
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-046
The Hanging Stent - Reverse Culotte Saved the Day
By Richa Sharma, Himanshu Rana
Presenter
Himanshu Rana
Authors
Richa Sharma1, Himanshu Rana2
Affiliation
Shri Mehant Indresh Hospital, India1, Graphic Era Institute of Medical Science, India2,
View Study Report
TCTAP C-046
Coronary - Complex PCI - Bifurcation
The Hanging Stent - Reverse Culotte Saved the Day
Richa Sharma1, Himanshu Rana2
Shri Mehant Indresh Hospital, India1, Graphic Era Institute of Medical Science, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
•65year old male,k/c/o hypertension p/w c/o acute onset chest pain since 1day prior to admission.
• O/EBP- 144/80, HR- 82bpm, Chest and CVS- NAD
•2DEcho s/o LVEF- 42%, LAD territory hypokinetic, No MR/AR/TR
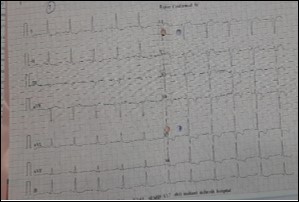
•ECGs/o ST coving with T inv in V2-V6
•Pt wasexplained for CAG+- revascularization
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
CAG- mLAD95%, Ostial-proxdiagonal (long segment) 99%,distal LAD critical disease
RCA and LCX normal


RCA and LCX normal
Interventional Management
Procedural Step
Initialplan was to do a LAD-D1 bifurcation by TAP
RRA, EBU 3.0/6f, Runthrough NS in LAD, Whisper ES in D1, To secure diagonal, D1was first dilated with 2.0*10mmSC balloon @6atm
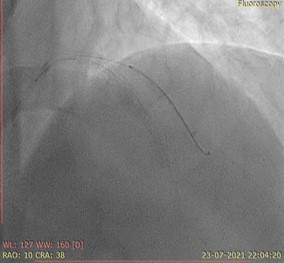
While pulling and positioning the D1 stent, shaft of stent broke from soft partof the balloon within the guide catheter. Stent was lying hanging uninflated inthe D1.
So, now the plan was to dilate the diagonal stent struts.


RRA, EBU 3.0/6f, Runthrough NS in LAD, Whisper ES in D1, To secure diagonal, D1was first dilated with 2.0*10mmSC balloon @6atm
While pulling and positioning the D1 stent, shaft of stent broke from soft partof the balloon within the guide catheter. Stent was lying hanging uninflated inthe D1.
So, now the plan was to dilate the diagonal stent struts.
Case Summary
The incidence of stent dislodgement ranges from0.3-8%