
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-235
Unraveling the Unexpected: Stent Dislodgement in Subclavian Artery Angioplasty
By Ru-Yin Hsu
Presenter
Ru-Yin Hsu
Authors
Ru-Yin Hsu1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-235
Endovascular - Other Endovascular Intervention
Unraveling the Unexpected: Stent Dislodgement in Subclavian Artery Angioplasty
Ru-Yin Hsu1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 73-year-old woman with a medical history of type 2 diabetes mellitus, hyperlipidemia, and hypertension has been experiencing dizziness for the past three years. Notably, she has not reported any nausea, vomiting, or episodes of syncope. Her blood pressure readings revealed a disparity of up to 40 mmHg between her two arms.
Relevant Test Results Prior to Catheterization
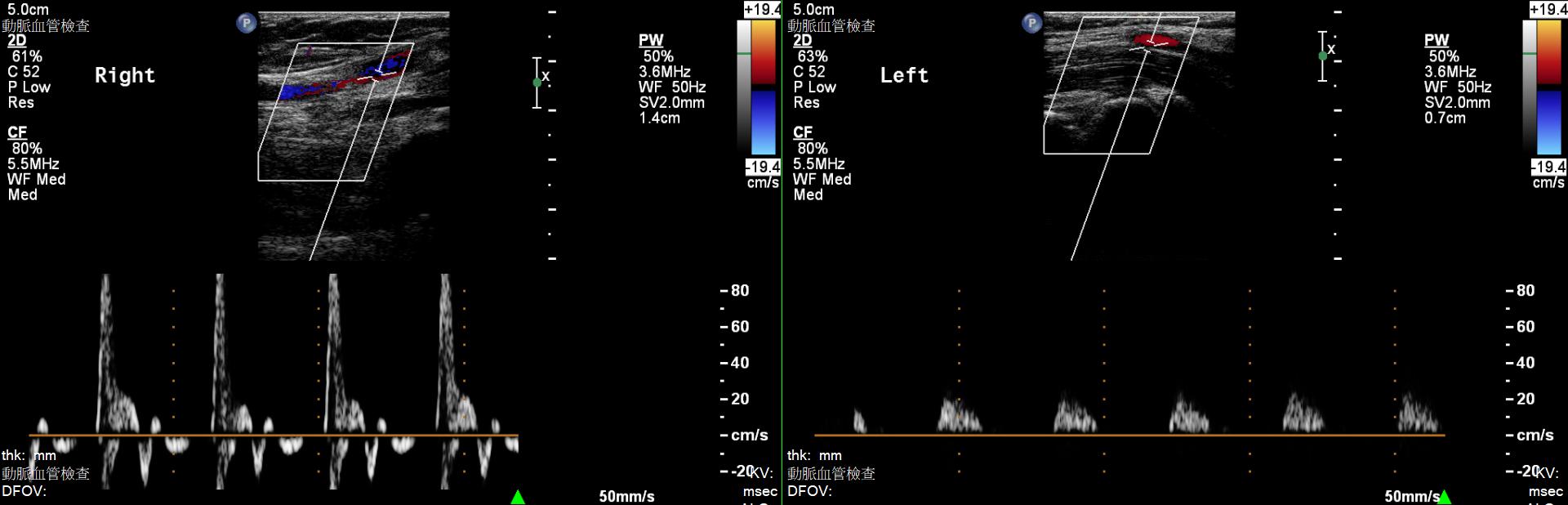
In light of these findings, a vascular duplex sonography was conducted, which indicated a significant compromise in blood flow within the left brachial artery, suggesting the presence of substantial stenosis in the left subclavian artery. A CT scan indicated a prominent calcification with severe stenosis at left subclavian artery orifice.


Relevant Catheterization Findings
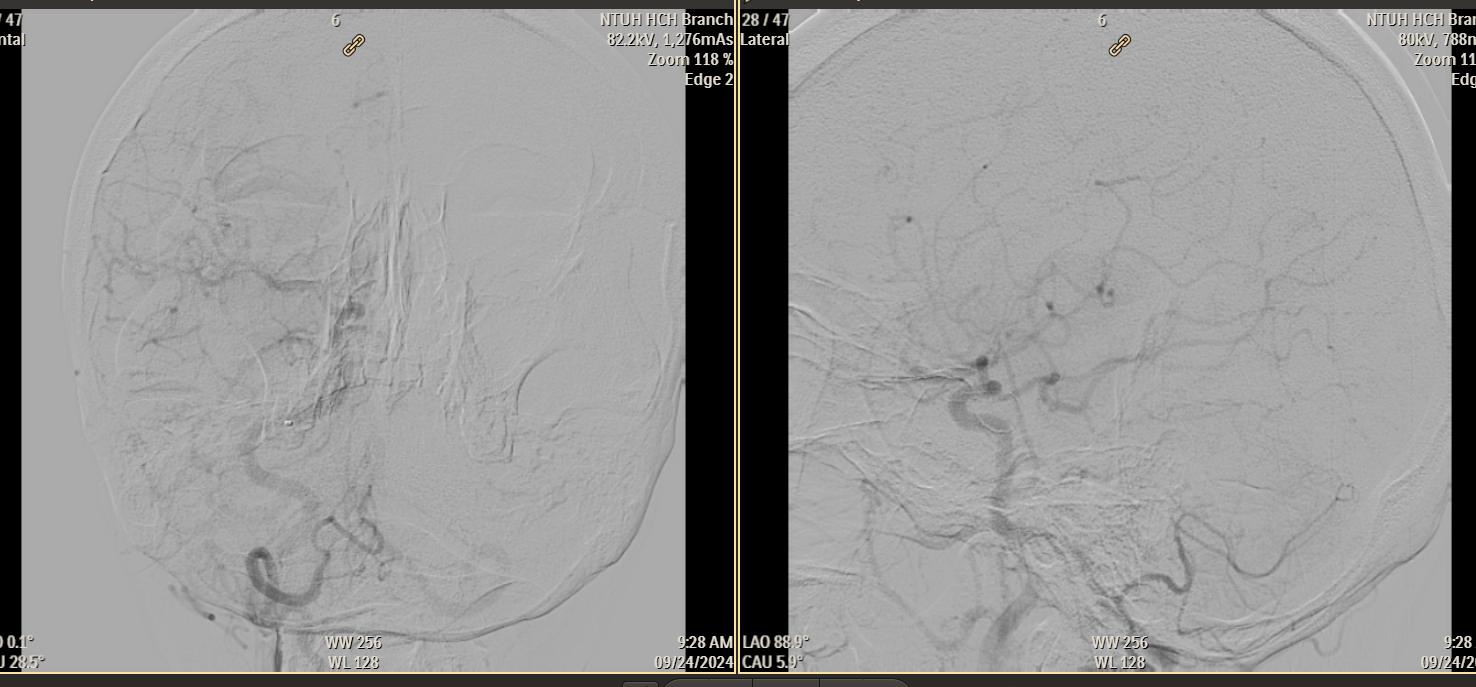
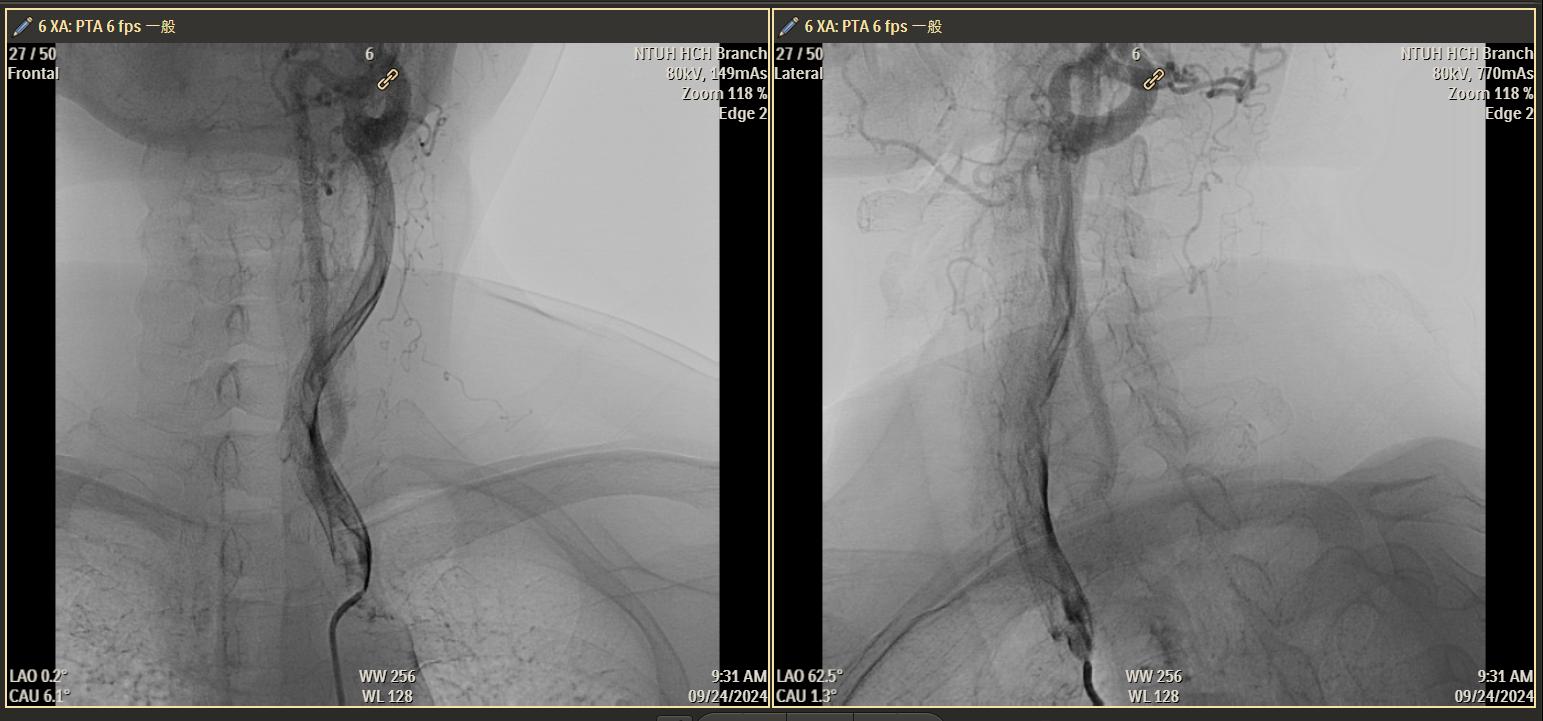
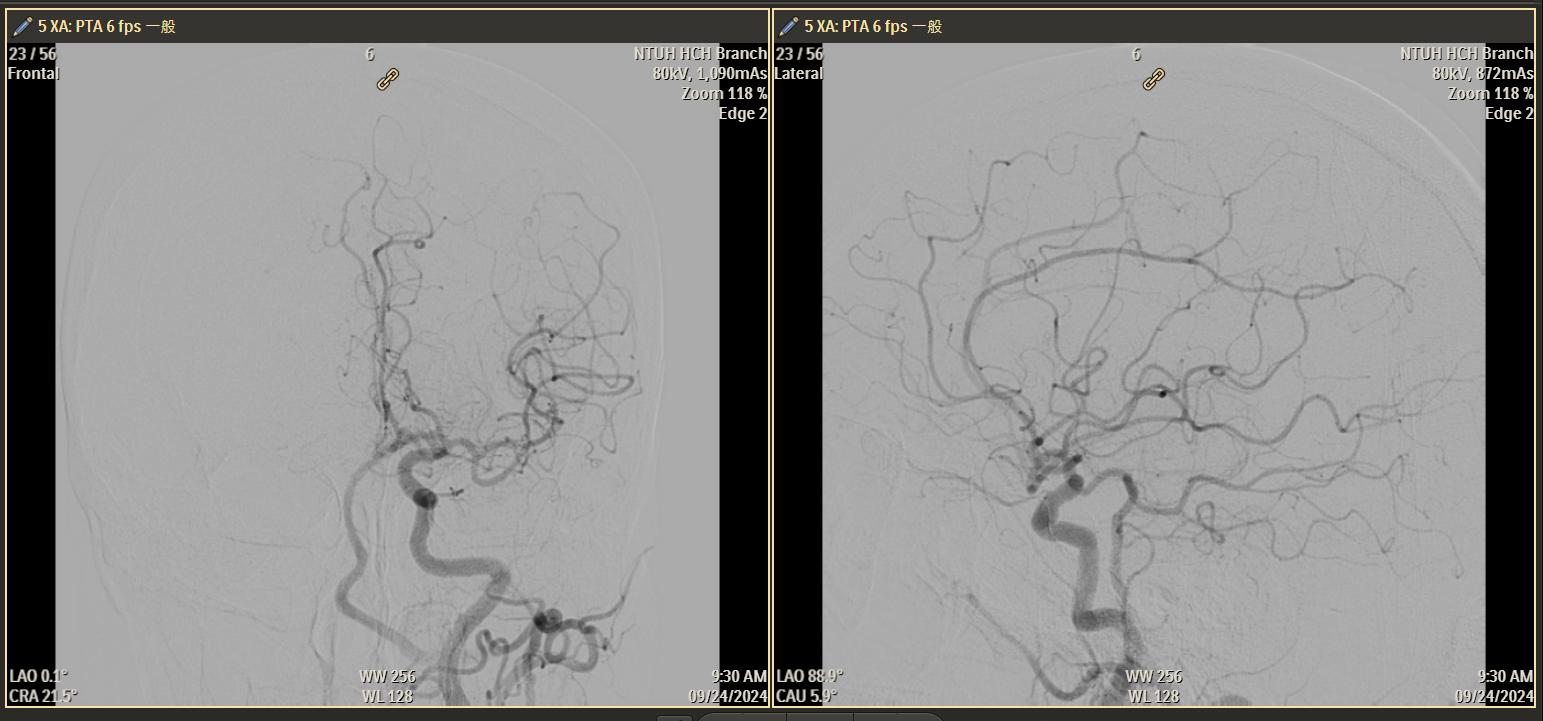
The carotid angiography confirmed the presence of left subclavian steal with retrograde flow in the left vertebral artery and complete occlusion of the left subclavian artery orifice. No antegrade flow from the vertebral artery contributed to the intracranial posterior circulation. Retrograde collaterals from the left middle cerebral artery reconstituted flow in the left subclavian artery.
 subclavian steal.jpg
subclavian steal.jpg
subclavian steal intracranial.jpg
Interventional Management
Procedural Step
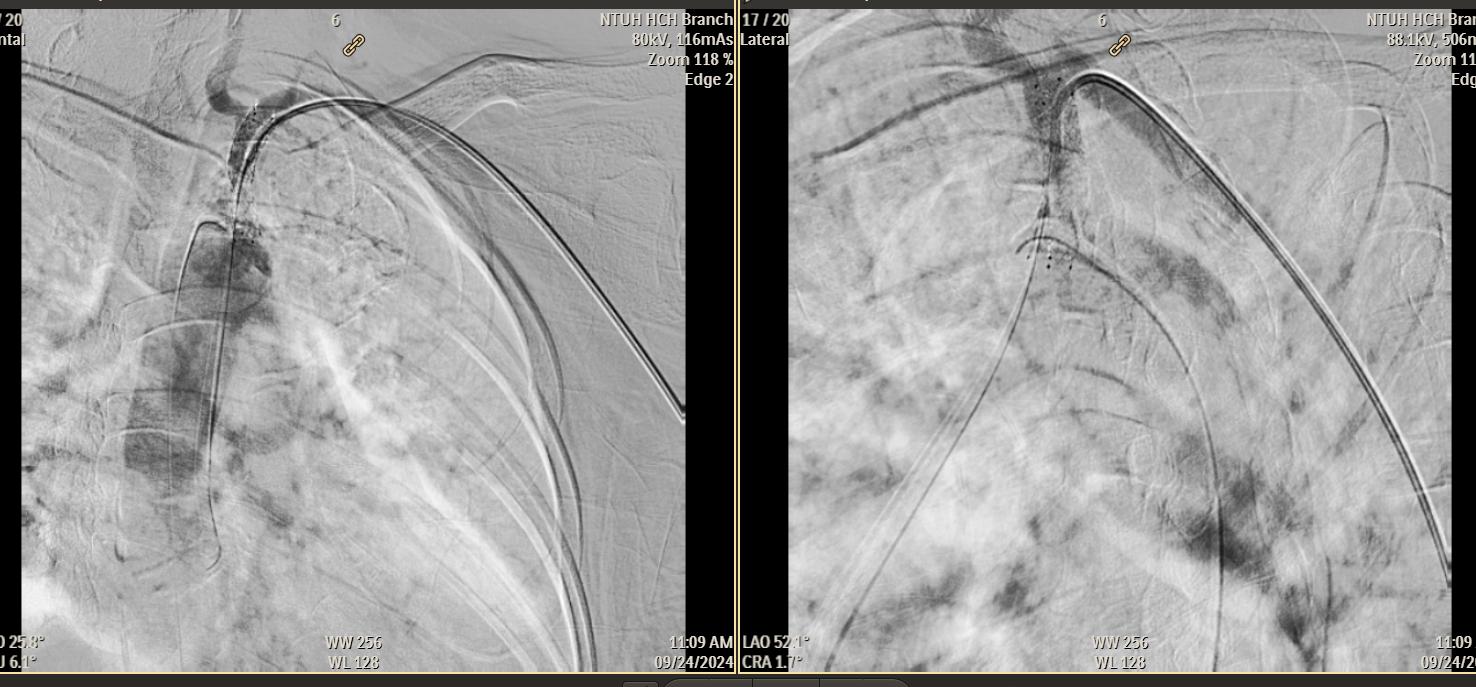
1. We performed the intervention via left radial artery approach and advanced 6Fr JR4 guiding catheter to left subclavian artery.2. Multiple attempts were made to access the left subclavian artery from a retrograde approach, but all failed.3. Successfully acrossed Astato 30 from left subclavian artery to aorta under micro-catheter CXI support.4. Performed balloon angioplasty with sterling balloon 2.5*120 mm up to 14 atm for 9 seconds.5. Performed balloon angioplasty with sterling balloon 5.0*40 mm up to 6 atm for 7 seconds.6. Failed to pass bare metal stent Visi-pro 6*27 mm from left subclavian artery to aorta.7. Tried to advance sterling balloon 5.*40 mm again to left subclavian artery but felt some force while advancing the balloon. The patient also complained left forearm pain at the same time.8. Checked the fluoroscopy and found the stent dislodged at left radial artery.9. Carefully pushed the stent to left subclavian artery with low pressure dilated balloon support.10. Antegradely crossed stiff 0.035 wire to left subclavian artery and performed angioplasyt with Passeo 6*40 mm up to 6 atm for 20 seconds.11. Successfully retrogradely across the bare metal stent to subclavian artery ostium, and deployed the stent up to 6 atm for 10 seconds.12. The residual stenosis was treated with stering balloon 5*40 mm and 7*20 mm post-diatation.13. Final angiography showed a significant improvement in the antegrade flow through subclavian artery.

Case Summary
Stent dislodgement is a rare complication of subclavian artery angioplasty. Stent loss can potentially lead to vascular occlusion, thrombosis, and limb ischemia. Therefore, retrieval of the stent is the principal goal of the intervention. If stent retrieval is infeasible, the displaced stent could be crushed against the blood vessel wall by another stent or parking in situ. Although our case demonstrated a successful rescue with inflation a low pressure balloon, it took the risk of vascular injury. Poor vascular preparation and calcified lesion are responsible for the tragedy. To avoid repeating the same mistakes, adequate vascular preparation and better support system are indispensable.