
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-049
Reevaluating Distal Cell Recrossing - A Case Study on Optimal Wire Positioning in Coronary Bifurcation Intervention
By Chieh-Yu Chang, Ming-Yun Ho
Presenter
Chieh-Yu Chang
Authors
Chieh-Yu Chang1, Ming-Yun Ho1
Affiliation
Chang Gung Memorial Hospital, Taiwan1,
View Study Report
TCTAP C-049
Coronary - Complex PCI - Bifurcation
Reevaluating Distal Cell Recrossing - A Case Study on Optimal Wire Positioning in Coronary Bifurcation Intervention
Chieh-Yu Chang1, Ming-Yun Ho1
Chang Gung Memorial Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
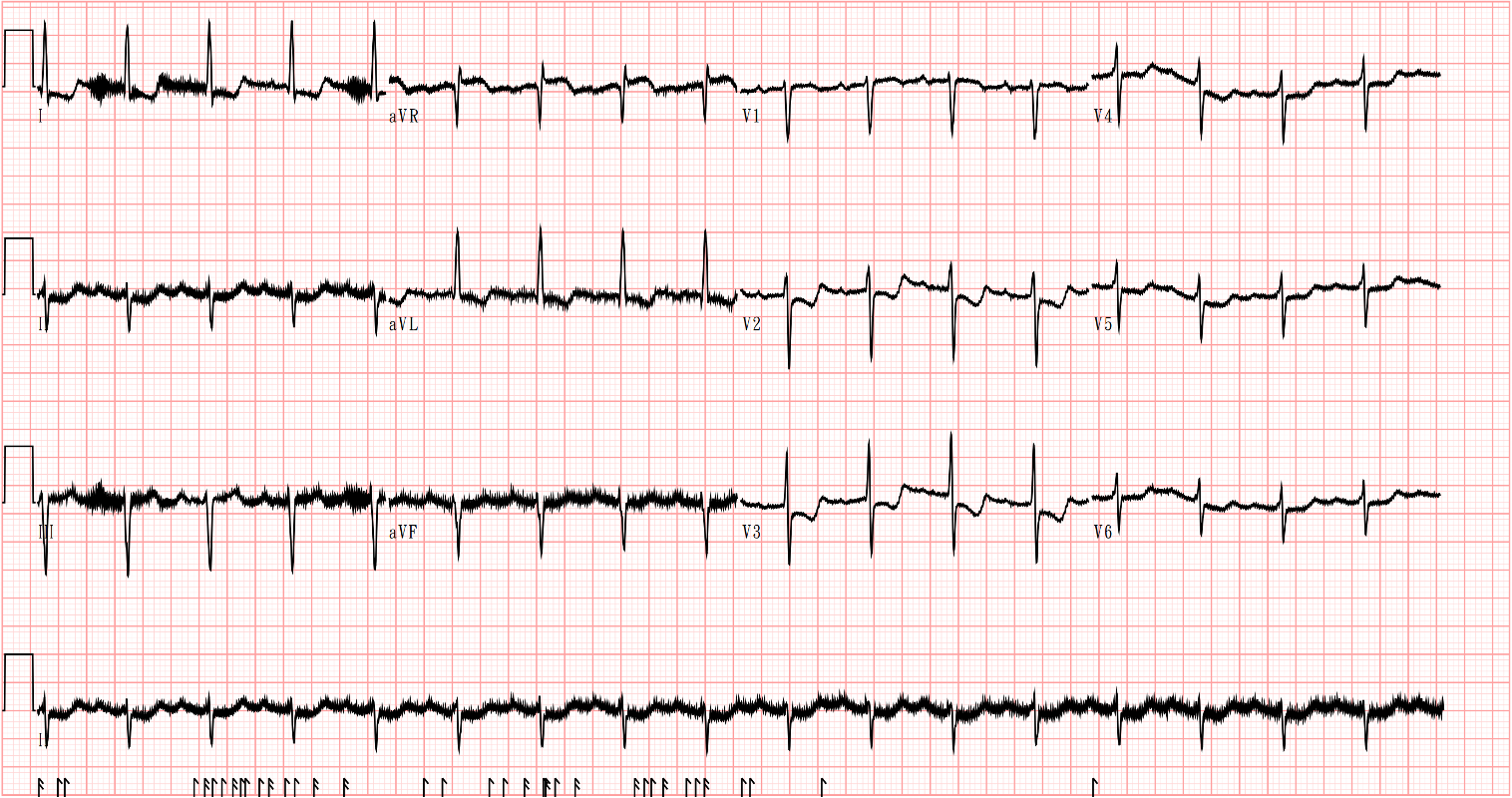
An 82-year-old woman with left main and triple-vessel coronary artery disease previously received two drug-eluting stents: one in the mid-LAD and another from mid-LM to mid-LCx. Her history included sick sinus syndrome with permanent pacemaker and end-stage renal disease on hemodialysis. She presented to the ED with four hours of typical angina and underwent immediate coronary angiography for anterior MI.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
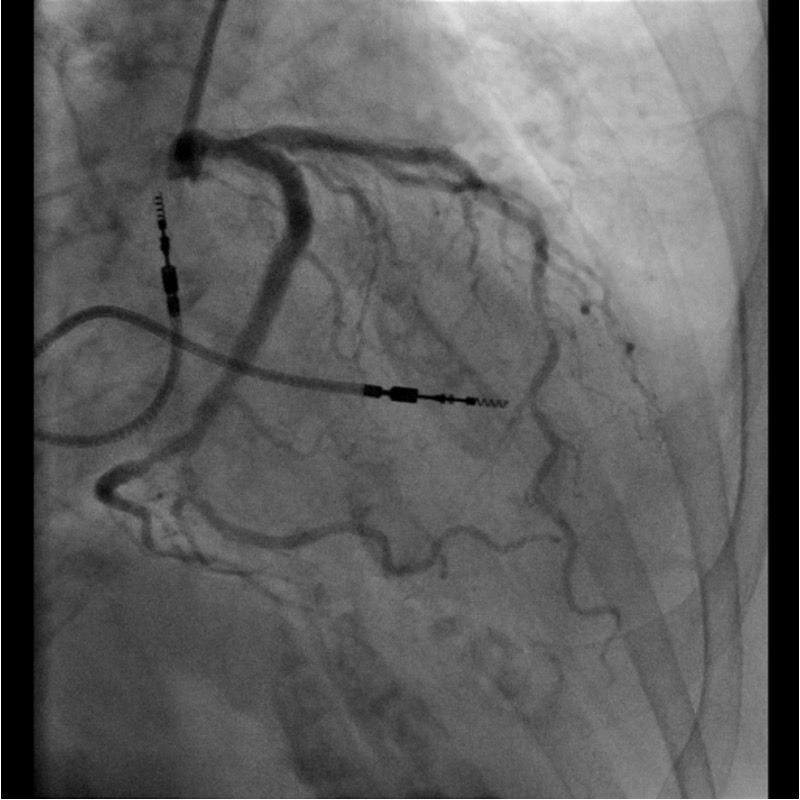
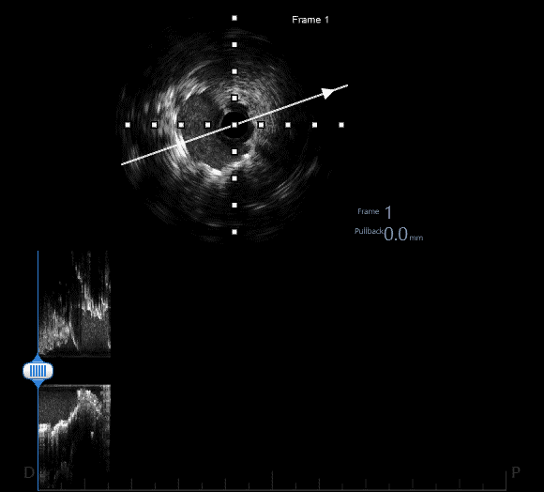
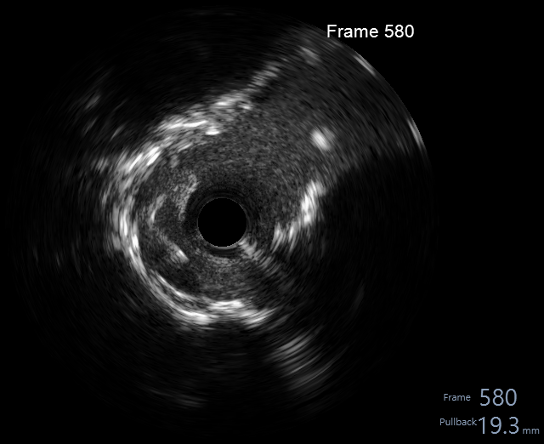
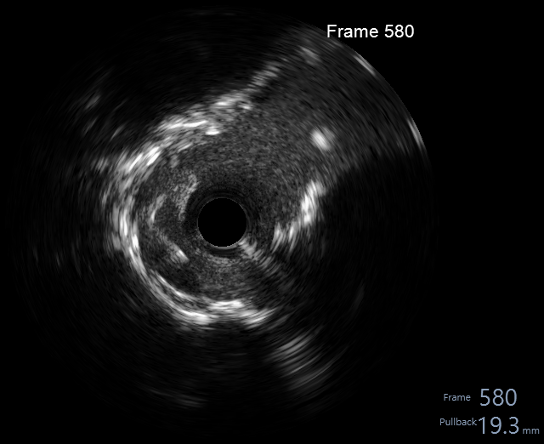
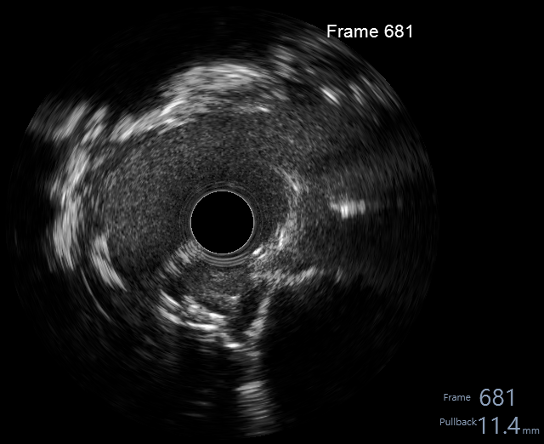
Angiography showed patent previous stent but new critical stenosis from distal LM to ostial LAD. Primary PCI using Culotte technique was performed with Medtronic Onyx 3.5x18mm stent under IVUS guidance. After distal cell wire-crossing and aggressive dilation (3.5mm NC@18atm + KBI with 3.0/3.5mm@12atm in LAD/LCx), IVUS revealed stent strut malapposition at ostial LCx.
Interventional Management
Procedural Step
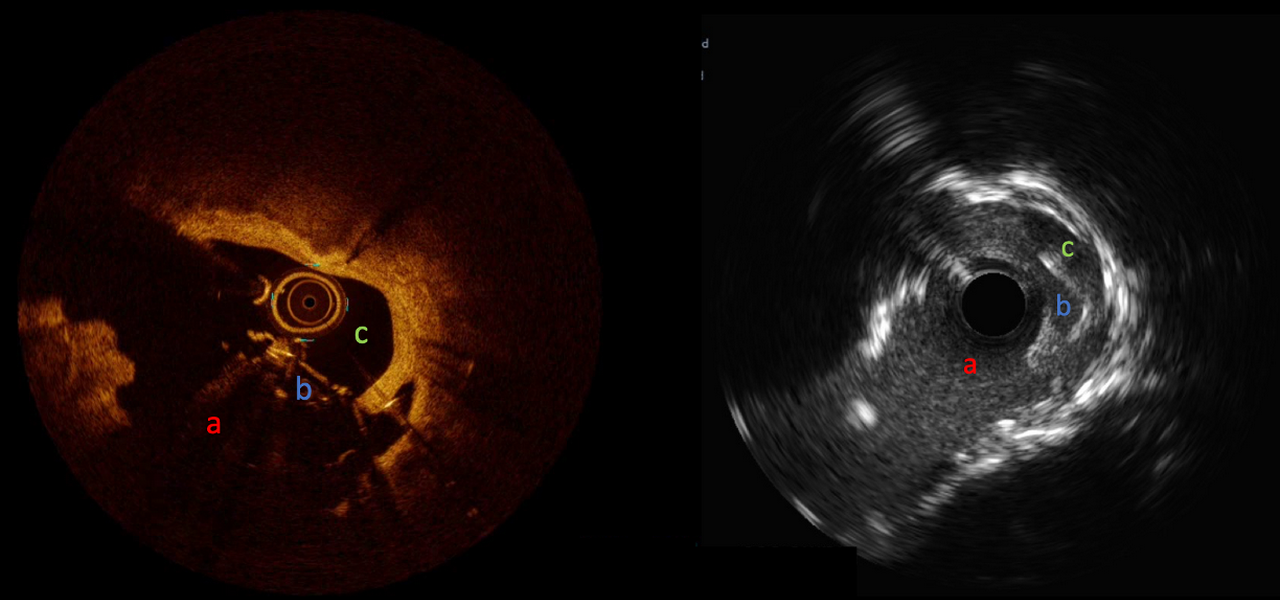
To correct stent misalignment, the wire was repositioned to more proximal cell under optical coherence tomography (OCT) guidance. The OCT analysis of LCx identified three stent cells near ostium. Cell a, the furthest, had been previously dilated and was intertwined with the edge of carina; Cell b, the second furthest, collapsed during the dilation of Cell a and became non-recrossable; and Cell c, the third, was selected for the current recrossing. Following this, we performed a KBI, leading to improved opening of side cell (Cell c) in LAD stent. However, this maneuver resulted in the formation of a centrally positioned neocarina due to proximal rewiring, as confirmed by both intravascular ultrasound (IVUS) and OCT imaging.
Case Summary
In bifurcation PCI, expert consensus recommends wire recrossing through the distal cell between carina and farthest stent ring for optimal side branch coverage. However, our case demonstrates that distal cell wiring may not always yield ideal results. When the farthest stent ring intersects the carina, OCT consensus suggests using the second most distal cell. While IVUS remains standard, its resolution limits may necessitate OCT guidance for precise wire placement and stent cell assessment in complex procedures.