
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-056
Conquering the Tough Calcium With IVUS Guidance and Rota-Cut
By Animesh Agarwal
Presenter
Animesh Agarwal
Authors
Animesh Agarwal1
Affiliation
Jindal Institute of Medical Sciences, India1,
View Study Report
TCTAP C-056
Coronary - Complex PCI - Calcified Lesion
Conquering the Tough Calcium With IVUS Guidance and Rota-Cut
Animesh Agarwal1
Jindal Institute of Medical Sciences, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
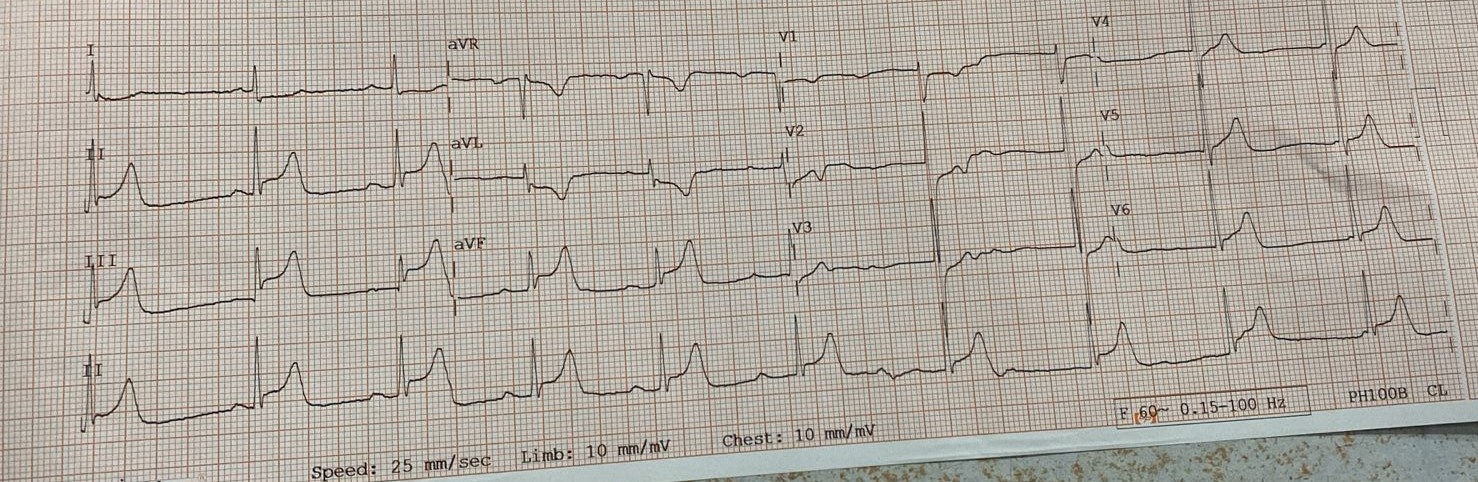
A 63 years old female, presented with the complaint of severe chest pain for one day. She was diabetic, hypertensive, obese. Her ECG showed Inferior wall MI. On examination her blood pressure was 130/90 mmHg, Heart rate was 89 beats per minute
Relevant Test Results Prior to Catheterization
Her Echocardiography showed a LVEF- 30%. Her Hemoglobin was 10.1 g/dl, Serum Creatinine level was 1.1 mg/dl.
Relevant Catheterization Findings
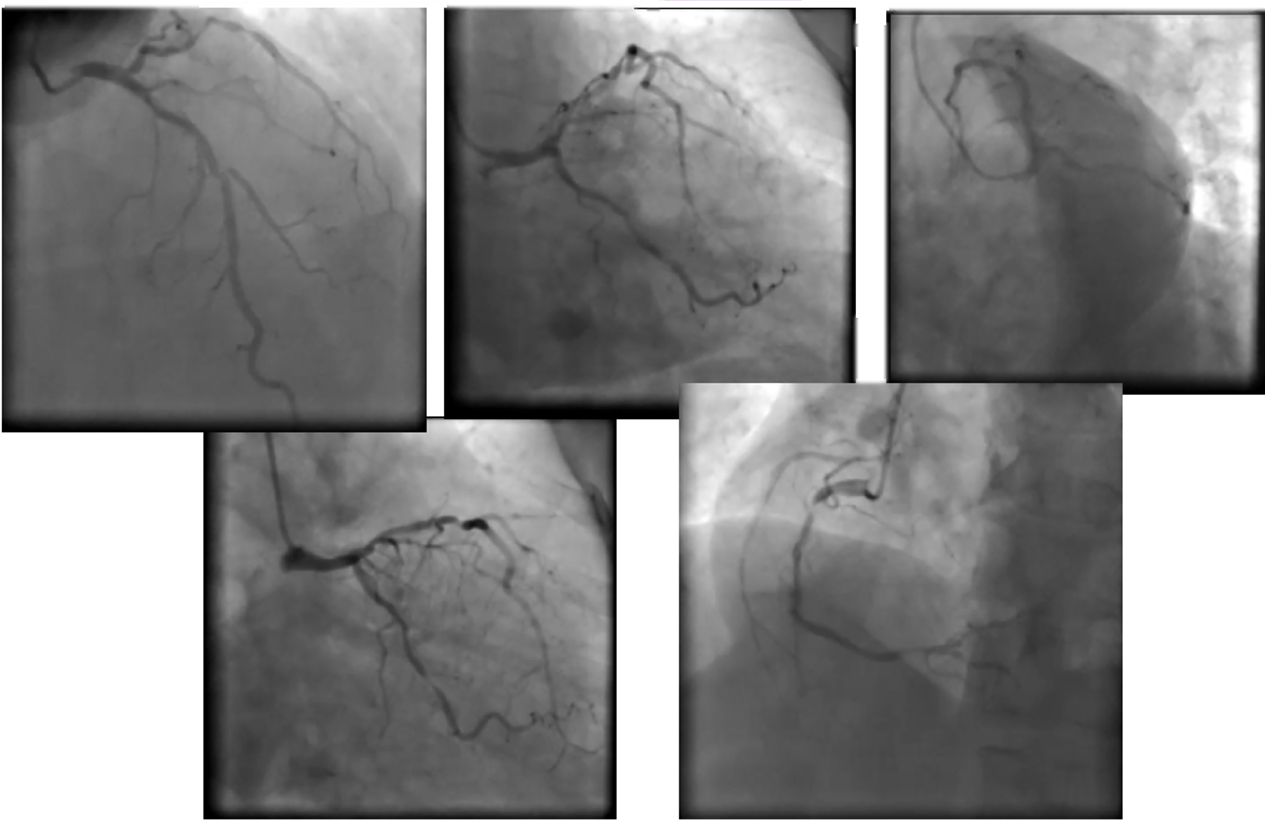
Coronary Angiography showed calcified lesion in proximal to mid segment of LAD with nearly 80% luminal stenosis. LCX distal was 80-90% stenosis . RCA was dominant and showed 80-90% lesion in the proximal segment of artery.
Interventional Management
Procedural Step
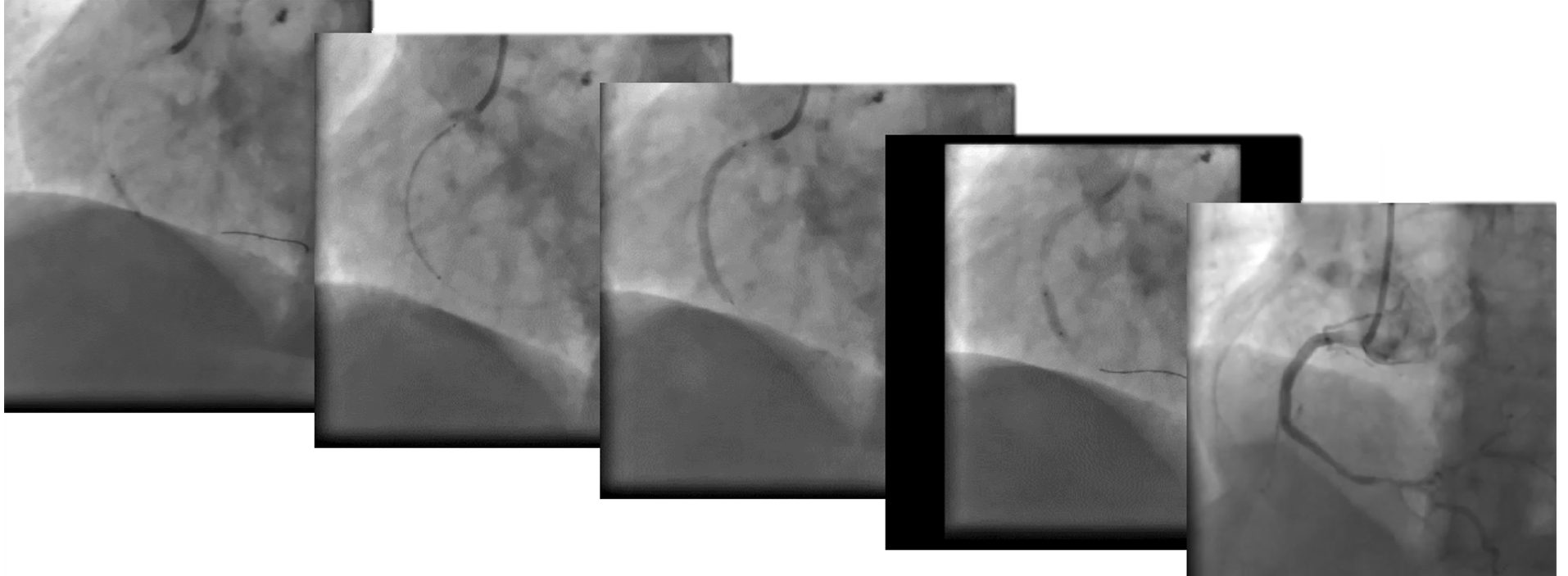
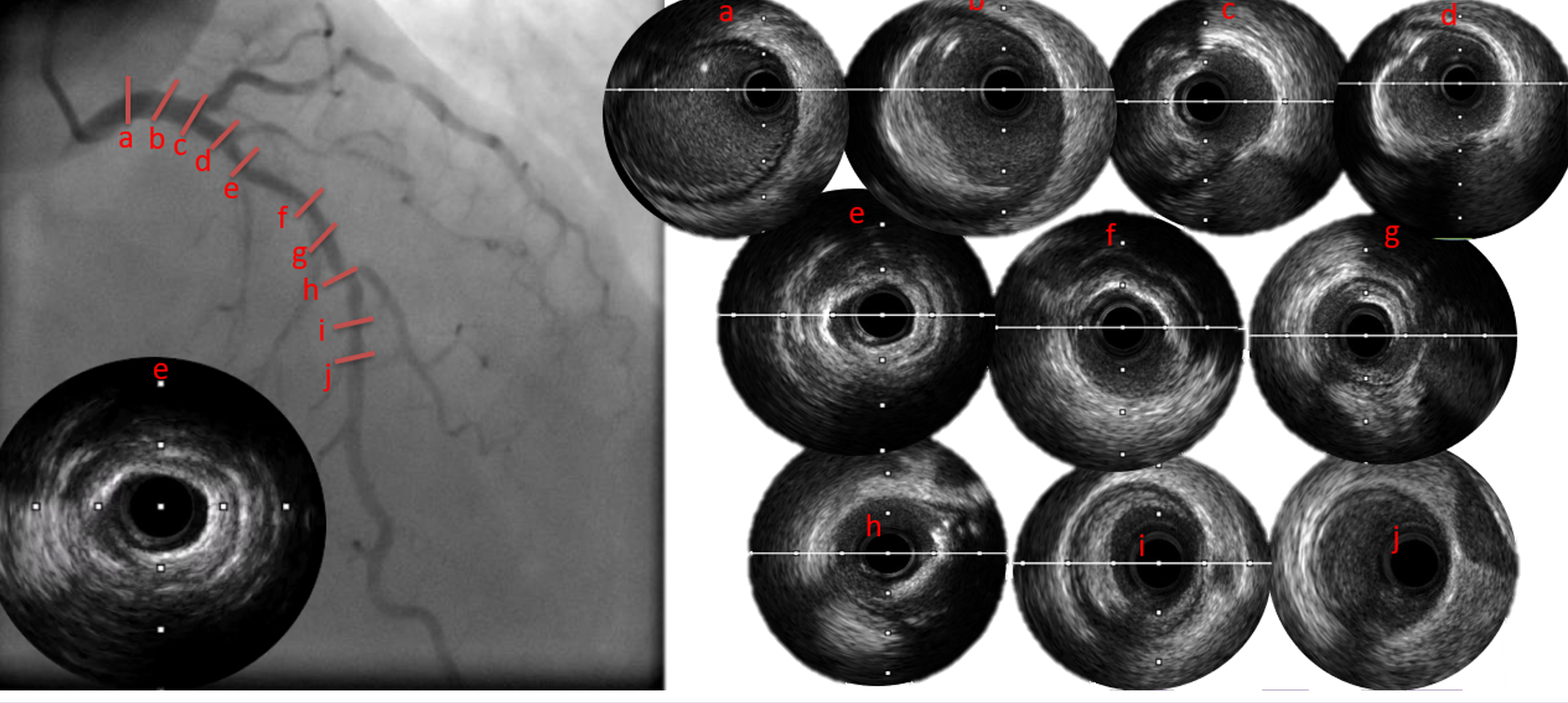
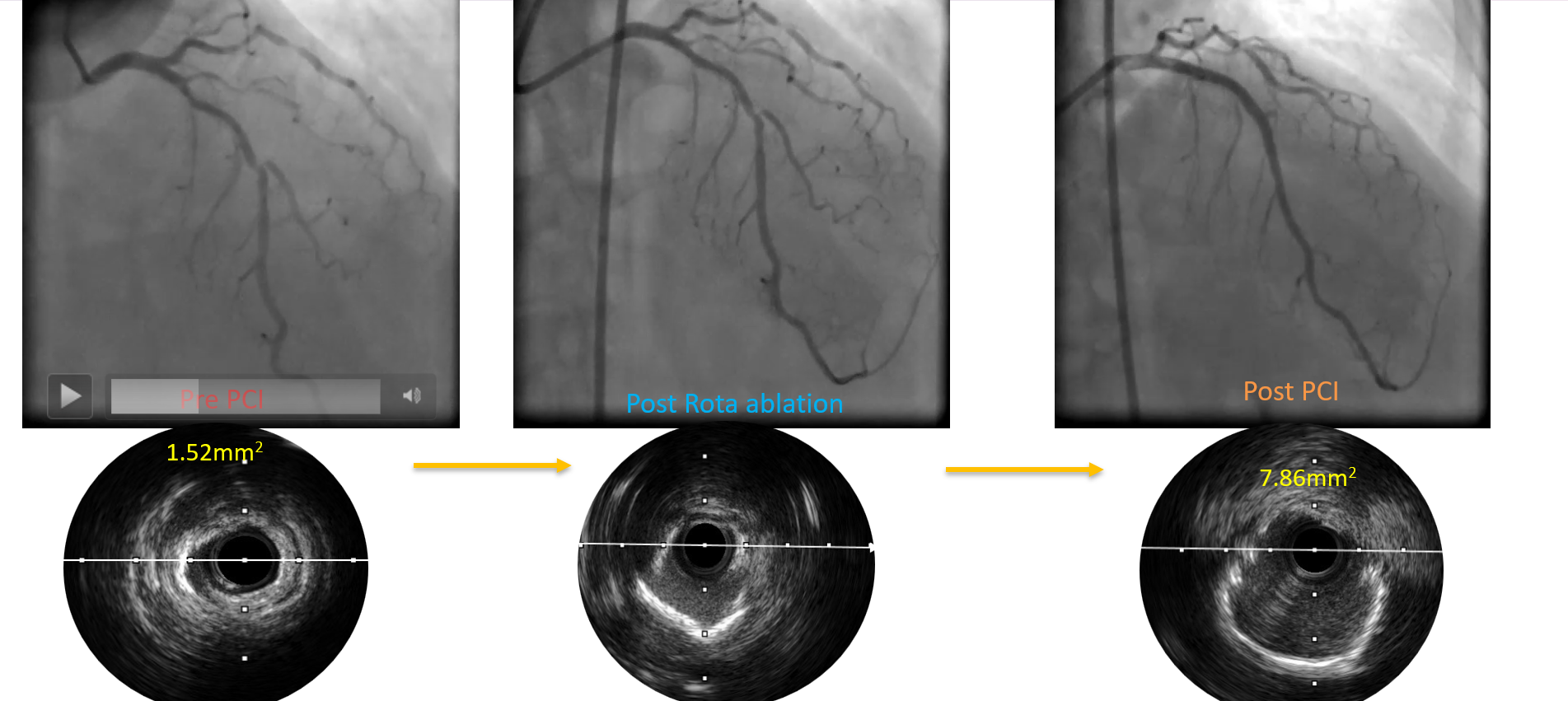
Primary PCI of RCA was performed. IVUS was performed in LAD-LMCA to assess the plaque morphology and right tool for bed preparation. IVUS showed a long calcified lesion in LAD with almost 360 degree arc of calcium in Mid LAD, MLA was 1.52 mm2. So looking at tight calcific lesion in LAD, planned to go with Rotablation in LAD. Lesion was crossed with WH wire and exchanged to Rota wire with the help of micro catheter. Rotablation was done with 1.75 mm burr at the speed of 150000 rpm to 170000 rpm. Total 7 Runs of 15-20 seconds each of Rotablation were done followed by polishing run. Post rotablation pre dilation was done with 2.75 mm x 10 mm NC balloon at 20 atm pressure, but DES was failed to cross the lesion. Then guide extension catheter was used to support the DES crossing, but stent still failed to cross the lesion. After that Cutting Balloon 2.75mm x 10mm size used to prepare lesion. Post bed prepared with cutting balloon, DES 3.00 mm x 48 mm was deployed in LAD with Guide extension support followed by post dilatation. Post IVUS Run confirms the well apposed, fully expended and no complication (dissection/Hematoma) at the edges of the stent
Case Summary
It is a good practice to do coronary imaging in PCI to assess proximal and distal landing zone (Diameter & Length), type of Plaque and disease burden and LMCA.IVUS always help in deciding right approach/tool for bed preparation, right Burr size, right diameter and length of stent, right balloon diameter for post dilatation.Right size and speed of Rota Burr helps in better and easy debulking of calcium.Don’t hesitate in using Guide Extension catheter while using DES/ancillary device in challenging coronaries.ROTA with Cutting Balloon (ROTA-CUT) gives better result with greater lumen and good expansion of DES (MSA).