
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-165
The First Long-Term Imaging Analysis of the Use of Bioadaptor in Chronic Total Occlusion Intervention: Insights From a Single-Centre Adapt-CTO Registry
By Chun-Yat Fung, Tak-Shun Chung, Siu-Fung Wong
Presenter
Chun-Yat Fung
Authors
Chun-Yat Fung1, Tak-Shun Chung1, Siu-Fung Wong1
Affiliation
United Christian Hospital, Hong Kong, China1,
View Study Report
TCTAP C-165
Coronary - DES/BRS/DCB
The First Long-Term Imaging Analysis of the Use of Bioadaptor in Chronic Total Occlusion Intervention: Insights From a Single-Centre Adapt-CTO Registry
Chun-Yat Fung1, Tak-Shun Chung1, Siu-Fung Wong1
United Christian Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
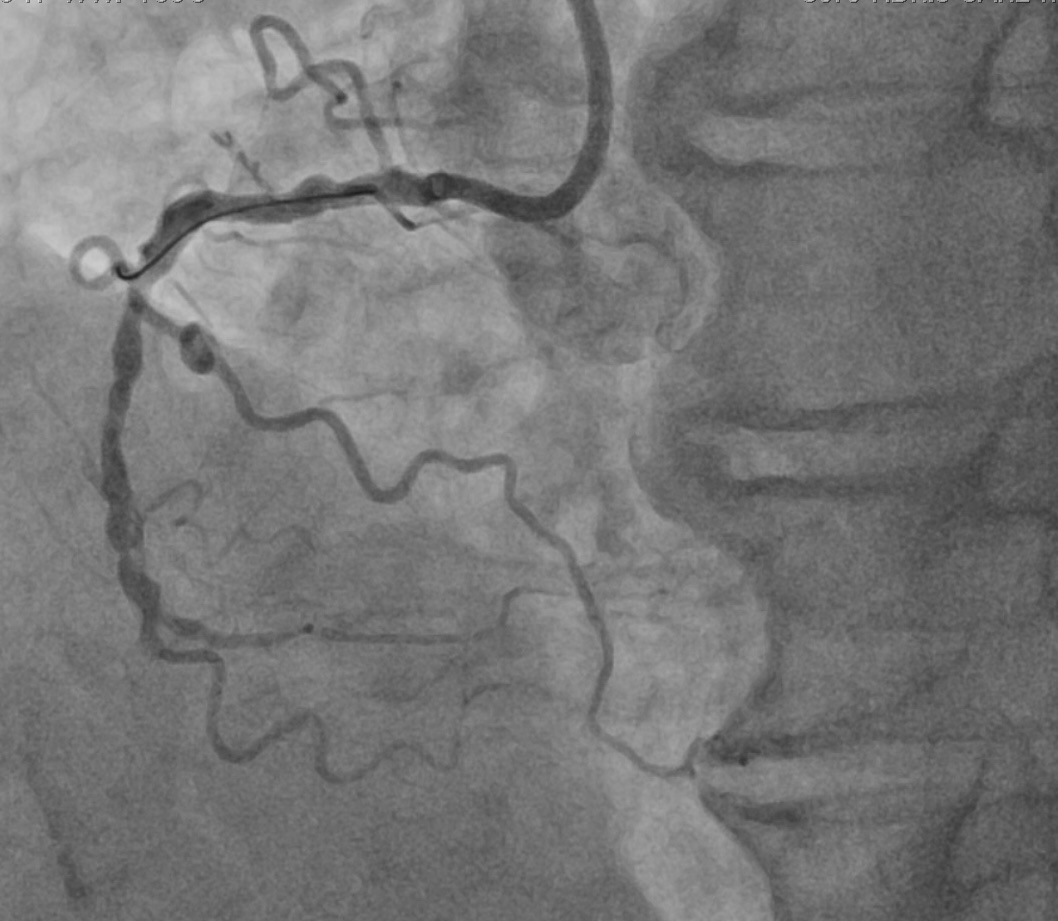
A 58 years old man with background of hypertension was referred to our unit for activity limiting angina refractory to medical treatment. Coronary angiogram showed severe triple vessel disease with a distal right coronary artery (dRCA) total occlusion. Echocardiogram showed normal LVEF with no regional wall motion abnormality. He was counselled on revascularization for symptom control and opted for multivessel PCI over CABG as the definitive treatment.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
A 7Fr AL 0.75 guiding catheter was engaged to RCA. dRCA CTO was successfully crossed with a Fielder XTR (Asahi) wire on Turnpike (Teleflex) microcatheter support, exchanged to a Runthrough NS (Terumo) wire and wired to the RPL. The CTO segment was predilated with 2mm semi-compliant ballon with restoration of TIMI 2 flow to RPL.


Case Summary
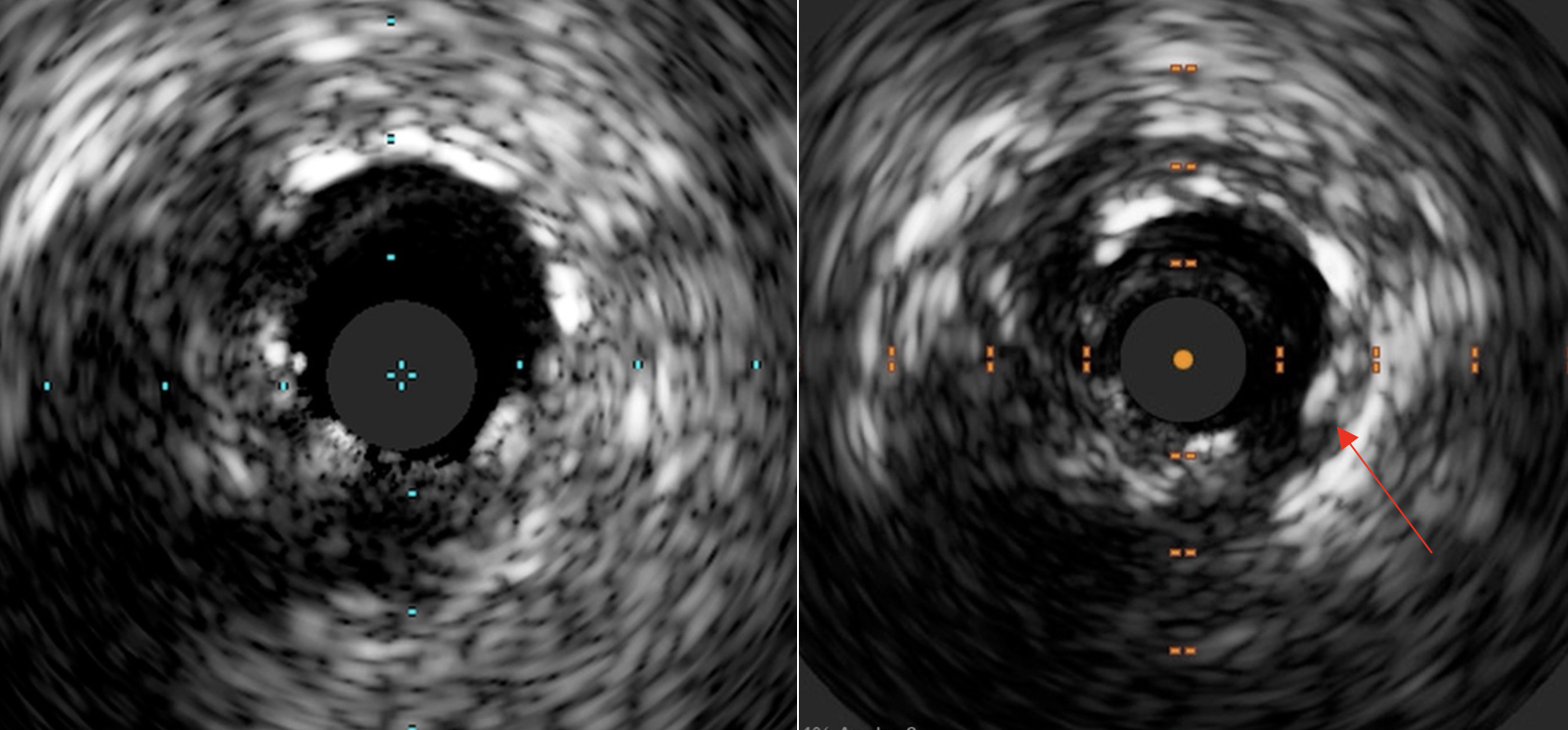
To our best knowledge, this is the first reported case of biopadaptor usage in CTO intervention with a long-term angiographic and intracoronary imaging follow-up. Certain properties of the bioadaptor scaffolds, including the positive adaptive remodelling and restoration of pulsatility of the vessel, was well demonstrated despite in the complex CTO subset of lesion.