
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-145
A Tale of Underexpanded Stent With Stuck Embolic Protection Device: Bail-Out Retrieval Using Intravascular Lithotripsy
By Wen-Shiann Wu, Meng-Han Tsai
Presenter
Meng-Han Tsai
Authors
Wen-Shiann Wu1, Meng-Han Tsai1
Affiliation
Chi-Mei Medical center, Taiwan1,
View Study Report
TCTAP C-145
Coronary - Complication Management
A Tale of Underexpanded Stent With Stuck Embolic Protection Device: Bail-Out Retrieval Using Intravascular Lithotripsy
Wen-Shiann Wu1, Meng-Han Tsai1
Chi-Mei Medical center, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 76-year-old man with a history of hypertension and type 2 diabetes mellitus presented to the emergency room after experiencing intermittent chest tightness and progressively worsening shortness of breath over the past two days. Elevated cardiac enzyme levels were detected upon evaluation. He received an aspirin loading dose and a heparin infusion. His blood pressure was stable. Physical examination revealed bilateral lung crackles and a systolic murmur at the right upper sternal border.

Relevant Test Results Prior to Catheterization
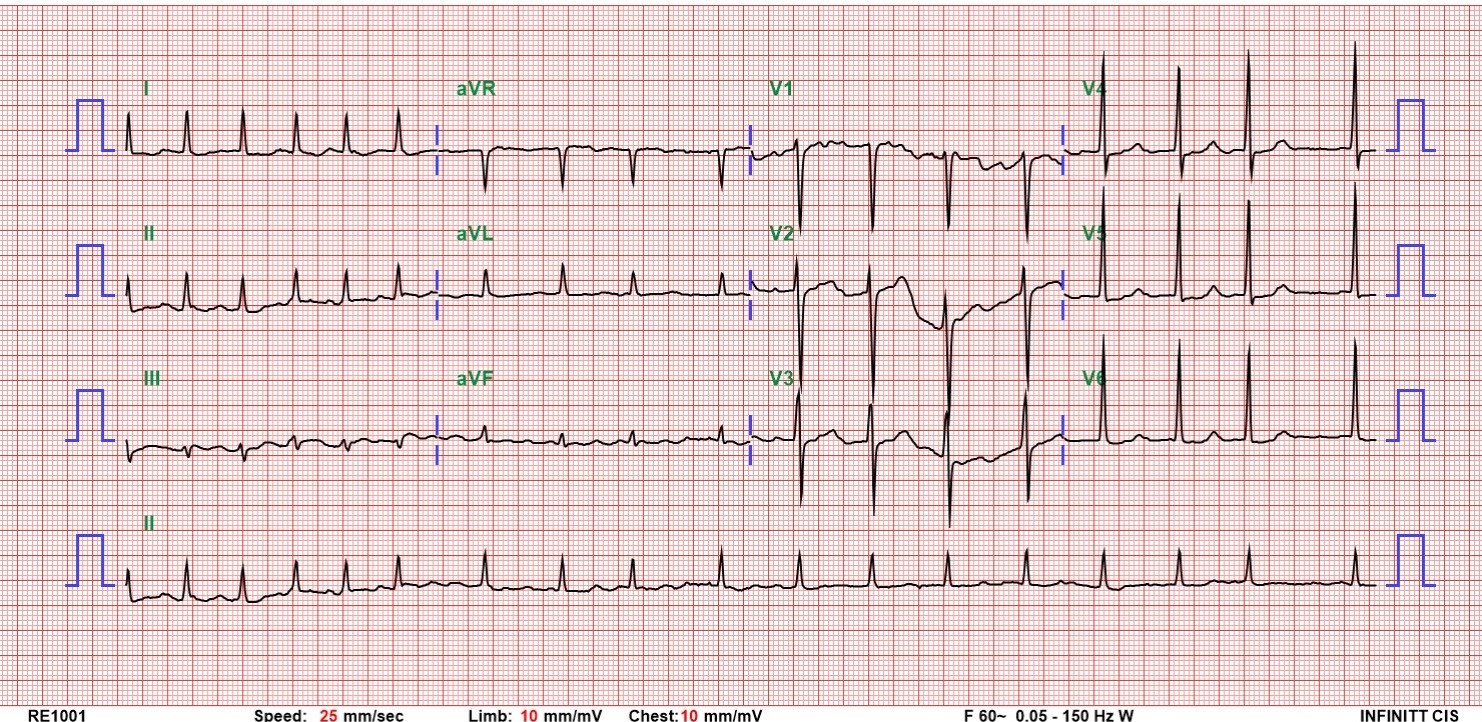
A chest X-ray revealed bilateral pulmonary edema and pleural effusion. The EKG showed atrial fibrillation with non-specific ST-T changes. Cardiac enzymes peaked at hs-Troponin I of 13,591 pg/ml. The patient was admitted to the cardiac intensive care unit with a tentative diagnosis of NSTEMI.
Relevant Catheterization Findings
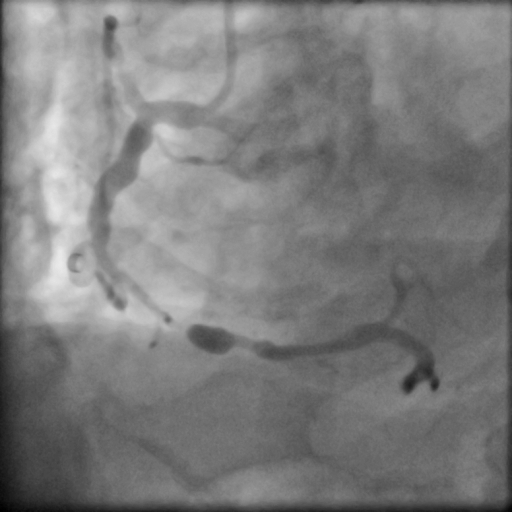
Coronary angiography showed 2-vessel coronary artery disease with severe stenosis in mid to distal-RCA and TIMI-2 flow. Small balloon pre-dilatation, followed by manual IVUS pullback performed. We noted mostly fibrous plaques but some lipid pools along the vessel with a short segment of heavy calcification. Thus an embolic protection device was placed smoothly in distal-RCA. Next lesion preparation with a 3.5x30mm balloon. Unfortunately we failed to notice incomplete balloon expansion in mid-RCA.


Interventional Management
Procedural Step
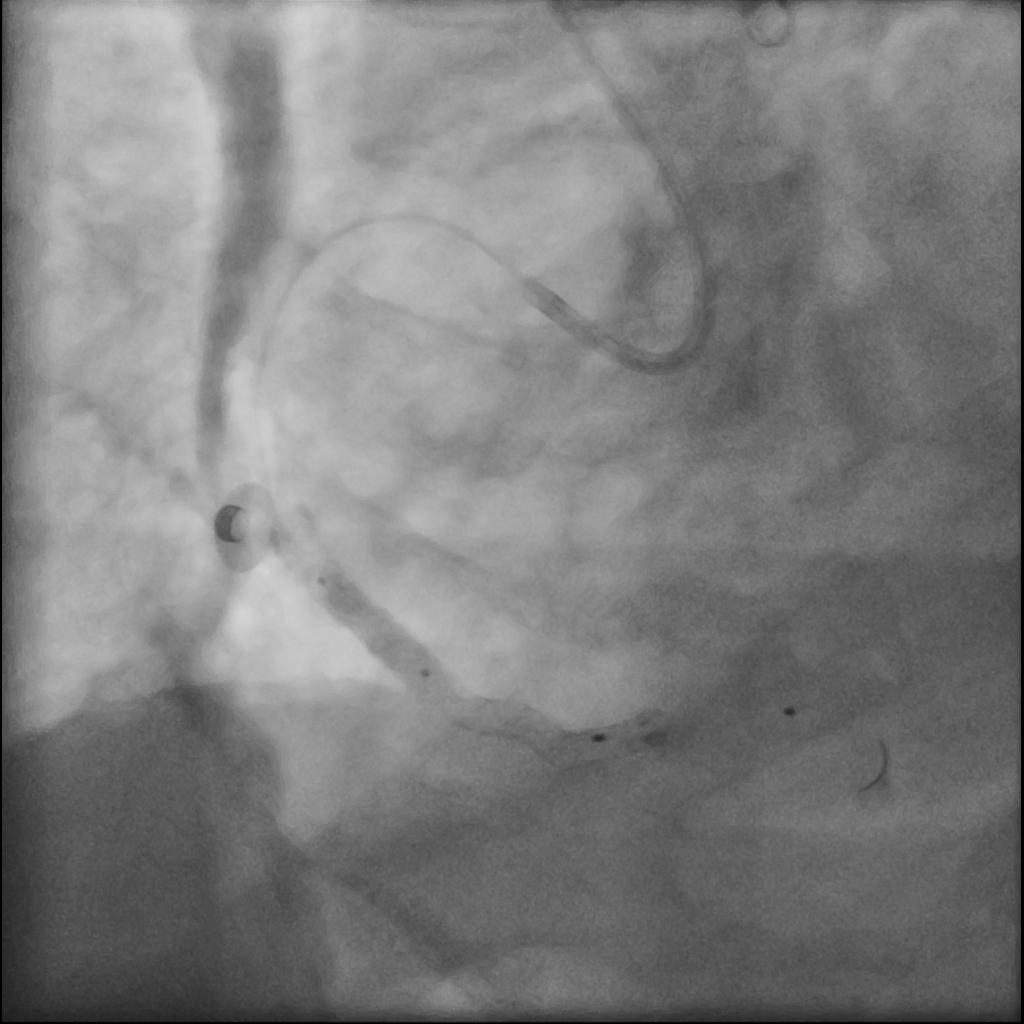
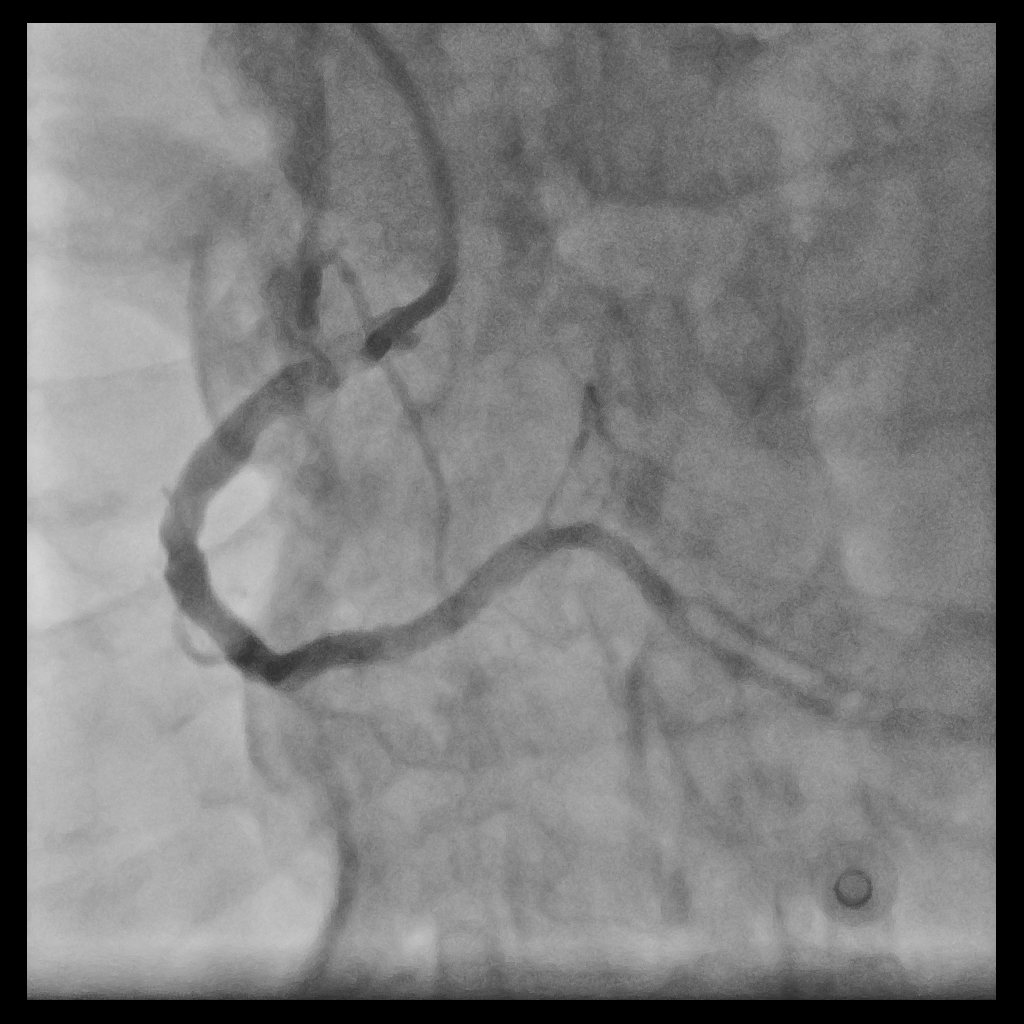
Using an AL1 guiding catheter, we navigated to the RCA-PDA. We performed balloon dilatation of the lesions in the RCA-M to RCA-D. IVUS with manual pullback revealed fibrous plaques with lipid pools and a glimpse of circumferential calcification in the RCA-M. We positioned the Spider FX embolic protection device with its filter basket in the RCA-D. Lesion preparation was done with a Euphora 3.5x30mm balloon. Stent deployment involved deep seating and using a guide extension catheter (GEC) to deploy an Ultimaster-Nagomi 3.5x44mm stent from RCA-M to RCA-D and another Ultimaster-Nagomi stent in the RCA-M. Notable underexpansion was observed in the middle part of the RCA-M stent . Post-dilatation was performed with an NC Accuforce 4.0x15mm balloon at 28 ATM. However, the RCA-M remained non-dilatable with persistent stent underexpansion. IVUS confirmed extensive circumferential calcification in the RCA-M. Despite multiple attempts using the GEC and balloon anchoring technique, we couldn't retrieve the Spider catheter's basket. We then used an intravascular lithotripsy balloon to deliver shockwaves to the proximal calcium ring, alternating with NC balloon inflations. Fortunately this inch-worm advance of the IVL achieved full stent expansion. Eventually, using an anchor balloon with GEC, we successfully retrieved the filter basket. The final angiography showed TIMI-3 flow in the RCA without any hemodynamic change throughout the procedure. A small emboli was found in the filter basket.

Case Summary
Embolic protection devices are effective for preventing distal embolization in lesions with lipid pools. However, it's crucial to conduct a thorough review of intravascular images and ensure adequate lesion preparation. In cases where stent underexpansion occurs in heavily calcified lesions, we recommend using intravascular lithotripsy as a bail-out method.