
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-015
Large Thrombus Burden Management
By Sheng-Fu Liu, Hsien-Li Kao
Presenter
Sheng-Fu Liu
Authors
Sheng-Fu Liu1, Hsien-Li Kao1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-015
Coronary - ACS/AMI
Large Thrombus Burden Management
Sheng-Fu Liu1, Hsien-Li Kao1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
57 year old gentleman was a case of active smoker and chronic obstructive pulmonary disease. He presented acute 57chest pain at night and visited emergency department for help. Initial vital signs showed BT 34.9 celsius degree, HR 57 beats/min, RR 20/min, BP 84/69mmHg, SpO2 98%.
PE revealed compression chest pain with diaphoresis and basal rales.
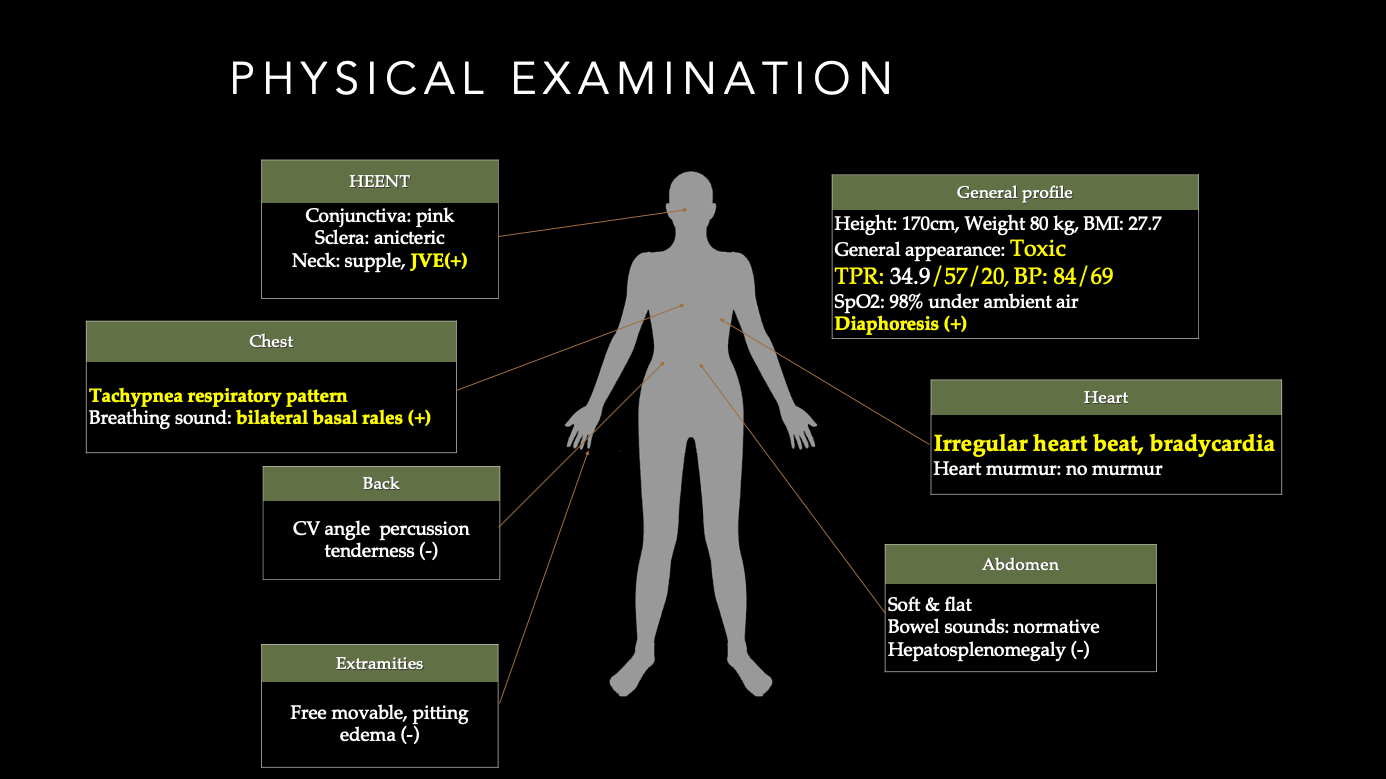
PE revealed compression chest pain with diaphoresis and basal rales.
Relevant Test Results Prior to Catheterization
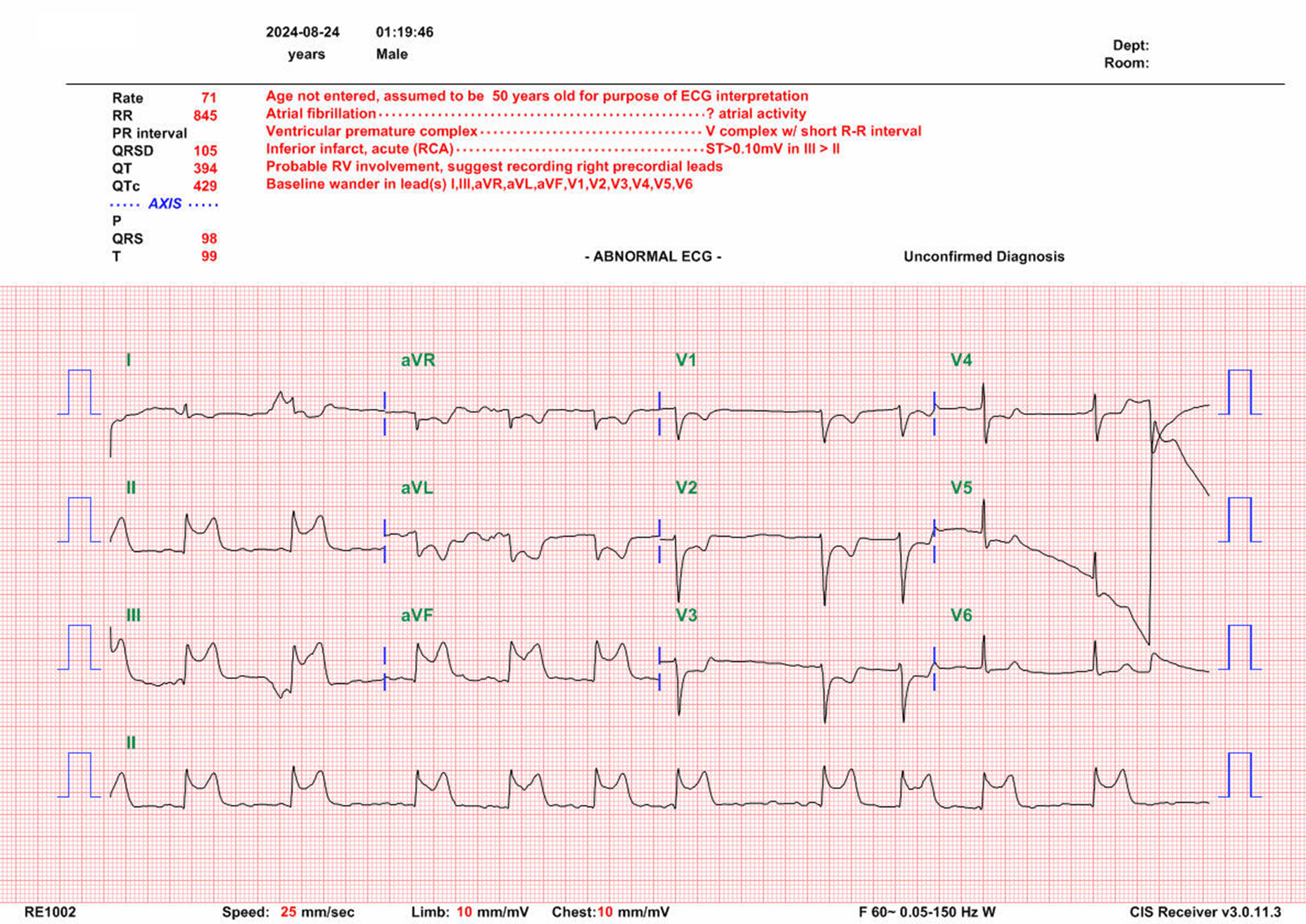
Chest X ray: Kerley'A line (+), Kerley B's line (+), Cephalization (+), thickening interlobar fisures...etc. All features indicated pulmonary edemaEKG: Complete atrioventricular block

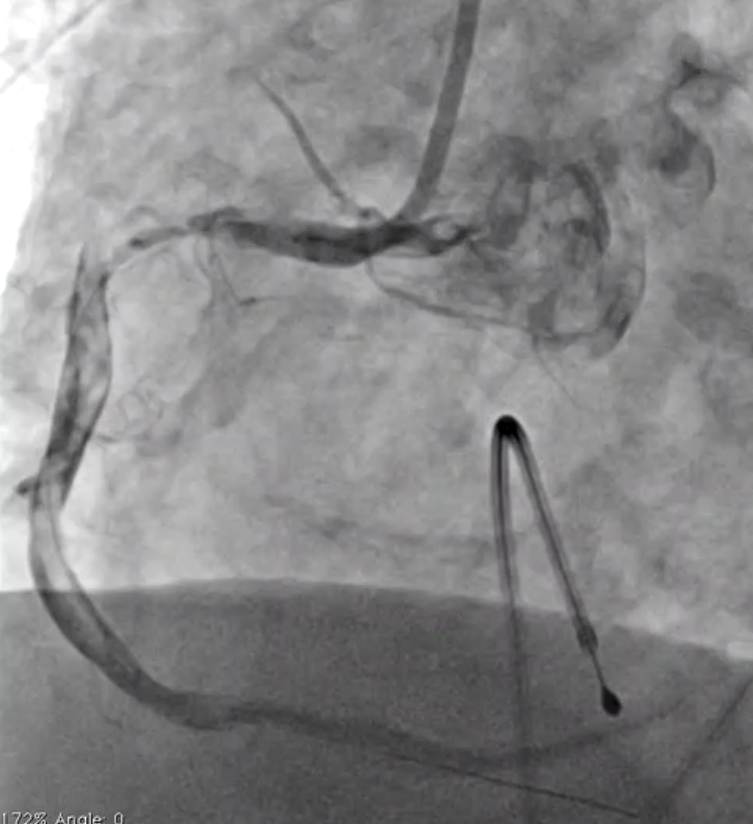
Relevant Catheterization Findings
CAG:LM: patentLAD: non-significant stenosis, milking in dLAD, collateral to RCALCX: non-significant stenosisRCA: 80% stenosis in pRCA with large thrombus burden

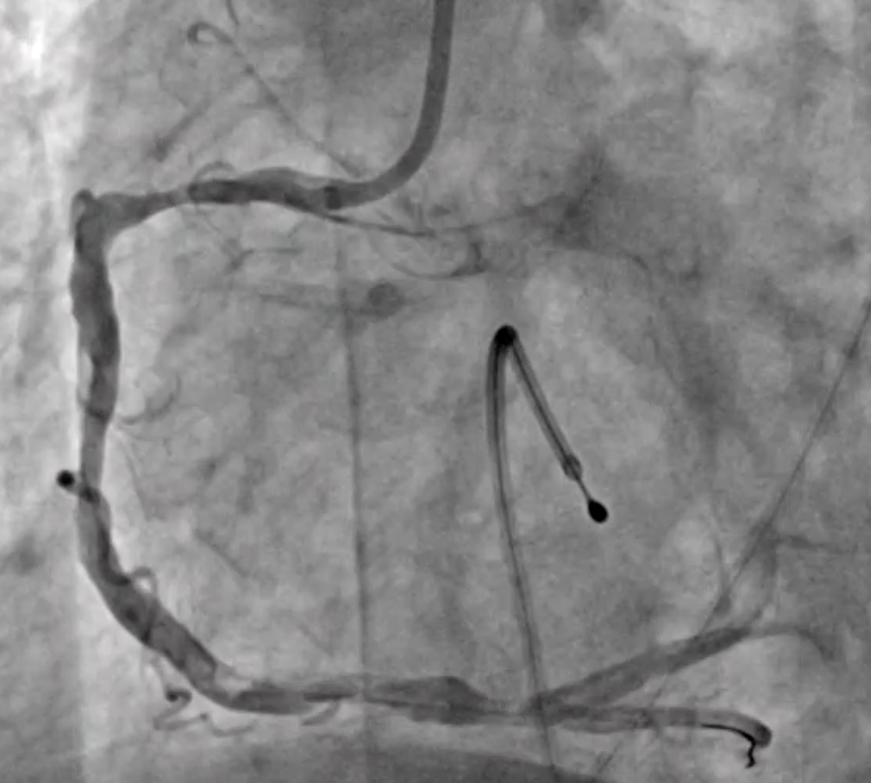
Interventional Management
Procedural Step
1. do RFA and RFV puncture and set TPM to RV apex2. engage to RCA with GC 7F JR43. wiring to dRCA with Sion but failed and rewiring with Fielder FC successfully4. perform thrombosuction with 7Fr MERIT aspiration catheter and red thrombi was aspirated5. much thrombi is noted with hypotension6. give Levophed IF and Aggrastat 850mcg ic7. perform thrombosuction with 7Fr MERIT aspiration catheter and red thrombi was aspirated8. persisted hypotension9. give Gipamin IF10. perform thrombosuction with 7Fr MERIT aspiration catheter and no red thrombi aspirated due to large thrombi. There is still much thrombi at mRCA and dRCA.11. POBA to pRCA with BC 3.0, c/w no reflow in dRCA12. perform thrombosuction with 7Fr MERIT aspiration catheter and red thrombi was aspirated. The flow was recoveried.13. give Urokinase 60000u ic for large burden of thrombi14. perform thrombosuction with 7Fr MERIT aspiration catheter and red thrombi was aspirated15. give Urokinase 60000u ic for large burden of thrombi. The burden of thrombi became smaller and fragmented16. POBA to pRCA with BC 4.017. POBAS to pRCA with BMS "Multi-link 4.0x18mm"18. post dilatation to pRCA stent with stent balloon and NC 4.519. post dilatation to pRCA stent edge with NC 5.020. final result is good, up to TIMI 3 flow21. implant IABP for cardiac support due to cardiogenic shock


Case Summary
Large thrombus burden often cause intervention faliure in STEMI patients. Intracoronary administration of Urokinase during primary PCI effectively improved myocardial perfusion in STEMI with cardiogenic shock pateints.