
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-224
Recurrent Fresh Left Atrial Appendage Thrombus in Severe Rheumatic Mitral Stenosis: Transitioning Strategy for Optimal Management
By Ingrid Maria Pardede, Sunanto Ng, Jessica Anastasia Setiawan
Presenter
Ingrid Maria Pardede
Authors
Ingrid Maria Pardede1, Sunanto Ng1, Jessica Anastasia Setiawan1
Affiliation
Pelita Harapan University, Indonesia1,
View Study Report
TCTAP C-224
Structural - Surgical Therapy (Structural)
Recurrent Fresh Left Atrial Appendage Thrombus in Severe Rheumatic Mitral Stenosis: Transitioning Strategy for Optimal Management
Ingrid Maria Pardede1, Sunanto Ng1, Jessica Anastasia Setiawan1
Pelita Harapan University, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
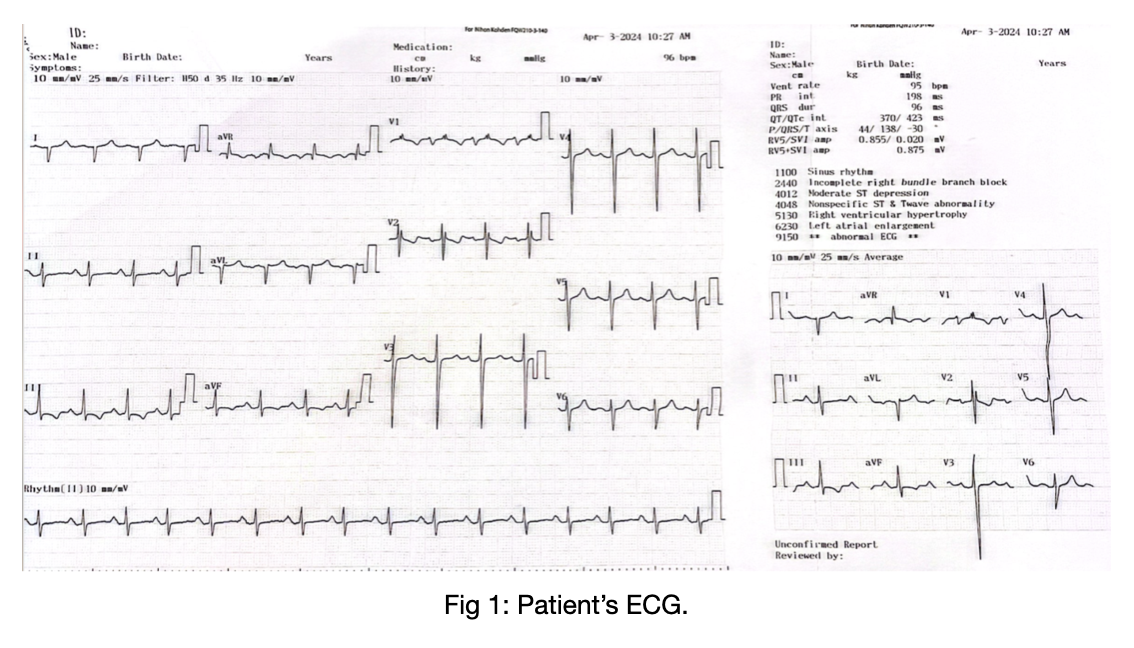
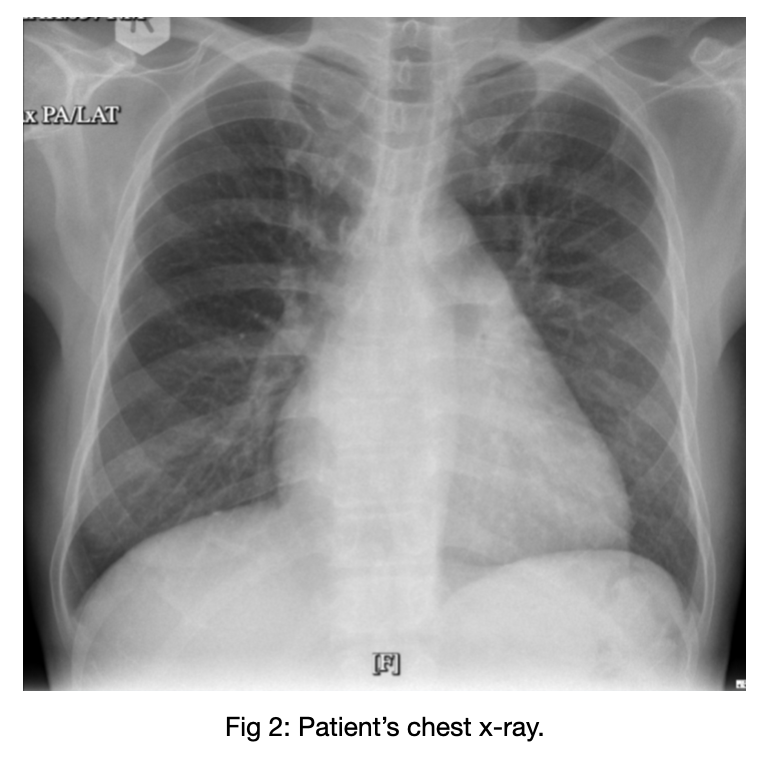
A 57-year-old male working as an aviation mechanic from Qatar came with worsening dyspnea on effort for 3 months with a previous history of uncontrolled DM (HbA1C 7.9 %). Physical examination was significant for diastolic murmur with opening snap, best heard at apex. ECG showed sinus rhythm, biatrial enlargement, RAD, RVH, incomplete RBBB. Chest x-ray revealed cardiomegaly with pulmonary artery dilatation and left atrial enlargement.
Relevant Test Results Prior to Catheterization
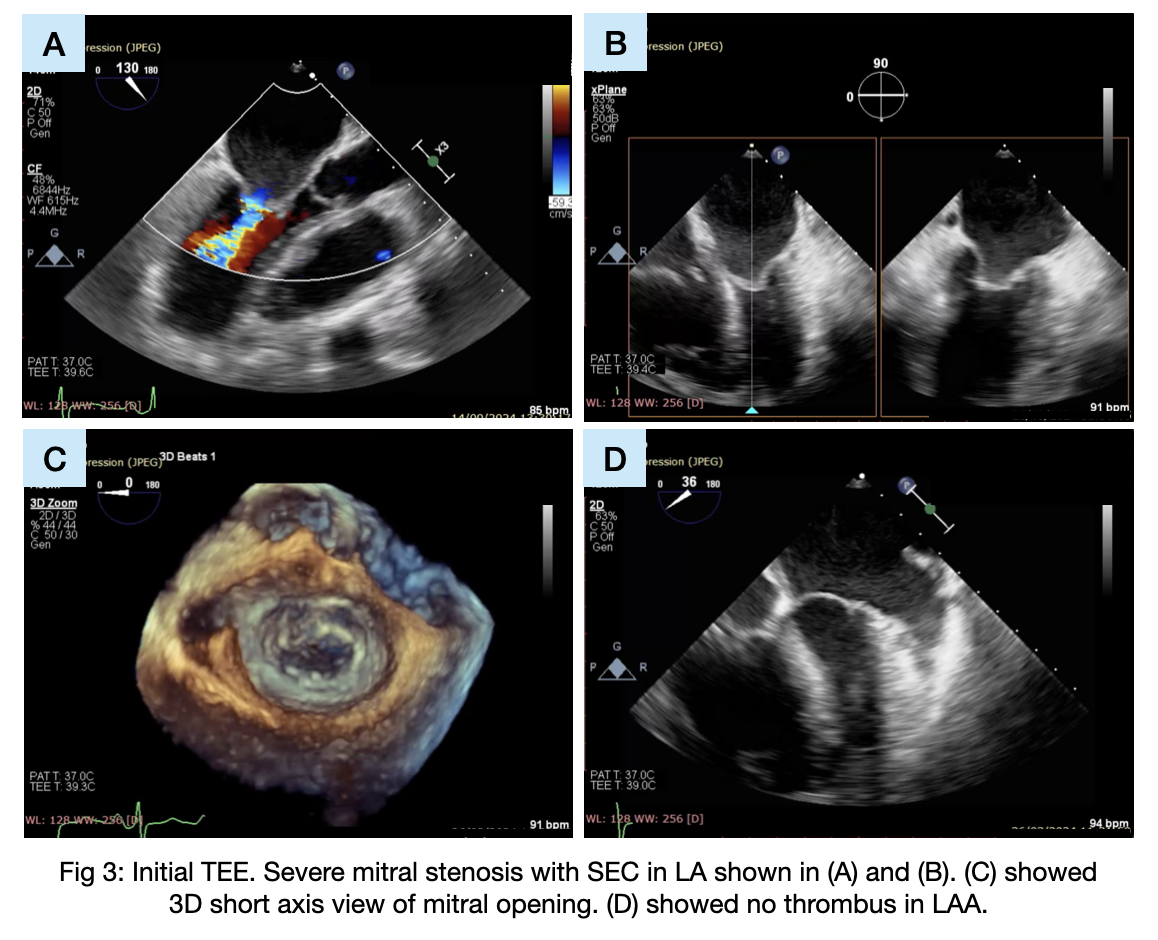
TEE showed severe mitral stenosis with rheumatic mitral morphology, MVA 0.6 cm2, mean/peak MVG 8/12 mmHg, Wilkins score of 8 favorable for BMV and pulmonary hypertension with secondary tricuspid regurgitation. In preparation for BMV, he was advised to consume warfarin for 3 months and achieved INR 3.5.
Relevant Catheterization Findings
Interventional Management
Procedural Step
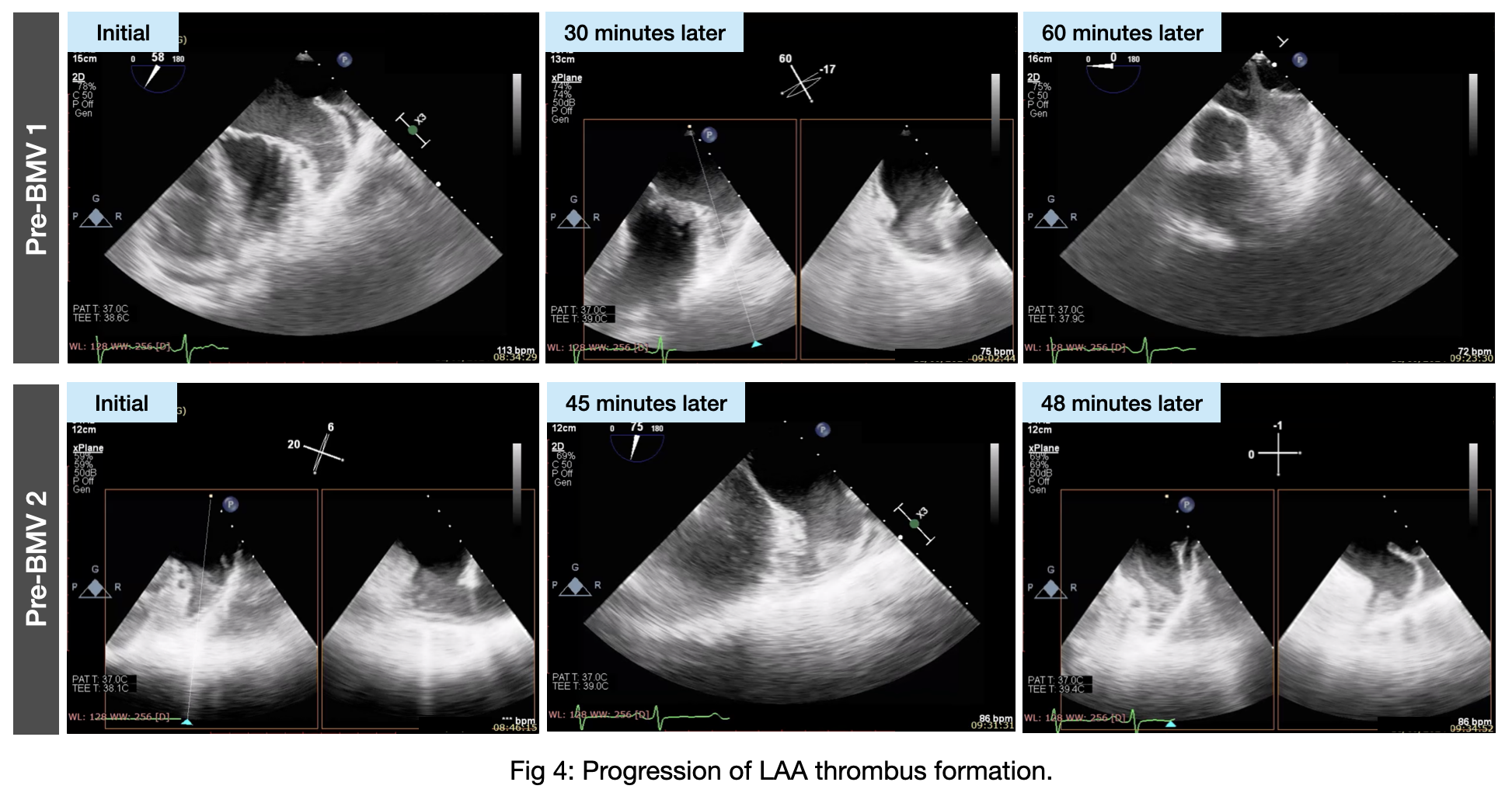
Right before BMV, his preprocedural TEE showed thrombus formation in LAA and the procedure was postponed. After 5 days with enoxaparin, follow-up TEE showed dissolved thrombus. Hence, another BMV was rescheduled. The second pre-BMV TEE showed another fresh thrombus formation in LAA, thus BMV was again canceled. Coronary angiography showed significant stenosis in p-mLAD and dRCA. Therefore, MVR and CABG were planned instead. Open heart surgery was done on-pump. CABG X2 was done (LIMA-LAD and SVG-distal D1). MITRIS RESILIA 25# (Edwards Lifesciences, USA) bioprosthetic valve was used for MVR. Tricuspid valve was repaired by bicuspidization (Kay annuloplasty). LAA plication was also done to prevent another thrombus formation. Post-operative valve evaluation showed good position and function with MVA 4.4 cm2, MVG 3 mmHg. One month later, ECG showed persistent atrial fibrillation despite receiving amiodarone. No cardiac thrombus seen in TEE and the patient received electric cardioversion of 200 J. Rhythm converted back to sinus. Follow-up in 2 weeks showed no recurrent atrial fibrillation.
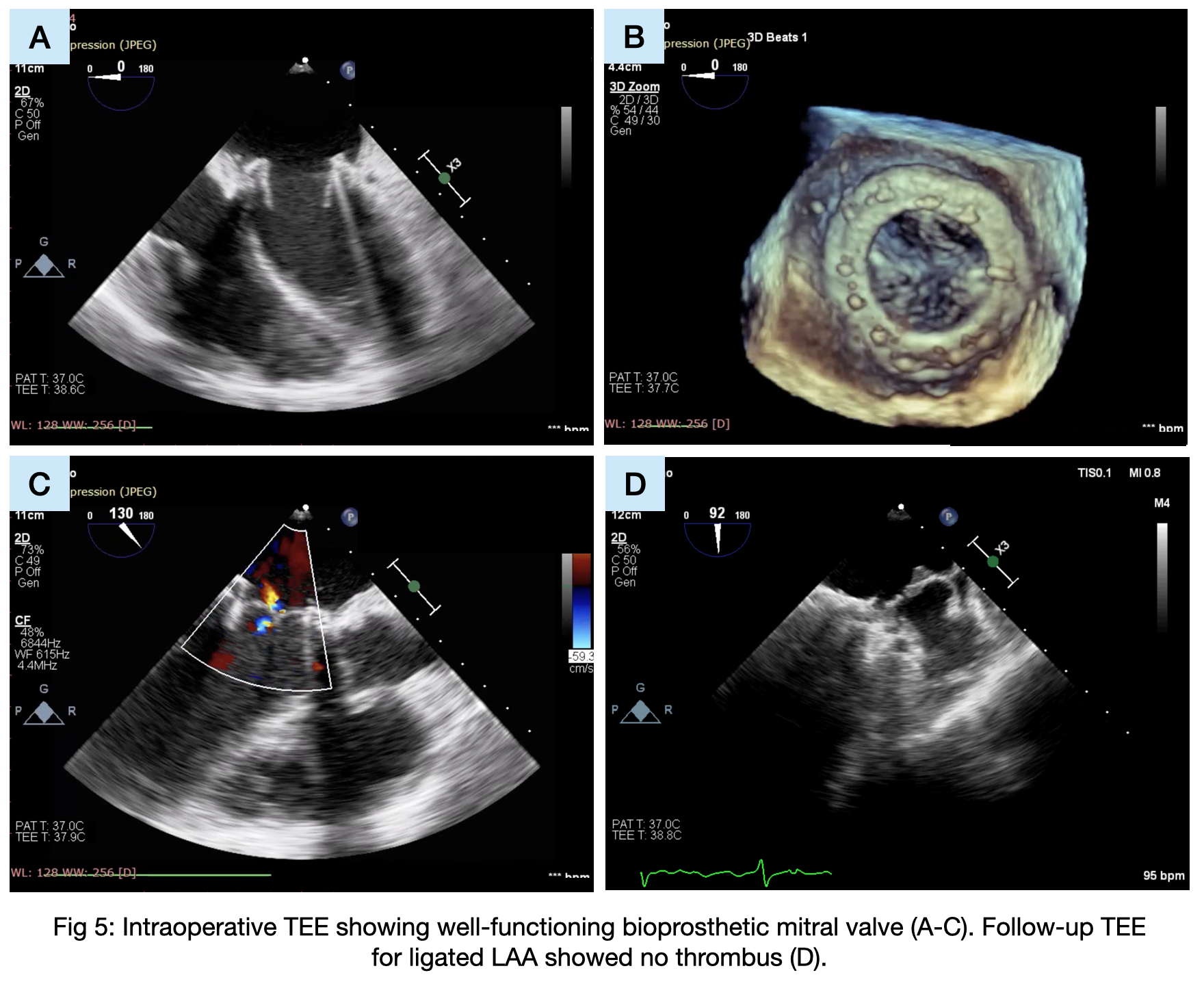

Case Summary
The initial plan for BMV was deferred twice due to thrombus recurrence, prompting a change in strategy to MVR with bioprosthetic valve and CABG for coexisting coronary artery disease. LAA plication effectively prevented further thrombus formation. Postoperative persistent atrial fibrillation necessitated rhythm control with electric cardioversion to restore sinus rhythm. Follow-up confirmed successful outcomes and maintained sinus rhythm, underscoring the importance of a multidisciplinary approach in complex cardiac cases.