
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-007
Managing Undersized Stents in Acute Coronary Syndrome: Insights and Strategies From a Challenging Case of Aneurysmal Right Coronary Artery Lesion
By Wen-Po Chuang, Hao-Yuan Tsai, Ching-Ping Chao
Presenter
Ching-Ping Chao
Authors
Wen-Po Chuang1, Hao-Yuan Tsai1, Ching-Ping Chao1
Affiliation
Far Eastern Memorial Hospital, Taiwan1,
View Study Report
TCTAP C-007
Coronary - ACS/AMI
Managing Undersized Stents in Acute Coronary Syndrome: Insights and Strategies From a Challenging Case of Aneurysmal Right Coronary Artery Lesion
Wen-Po Chuang1, Hao-Yuan Tsai1, Ching-Ping Chao1
Far Eastern Memorial Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
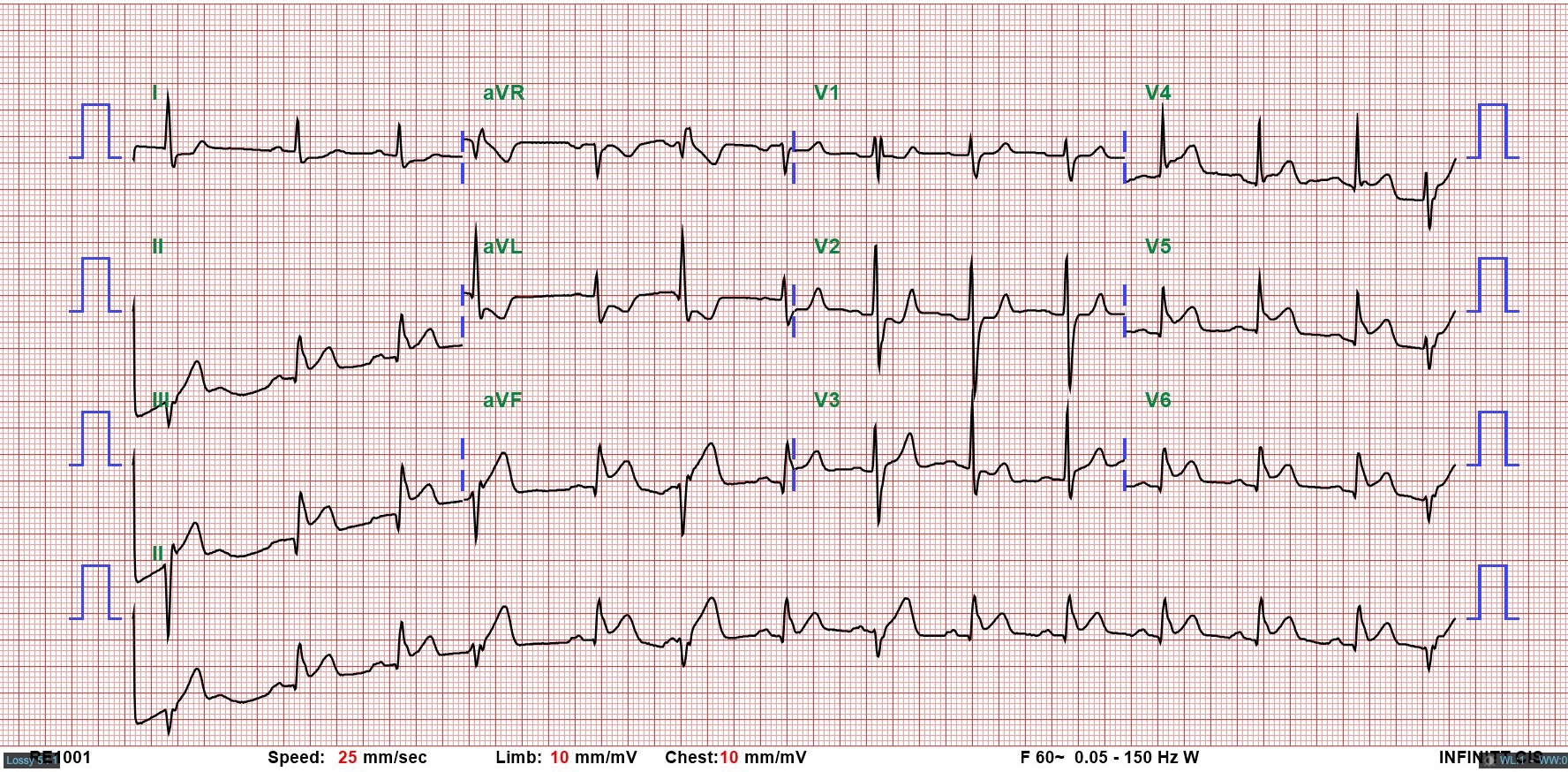
A 42-year-old male, a former smoker with a history of non-ST elevation myocardial infarction (NSTEMI) in 2020, presented with 30 minutes of chest pain and cold sweats. Examination showed stable vital signs, clear breath sounds, and no murmurs. EKG revealed ST elevation in leads II, III, aVF, and V5-V6, with reciprocal changes in leads I and aVL. Echocardiography showed inferior-posterior wall motion abnormalities. Diagnosed with inferior wall STEMI, emergency coronary intervention was arranged.
Relevant Test Results Prior to Catheterization
In 2020, he was admitted for NSTEMI. Emergency coronary angiography showed total occlusion of the right coronary artery (RCA). Initial attempts with a Fielder FC wire failed. Using a Gaia 1 and then Gaia 2 wire with a Progreat microcatheter, the lesion was successfully crossed. Predilatation was done with Euphora balloons (2.0 × 20 mm, 3.0 × 30 mm). Two Xience Sierra stents (3.5 × 38 mm, 3.5 × 15 mm) were deployed, followed by post-dilation with Accuforce balloons (4.0 × 20 mm, 4.5 × 15 mm).
Relevant Catheterization Findings
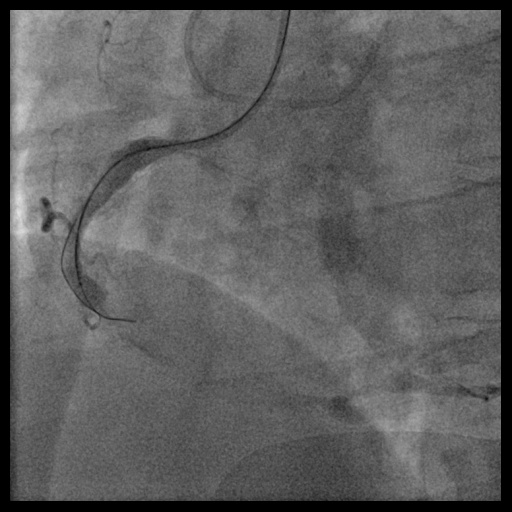
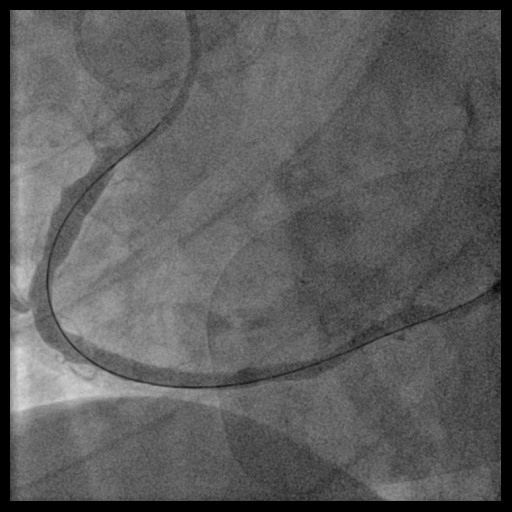
During this emergency catheterization, the right radial artery was accessed using a 20-gauge needle. A 6 Fr in 5 Glidesheath Slender® (Terumo Corp., Tokyo, Japan) was inserted. Coronary angiography was performed using Terumo 5 Fr Judkins catheters, revealing in-stent total occlusion of the RCA and patent left coronary artery (LCA).


Interventional Management
Procedural Step
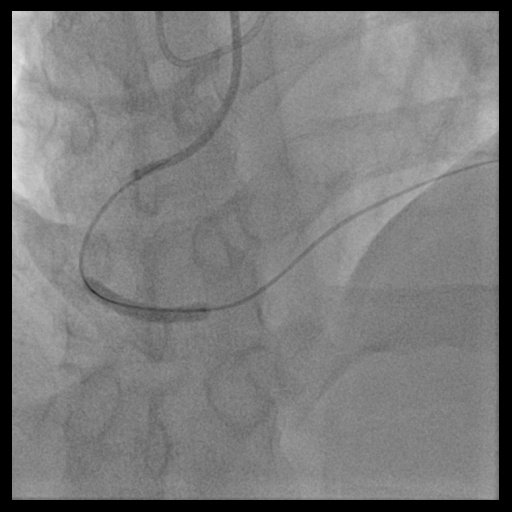
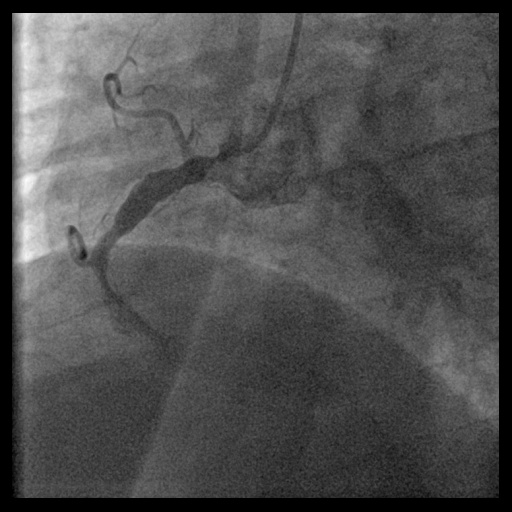
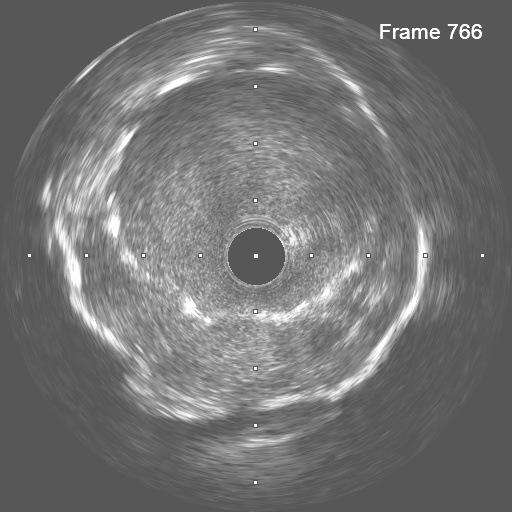
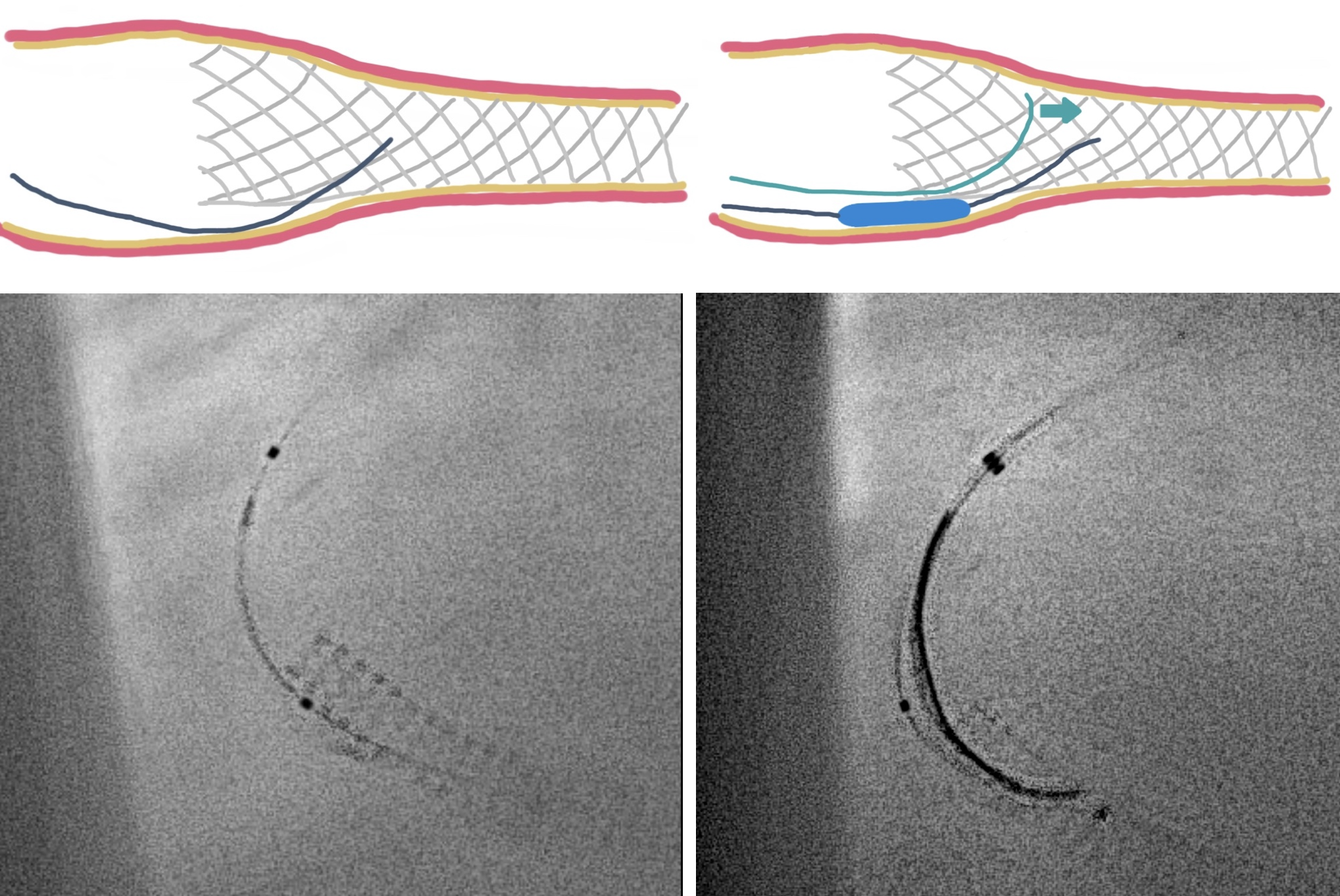
In anticipation of a high thrombus burden, intracoronary Tirofiban was given to mitigate thrombotic risks. The Terumo 6 Fr in 5 Glidesheath Slender was exchanged for a 7 Fr in 6 Glidesheath Slender to accommodate larger catheters while preserving radial artery access. Using a 7 Fr SAL 1.0 guiding catheter (Medtronic, USA), the Fielder FC 0.014” × 180 cm wire (ASAHI Intecc, Japan) was advanced to the distal RCA. Despite GuideLiner (Teleflex, USA) support, the Terumo Eliminate aspiration catheter could not advance beyond the mid-RCA. StentBoost imaging revealed the wire had wound along the aneurysmal vessel wall and passing through a previous stent’s strut. Attempts to reshape the wire tip for re-entry into the stent center were unsuccessful. Although stent crushing was considered, navigating the wire through the stent without damage was prioritized. An Euphora balloon (2.0 × 20 mm) was inflated at 2 atm to seal the gap between the stent and vessel wall, enabling the passage of a Runthrough NS Floppy wire into the distal RCA. IVUS confirmed the wire’s position within the stent, which remained intact. The wire was exchanged for an ASAHI Sion Blue Extra-support wire with a Caravel microcatheter. Thrombus aspiration was completed using the Eliminate catheter. Post-dilatation was performed with a Conqueror NC balloon (4.00 × 20 mm, APT Medical), followed by NC Emerge and Accuforce balloons (4.5-6.0 mm). IVUS confirmed excellent stent apposition, and TIMI 3 flow was achieved.

Case Summary
This case highlights the challenges of managing stents in STEMI patients with aneurysmal vessels. In such patients, vessel size is often underestimated during urgent procedures, leading to stent malapposition and an increased risk of thrombosis. IVUS or OCT is crucial for accurate vessel sizing and ensuring proper stent expansion. The gap between the stent and the vessel wall often causes the guidewire to preferentially pass through the aneurysmal vessel along the greater curve, rather than properly navigating through the stent. Finally, sealing these gaps with a small balloon facilitates guidewire passage and improves outcomes.