
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-097
Shocking Scene "When You Face CTO in ACS, to Proceed or Not?"
By Salma Mohamed Elshokafy, Ramy Mohamed Atlm
Presenter
Salma Mohamed Elshokafy
Authors
Salma Mohamed Elshokafy1, Ramy Mohamed Atlm1
Affiliation
Tanta University Hospital, Egypt1,
View Study Report
TCTAP C-097
Coronary - Complex PCI - CTO
Shocking Scene "When You Face CTO in ACS, to Proceed or Not?"
Salma Mohamed Elshokafy1, Ramy Mohamed Atlm1
Tanta University Hospital, Egypt1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
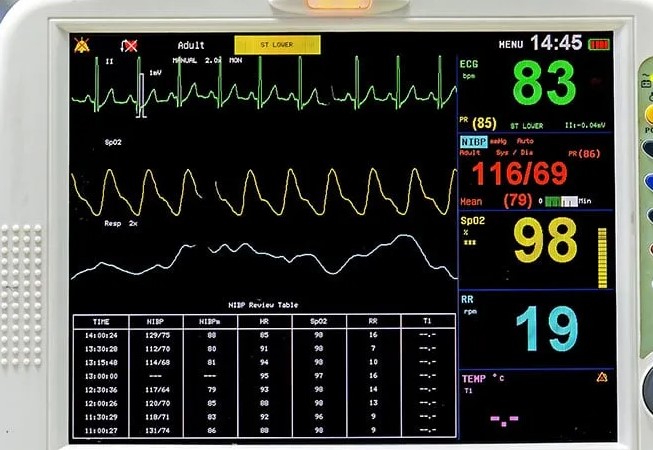
Male patient, 35 years old , Smoker , Diabetic ,Dyslipidemic , History of Multiple sclerosis since 2010 receiving Steroids . Presented with Typical anginal pain recurrent for 3 days and maximum 10 hrs before presentation to ED. Generally : No signs or symptoms of heart failure Local ex: Audible HS with no added murmurs Bl pr : 116 / 69 , HR 83 b/m , Temp: 37.2 , RR : 19
Relevant Test Results Prior to Catheterization
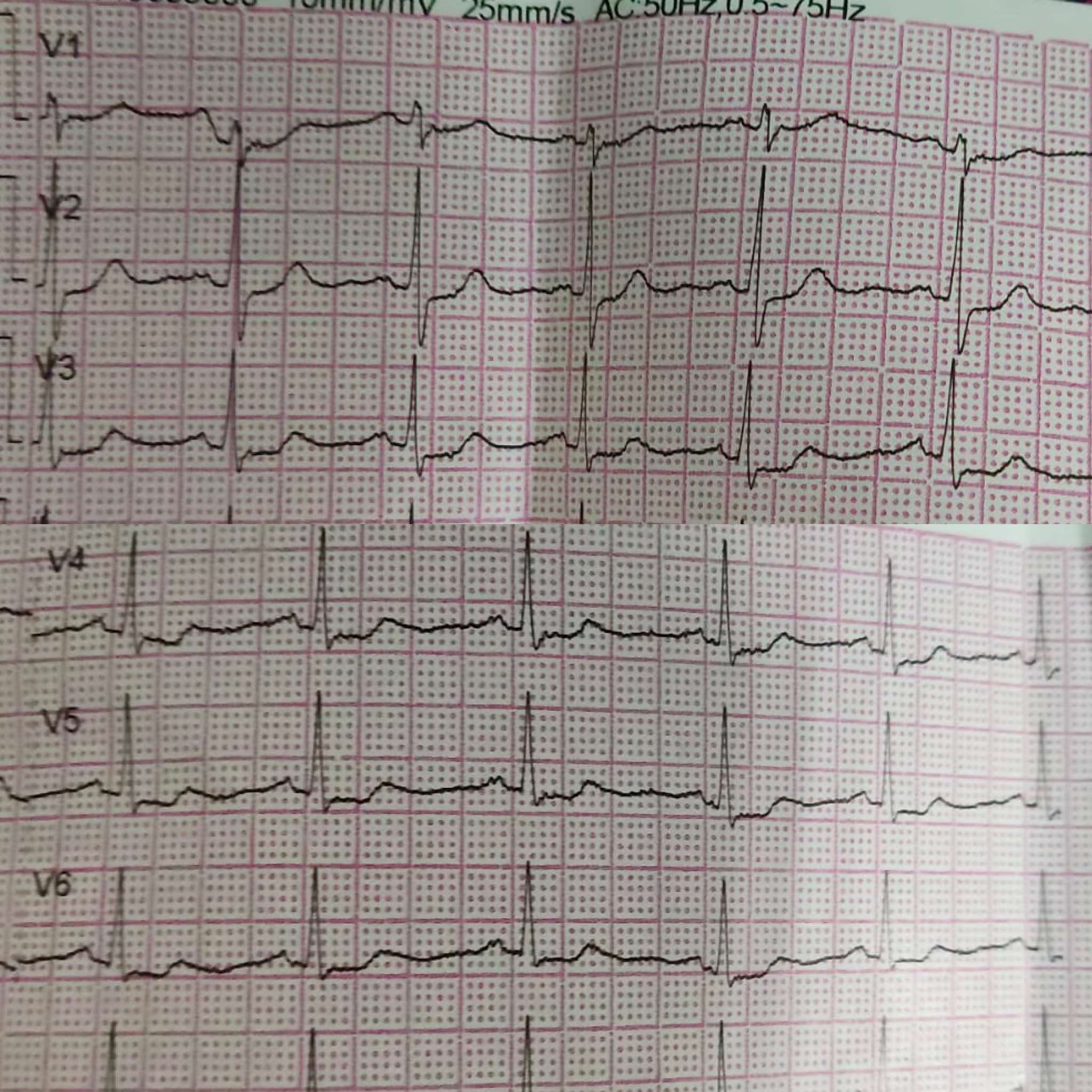
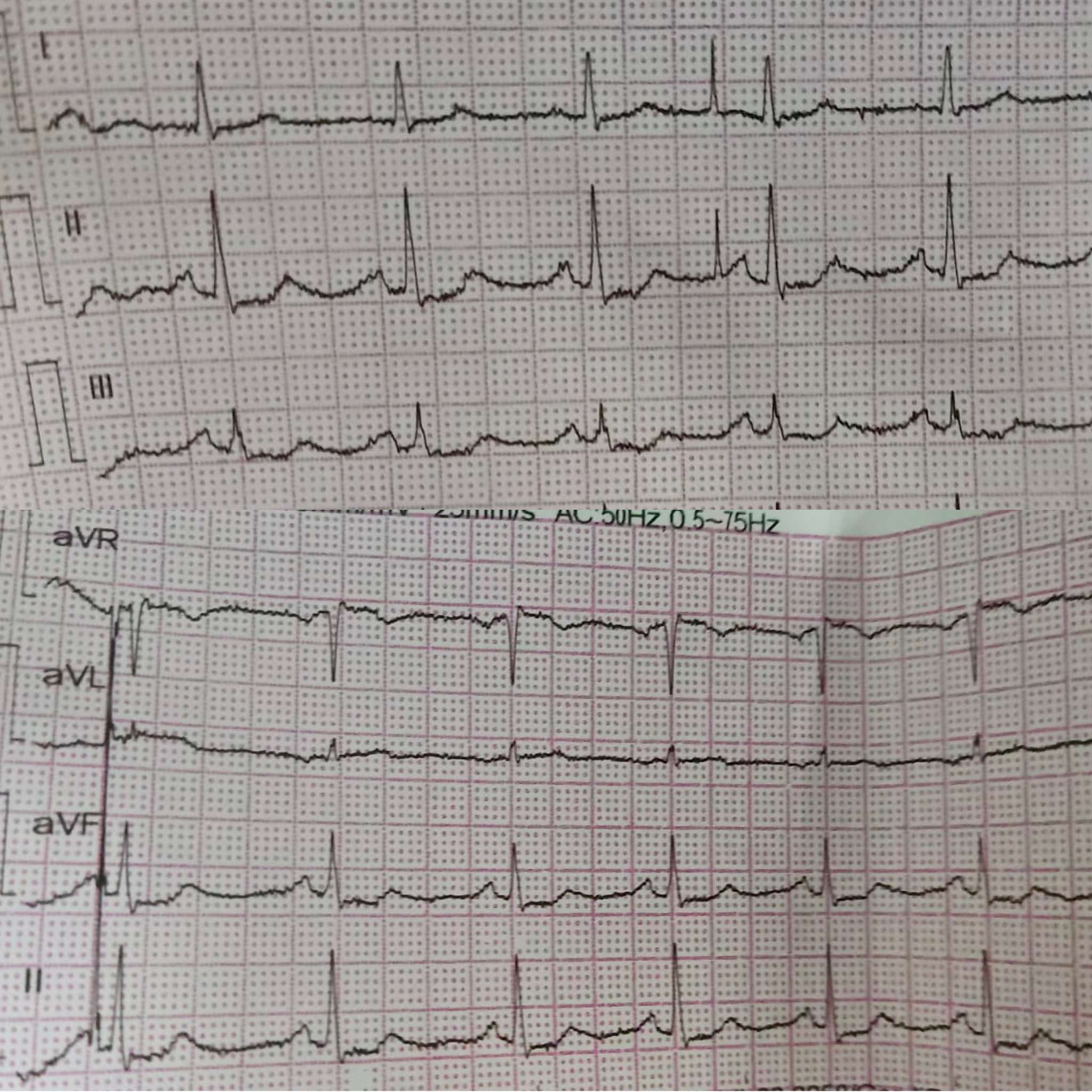
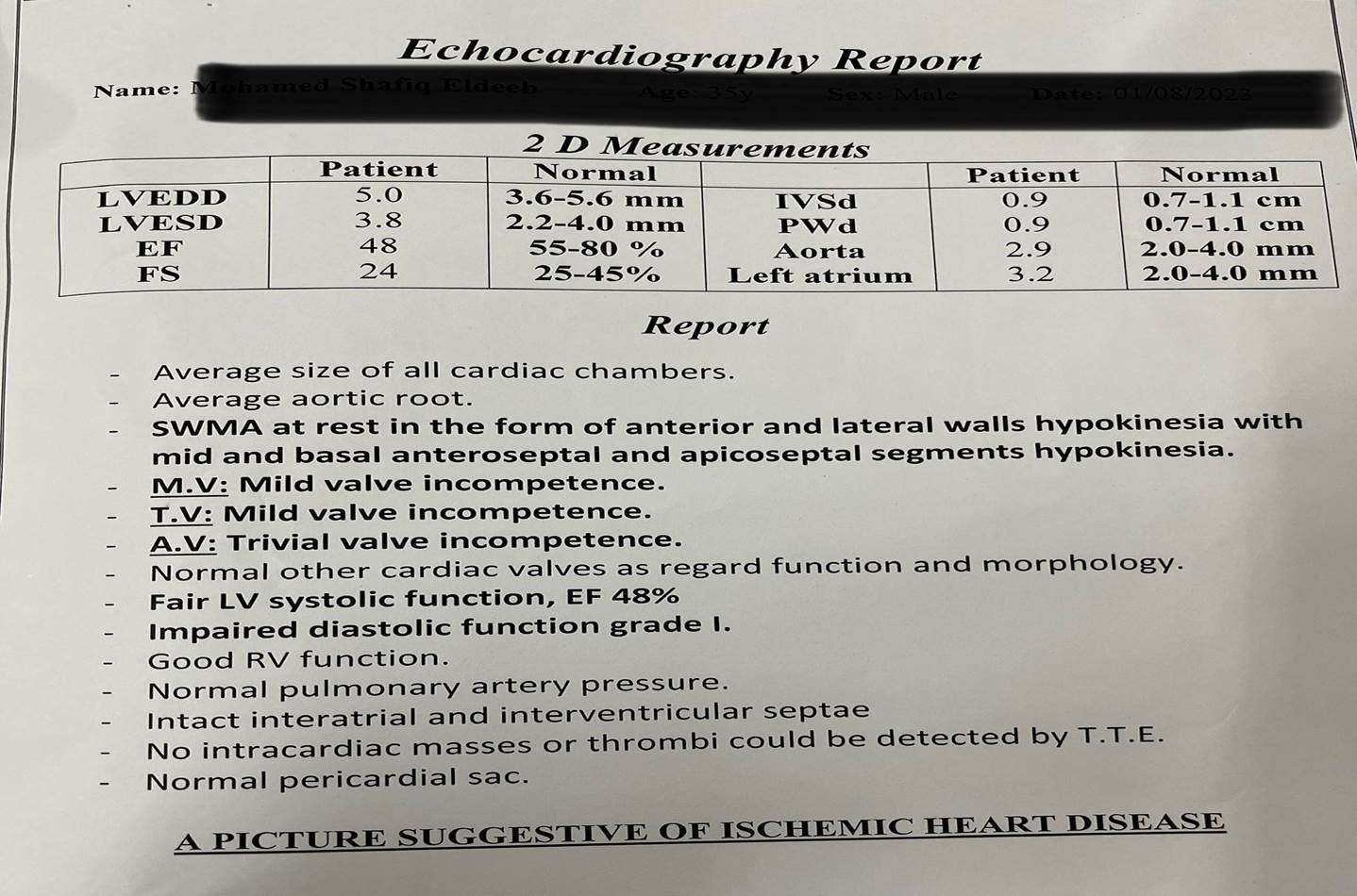
RBS : 326 ECG shows : Sinus Rhythm with ST depression in all leads and elevation AVR wave Echo shows : ischemic heart disease with EF 48 % , segmental wall motion in the form of mid and basal anterior , anteroseptal and lateral wall hypokinesia with no significant valvular lesions All other laboratory investigations were unremarkable except for Positive Troponin , Elevated CKMB 180 and un controlled diabetes Markedly ( elevated HBA1C )
Relevant Catheterization Findings
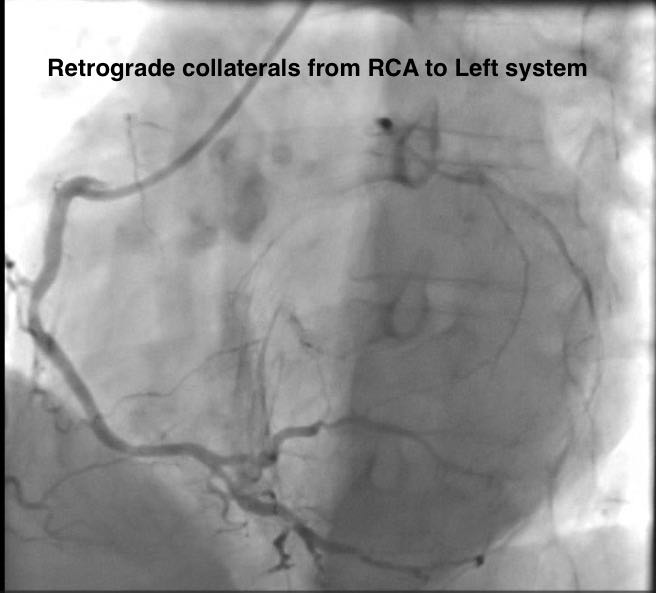
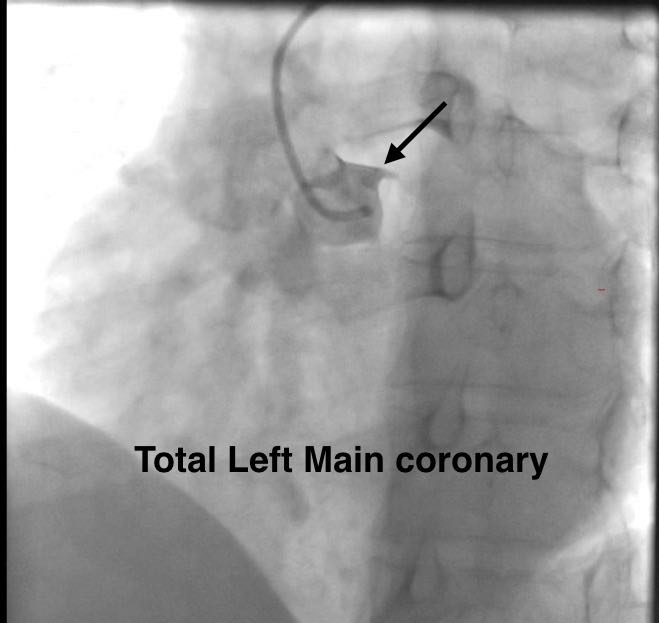
LM : Atherosclerotic vessel with Total occlusion.RCA : Atherosclerotic vessel with non significant lesions , giving retrograde collaterals to left system .
Interventional Management
Procedural Step
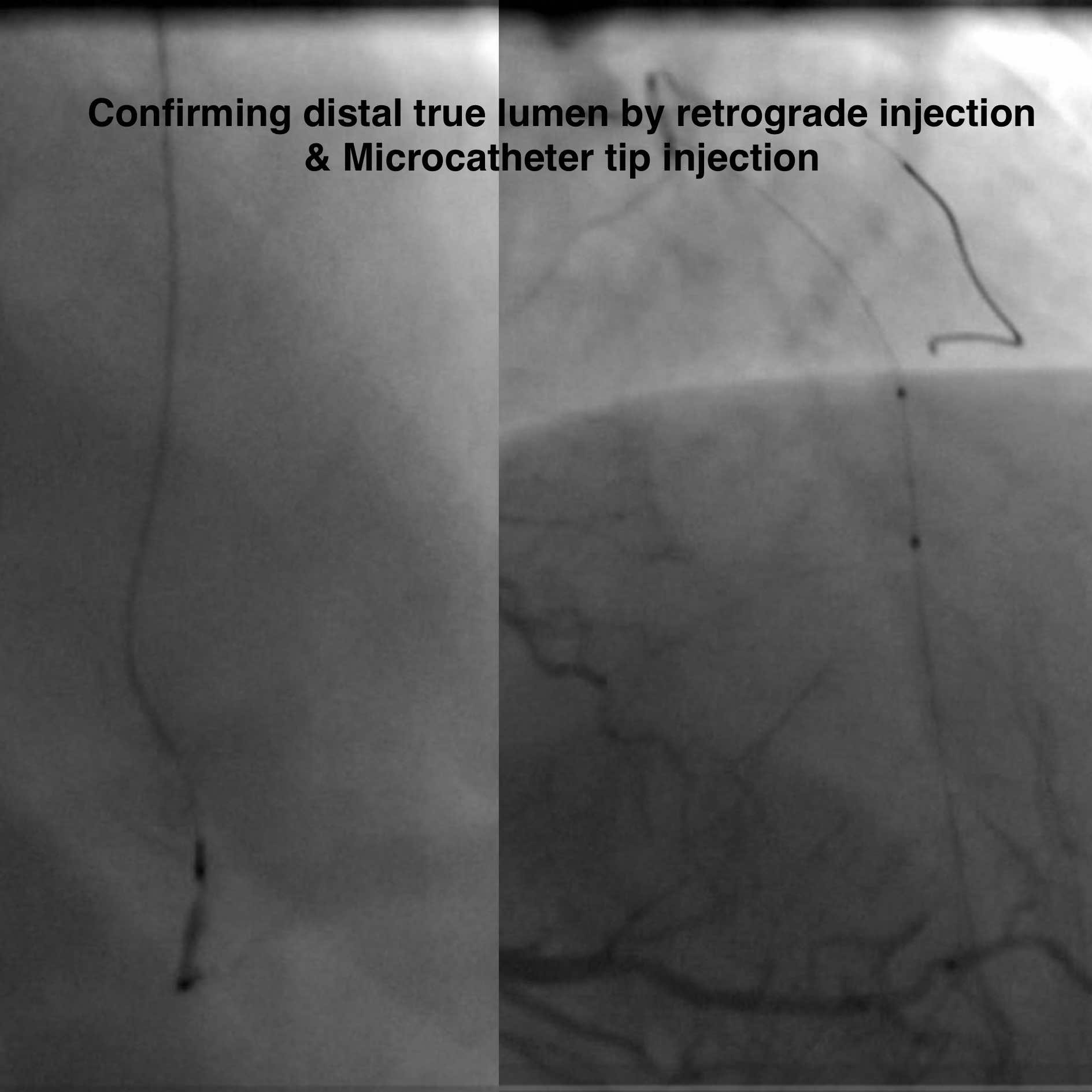
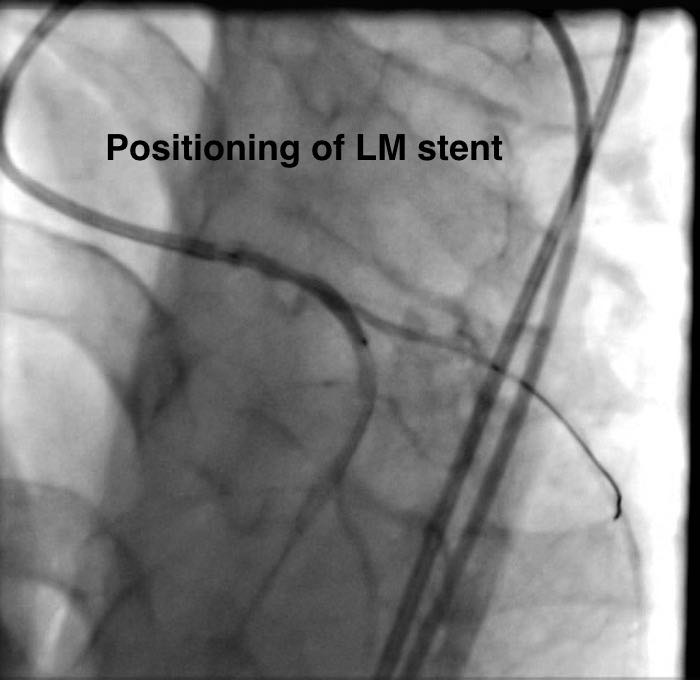
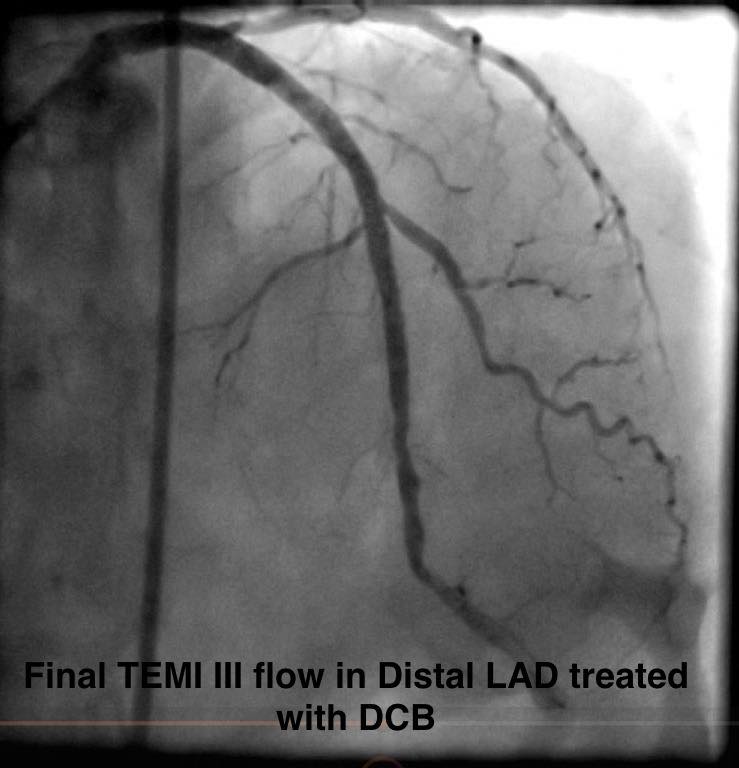
Engagement of LM with Guiding Cath XB 3.5 7F, Wiring of LAD with FIELDER XTA over a CARAVEL MC ,The wire succeeded to go easily so we decided to confirm wire position through retrograde injection that shows the wire in a Diagonal branch , We decided to open LM first with a 3.25 * 15 mm Balloon , We exchanged the Diagonal wire with a regular wire and another wire was introduced into LCX with confirming positions with both ante and retrograde injections , We tried to negotiate the Mid segment CTO LAD with FIELDER XTA wire over the MC , The wire go through dissection , so left in place and another parallel wire was used to track true lumen , The ( Runthrough ) wire succeeded to track true lumen Confirmed by retrograde injection , Confirming we are True Lumen with MC injection, Then PTCA at site of CTO with 2 * 15 mm Balloon , Stenting of Ostial LM-LAD with 4 * 23 DES with post-dilatation , and we decided not to stent whole LAD dissection ( INVESTMENT PROCEDURE ) and to perform control angiography again , which was done three month later showing midsegment LAD lesion which was stented with 3 * 48 mm DES and treated distally with Drug coated balloon with final good angiographic results and TEMI III flow
Case Summary
In Conclusion , According to Esc guidelines for Risk Stratification of NON-STEMI patient , he is considered high risk due to Dynamic ECG changes & Elevated cardiac enzymes . So, Early invasive PCI in the first 24 hours was indicated , But after angiography there was a debate about either to proceed to PCI or CABG , So we discussed with the Heart Team together with the respection of patient and close relatives decision and proceeded for a high risk procedure . Studies suggest that MS is associated with an increased risk of cardiovascular disease that is related to genetic factors & inflammatory process.In a high risk PCI , study your patient well , put a proper plan , Be well equipped .