
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-236
Successful Catheter-Directed Thrombolysis for Massive Pulmonary Embolism in a Patient With Recent Cerebral Hemorrhage
By Cuong Tran, Duc Chinh Nguyen, Chi Quyen Mach, Xuan Bach Cao, Thi Thao Trang Nguyen, Duc Cam Tran, Duong Khanh Nguyen, Mai Hoang, Loc Vu, Thach Nguyen
Presenter
Chi Quyen Mach
Authors
Cuong Tran1, Duc Chinh Nguyen1, Chi Quyen Mach1, Xuan Bach Cao1, Thi Thao Trang Nguyen1, Duc Cam Tran1, Duong Khanh Nguyen1, Mai Hoang2, Loc Vu2, Thach Nguyen2
Affiliation
Can Tho Stroke International Services General Hospital, Vietnam1, Tan Tao University, Vietnam2,
View Study Report
TCTAP C-236
Endovascular - Other Endovascular Intervention
Successful Catheter-Directed Thrombolysis for Massive Pulmonary Embolism in a Patient With Recent Cerebral Hemorrhage
Cuong Tran1, Duc Chinh Nguyen1, Chi Quyen Mach1, Xuan Bach Cao1, Thi Thao Trang Nguyen1, Duc Cam Tran1, Duong Khanh Nguyen1, Mai Hoang2, Loc Vu2, Thach Nguyen2
Can Tho Stroke International Services General Hospital, Vietnam1, Tan Tao University, Vietnam2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
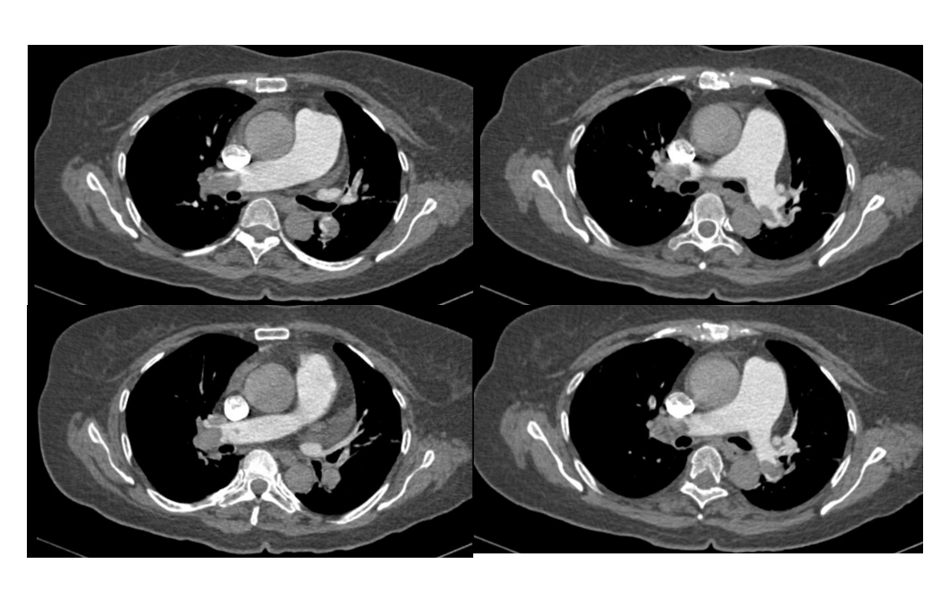
A 62-year-old female presented with sudden convulsions in all four limbs, lasting less than 1 minute. After the event, she became lethargic, fatigued, and experienced rapid breathing. The patient was admitted to the hospital 4 hours later with a history of cerebral hemorrhage from a ruptured aneurysm 20 days prior (pic 1&2), for which she underwent surgical clipping. She also had a 10-year history of hypertension. She showed signs of left-sided hemiparesis but had no peripheral edema.
Relevant Test Results Prior to Catheterization
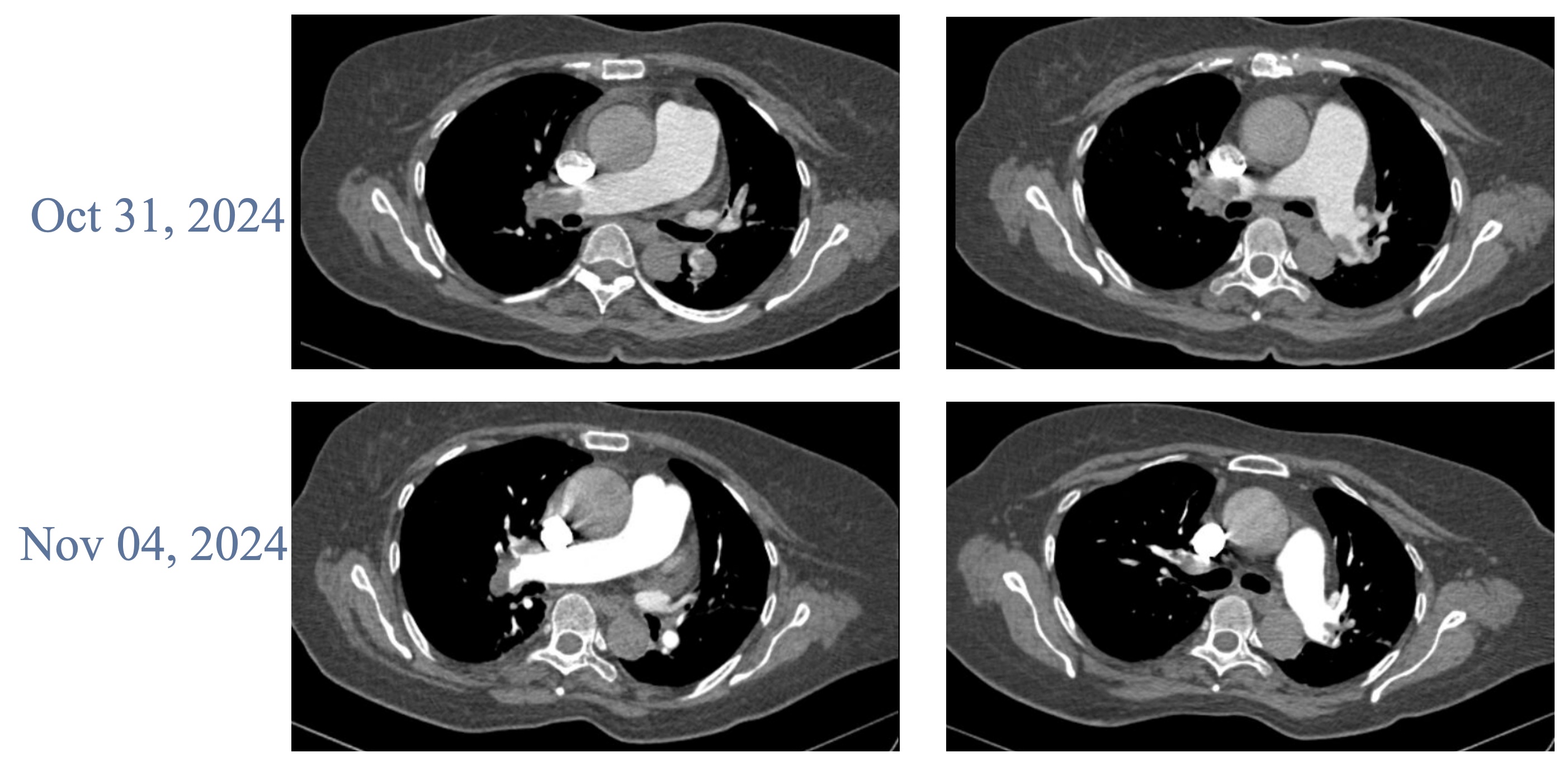
The D-dimer levels (1028.7 ng/ml), NT-proBNP (609.4 pg/ml), and Troponin I (0.16 pg/ml) were elevated. Echocardiography revealed right ventricular dilatation (RVd = 48 mm), severe tricuspid regurgitation (3/4), and elevated PAPs = 55 mmHg. A leg ultrasound showed a complete thrombus in left superficial femoral vein, the great and small saphenous veins. A CT scan revealed a total thrombus in the right pulmonary artery and partial thrombus in the left pulmonary artery.

Relevant Catheterization Findings
The patient underwent pulmonary artery catheterization due to a diagnosis of high-risk pulmonary embolism. Imaging revealed a large thrombus in the right main pulmonary artery and partial thrombus in the left artery, causing near-total obstruction.
Interventional Management
Procedural Step
Initial attempts to aspirate the clot were unsuccessful, and a catheter was placed in the right pulmonary artery for local thrombolysis with Actilyse at a rate of 1mL/h over 24 hours. Hemodynamic monitoring showed pulmonary artery pressure at 60/25 mmHg pre-thrombolysis. Post-thrombolysis, pulmonary pressures decreased, and follow-up imaging revealed a reduction in clot burden, with improved right ventricular size (RVd decreased from 48 mmHg to 31 mmHg) and a reduction in tricuspid regurgitation severity, PAPs dropped from 55 mmHg to 18 mmHg.
Case Summary
With the massive PE and high risk for hemorrhage, in hospitals with adequate equipment, thrombectomy or mechanical thrombectomy can be performed. At the small hospital with limited equipment, low-dose local rTPA could be considered after multidisciplinary consultation, although it is contraindicated. Particularly, the patient's hemodynamics were unstable, leaving only one option.This case showed that when the cause of cerebral hemorrhage has been resolved, low-dose rTPA (1 mg/hour for 24 hours) can be safe and effective