R wave progression in anterior lead. Her echocardiography showed mildly reduced LV systolic function with LV ejection fraction of 51%, hypokinetic at mid anteroseptal, apikoseptal, apical cap, with other segments normokinetic, concentric LVH with mild LV diastolic dysfunction. Her notable laboratory findings were fasting glucose levels of 159 mg/dL and post prandial glucose of 282 mg/dL.
Relevant Catheterization Findings
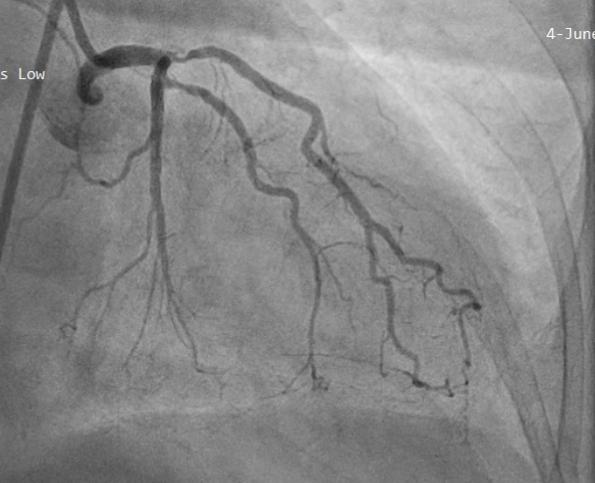
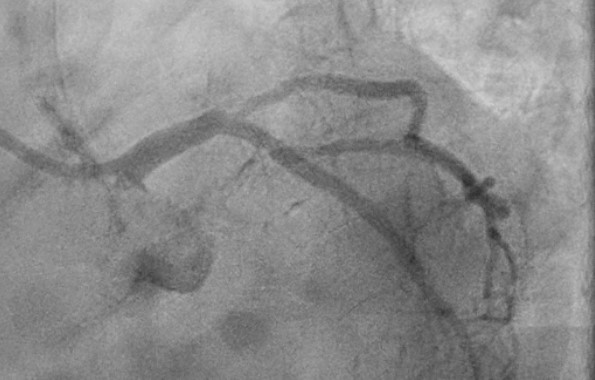
Left coronary angiography showed chronic total occlusion (CTO) of ostial left anterior descending artery (LAD), severe stenosis in proximal of intermediate artery, and mild irregularity of obtuse marginal branch. Right coronary angiography showed subtotal stenosis in proximal part and diffuse stenosis in mid-distal part of right coronary artery (RCA), with conal branch and distal RCA supplied collaterals to mid-distal LAD.

Interventional Management
Procedural Step
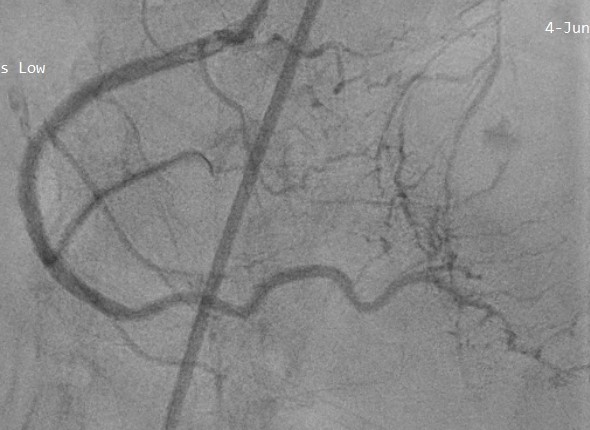
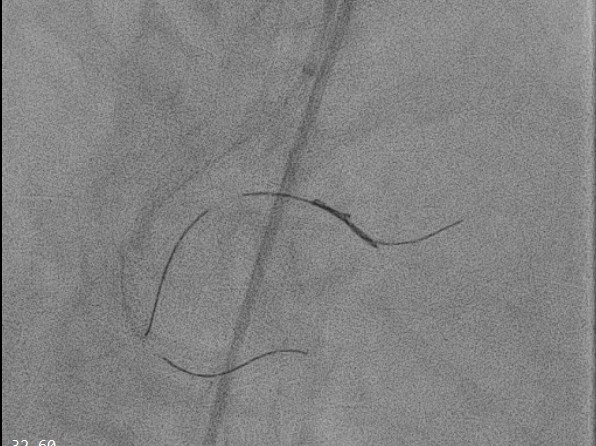
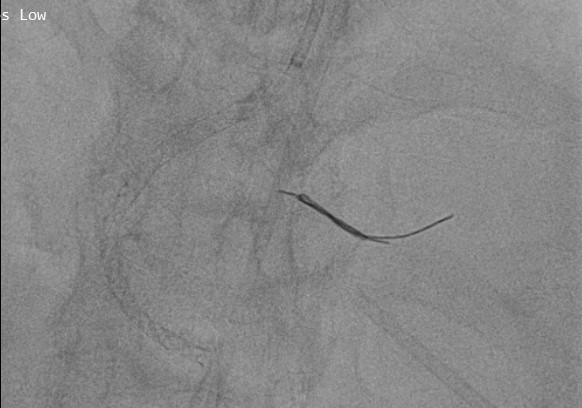
PCI of the RCA was performed using a JR 3.5/7 F catheter and a Runthrough Hypercoat guidewire. The lesion was crossed to the PLB, and NC balloons was used for lesion preparation (3.0x15 mm in the proximal RCA and 2.0x15 mm in the mid-distal RCA). A 3.0x38 mm DES was deployed in ostial-mid RCA, overlapping with a 2.75x46 mm DES in mid-distal RCA, achieving excellent angiographic results. However, a coronary perforation (Ellis type III) was noted in the distal PLB, leading to worsening chest pain, dizziness, and cardiac arrest. CPR was promptly administered, the patient was successfully resuscitated, and bedside echocardiography revealed moderate pericardial effusion. Emergency pericardiocentesis via the apical approach with a 5F radial sheath was performed, and aspirated blood was retransfused via the femoral vein.Persistent contrast extravasation necessitated prolonged balloon inflation (NC 1.5x15 mm), which eventually failed, leading to the use of a handmade coil due to the unavailability of a commercial coil. A fragment of the Runthrough guidewire was cut, inserted into a microcatheter, and placed at the perforation site multiple times. Final angiography showed reduced extravasation, and echocardiography indicated mild pericardial effusion. During the procedure, 2 liters of blood were aspirated and retransfused. The patient was stabilized with vasopressors, PRC, and FFP, showing continued improvement and being discharged in good clinical condition after five days.
Case Summary
Guidewire-induced coronary perforation can lead to life threatening complication and management requires early detection and achieving hemostasis using various methods.In most cases, definitive treatment with coil embolization is preferred. However, when commercial coil is unavailable, operators need to improvise devices. In this case, we successfully sealed the perforation using a handmade coil created from available devices. For interventional cardiologist, it is crucial knowing how to manage wire perforation during PCI and to prevent perforations by monitoring the position of the distally advanced guidewire.