
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-027
Survival Against All Odds: Eleven Arrests, Double Culprit STEMI, and Multi-Organ Failure
By Marshell Luntungan, Dewi Utari Djafar
Presenter
Marshell Luntungan
Authors
Marshell Luntungan1, Dewi Utari Djafar1
Affiliation
Prof. Dr. R.D. Kandou General Hospital, Indonesia1,
View Study Report
TCTAP C-027
Coronary - ACS/AMI
Survival Against All Odds: Eleven Arrests, Double Culprit STEMI, and Multi-Organ Failure
Marshell Luntungan1, Dewi Utari Djafar1
Prof. Dr. R.D. Kandou General Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
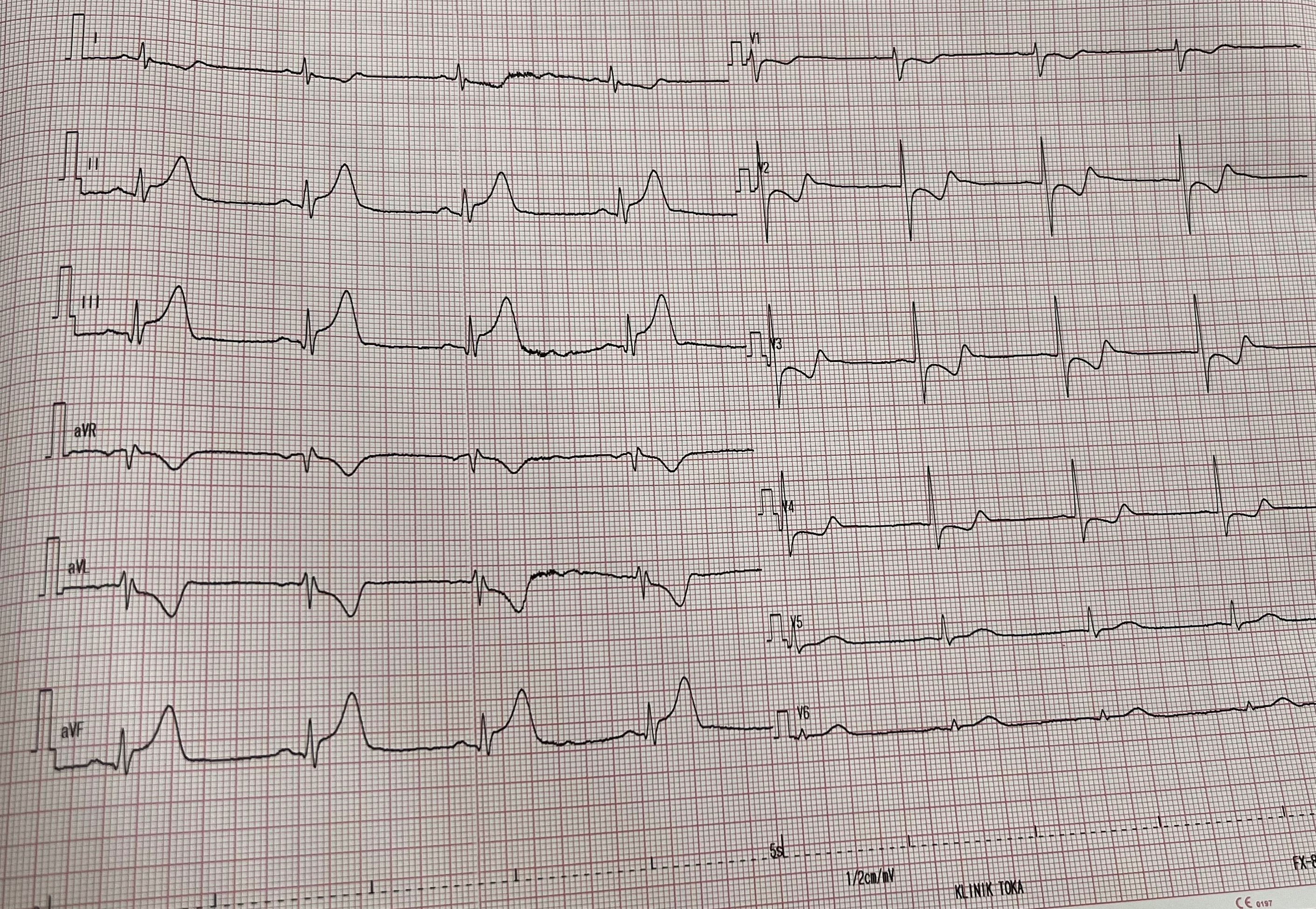
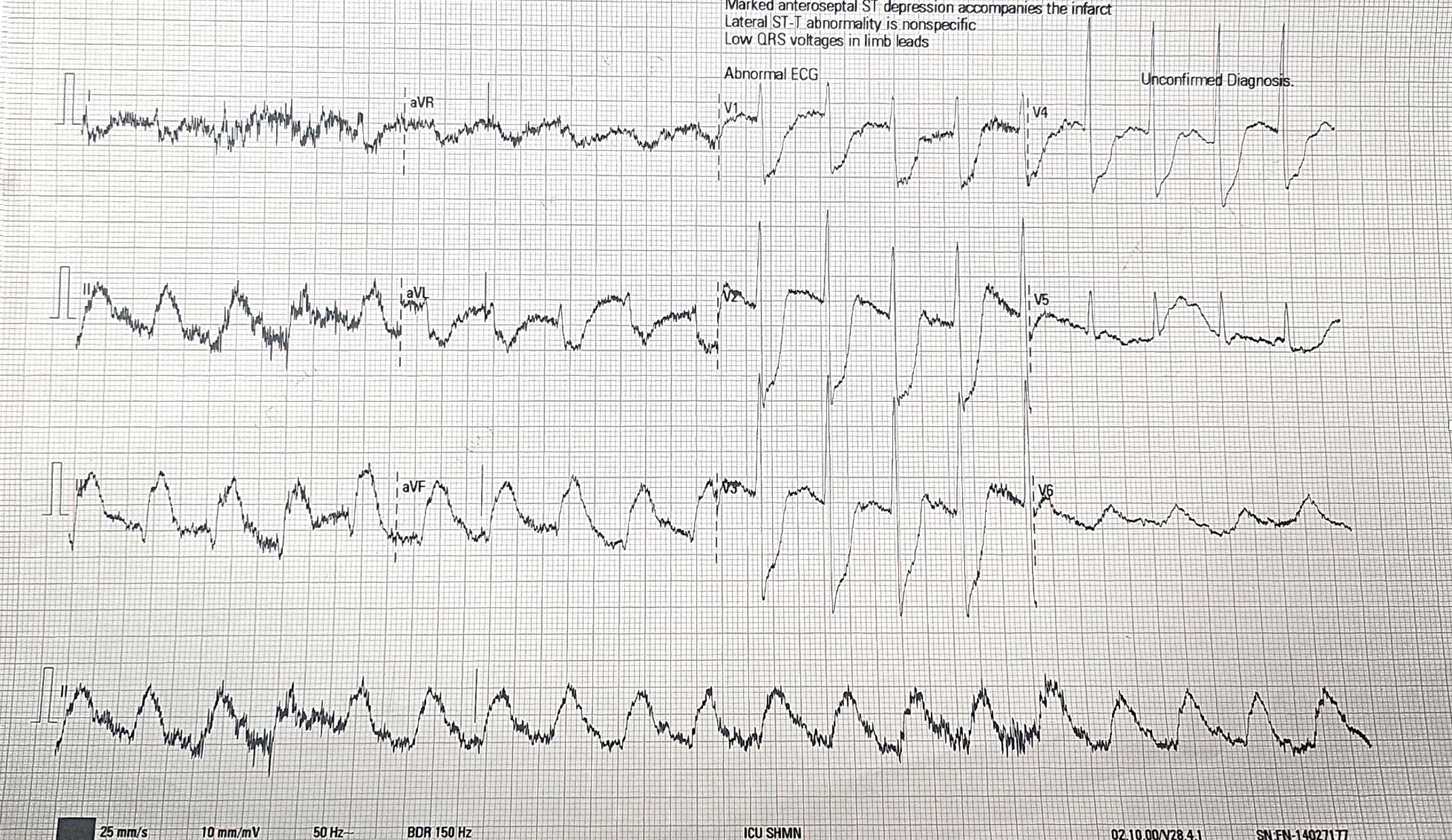
A 34-year-old male was evacuated from a mining site to ED with retrosternal chest pain lasting 3 hours. An ECG confirmed inferior-posterior STEMI. Known risk factors included heavy smoking and alcohol use. Upon transfer from the ambulance, he suffered cardiac arrest. High-quality CPR achieved ROSC. Intubated with a GCS of 3, he presented in cardiogenic shock (BP 80/40).
Relevant Test Results Prior to Catheterization
Due to fluctuating high random blood glucose levels (374-456 mg/dL), primary percutaneous coronary intervention (PPCI) could not be performed within the optimal 120-minute window. Consequently, alteplase was used as a bailout strategy. The patient experienced several additional cardiac arrests and ROSC.Approximately 6 hours later, after achieving target random blood glucose levels, he was urgently transferred to the cath lab for rescue PCI
Relevant Catheterization Findings
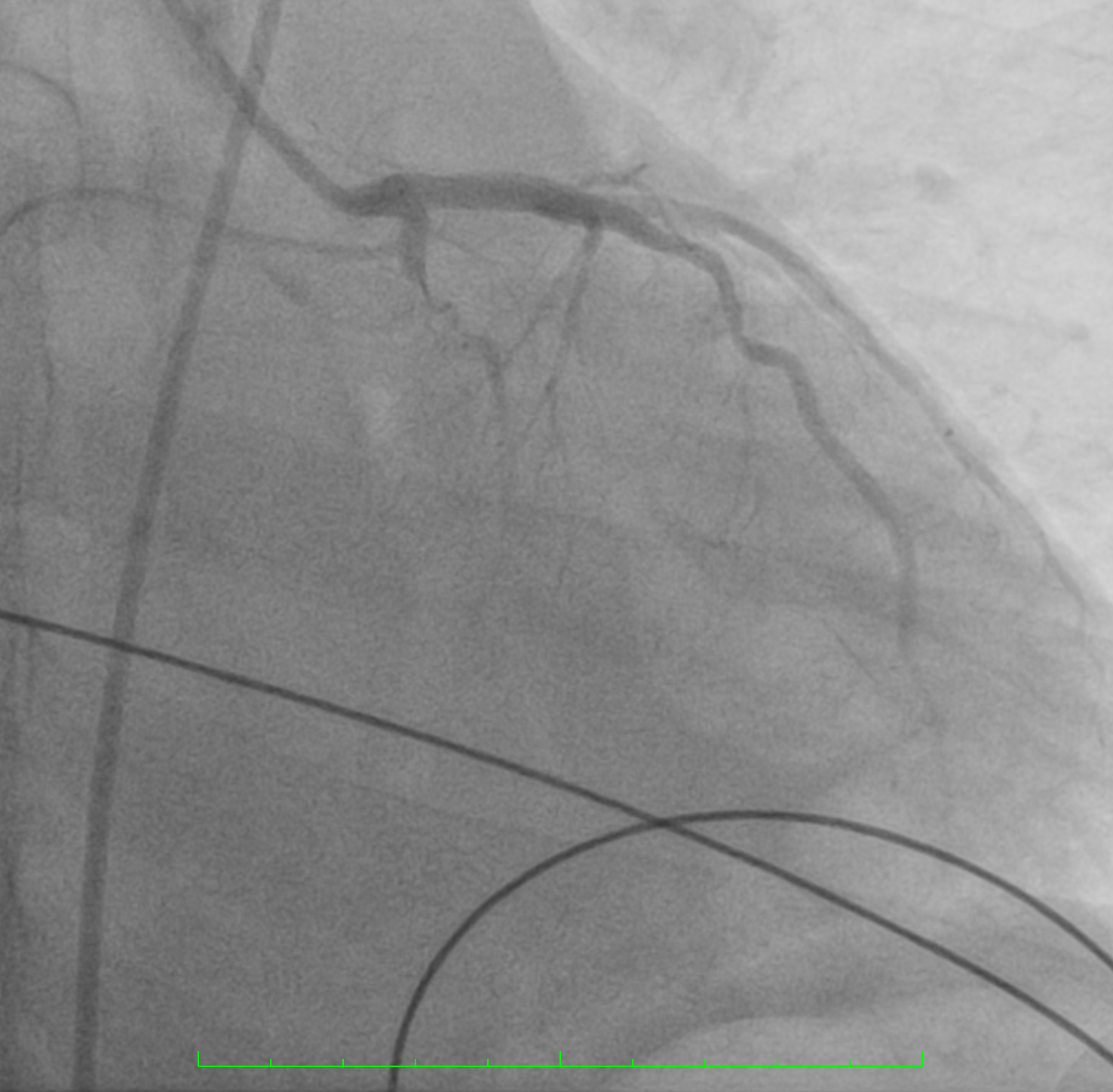
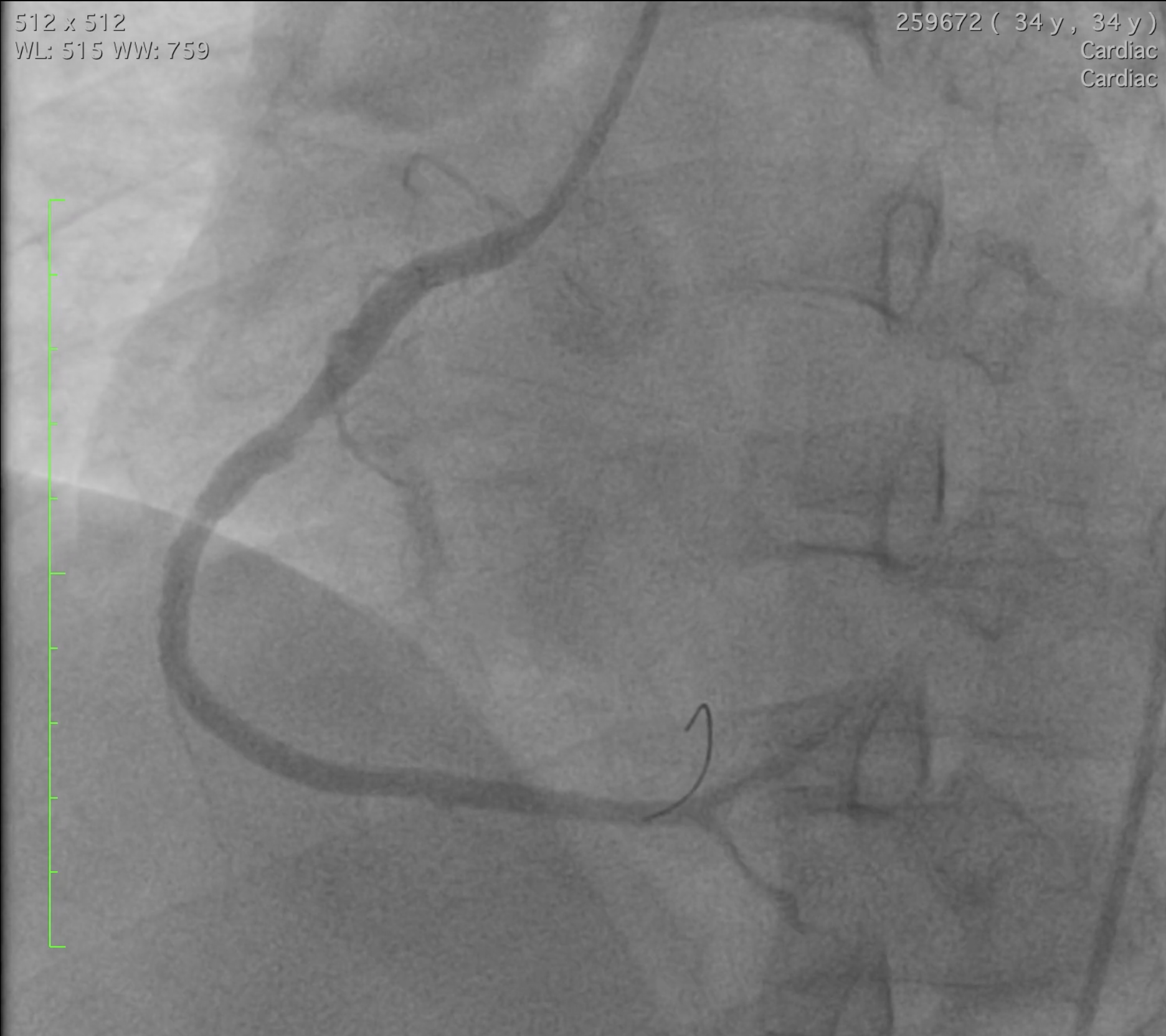
Rescue PCI was successful, with one drug-eluting stent (DES) placed in the posterior left circumflex (pLCX) and another in the posterior right coronary artery (pRCA), both of which were occluded with grade V thrombus

Interventional Management
Procedural Step
LCX:- Femoral Access- GC JL 3.5/6F- Thrombus grade V proximal LCX- Using Intuition wire can penetrate until distal LCX- Predilate with SC baloon Ikazuchi 2.0x20mm showed TIMI 2-3 Flow- Stent with DES Xience Xierra 2.75 x 23mm showed TIMI 3 Flow with no residual thrombus or stenosisRCA:- Femoral Access- Thrombus grade V proximal RCA- GC JR 3.5/6F- Using intuition wire can penetrate until distal RCA- Direct stent with DES Biomatrix Ultra 3.5x36mm showed TIMI 3 Flow with no residual thrombus or stenosis

Case Summary
1. Quick recognition and treatment of STEMI are vital, even in complex cases with rapid deterioration .