
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-042
When a DK Crush Is Not a DK Crush: The Use of Intra Vascular Imaging in Bifurcation Stenting
By Matthew Hordern, Sarah Fairley, Scott Harding
Presenter
Matthew Hordern
Authors
Matthew Hordern1, Sarah Fairley1, Scott Harding1
Affiliation
Wellington Hospital, New Zealand1,
View Study Report
TCTAP C-042
Coronary - Complex PCI - Bifurcation
When a DK Crush Is Not a DK Crush: The Use of Intra Vascular Imaging in Bifurcation Stenting
Matthew Hordern1, Sarah Fairley1, Scott Harding1
Wellington Hospital, New Zealand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
An 84 year old male presented with a non-ST elevation myocardial infarcton (NSTEMI). An echocardiogram demonstrated overall preserved left ventricular function and no significant valvular abnormalities. A subsequent coronary angiogram demonstrated severe left main coronary artery (LMCA) bifurcation stenosis (Medina 1,1,1).
Relevant Test Results Prior to Catheterization
Left main bifurcation stenting was performed using intravascular ultra sound (IVUS) guided double kiss (DK) crush bifurcation stenting technique after calcium modification with orbital atherectomy.
Relevant Catheterization Findings
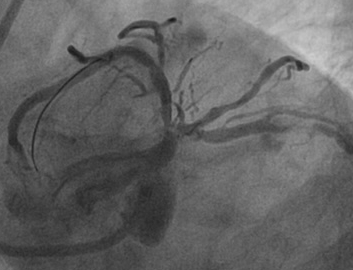
The patient represented 4 days later with a further NSTEMI. A repeat coronary angiogram demonstrated an opacity at the ostium of the circumflex (LCx).

Interventional Management
Procedural Step
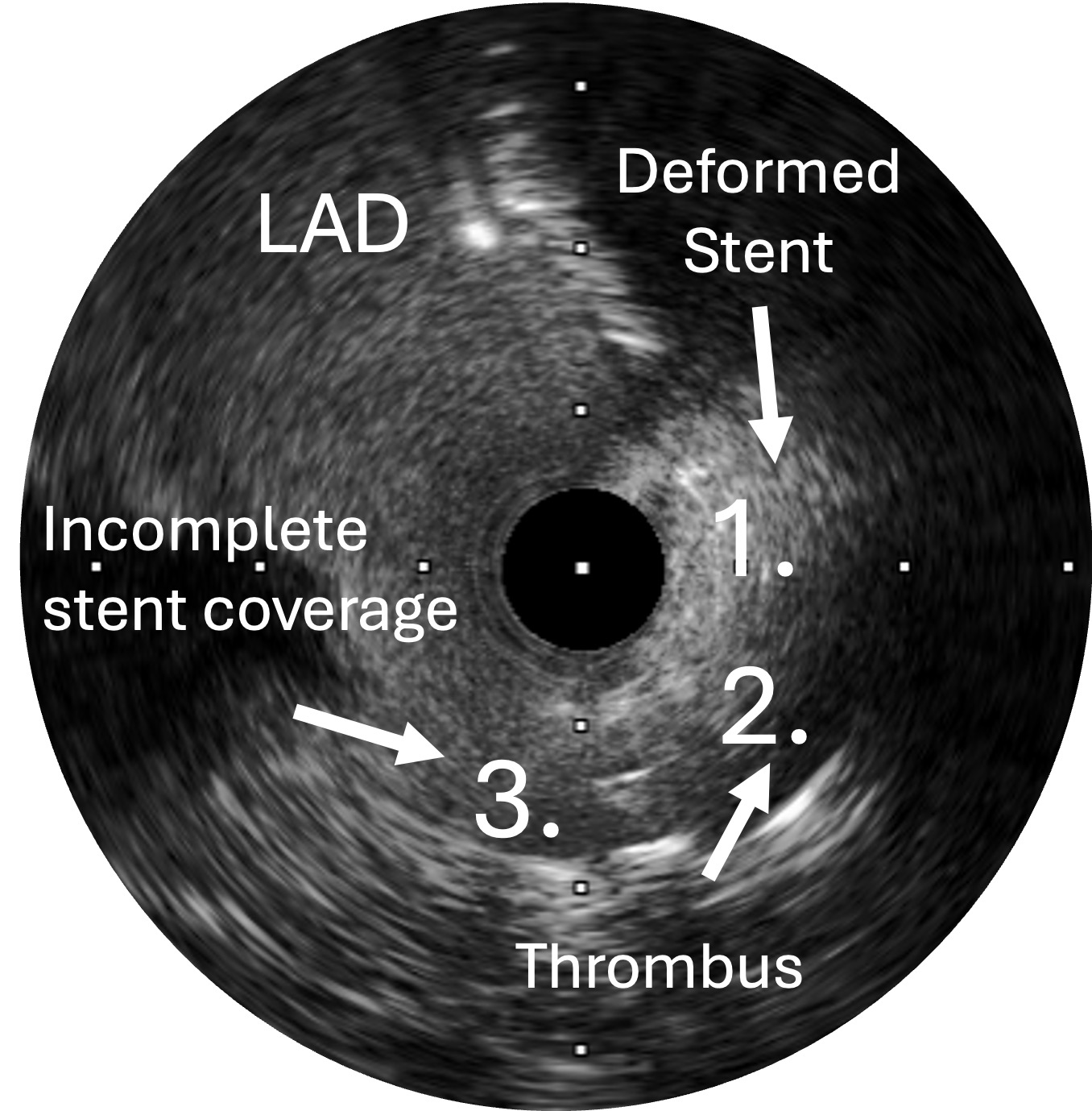
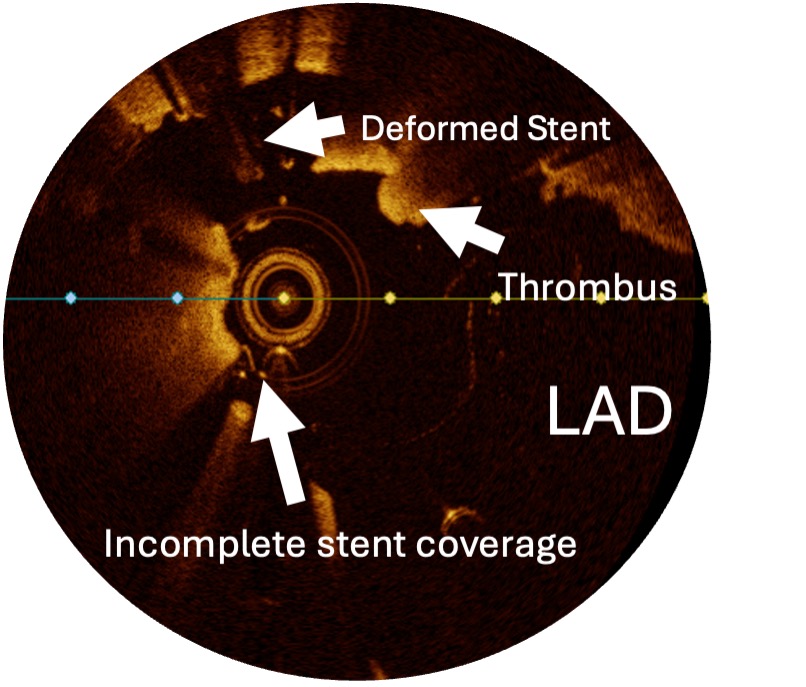
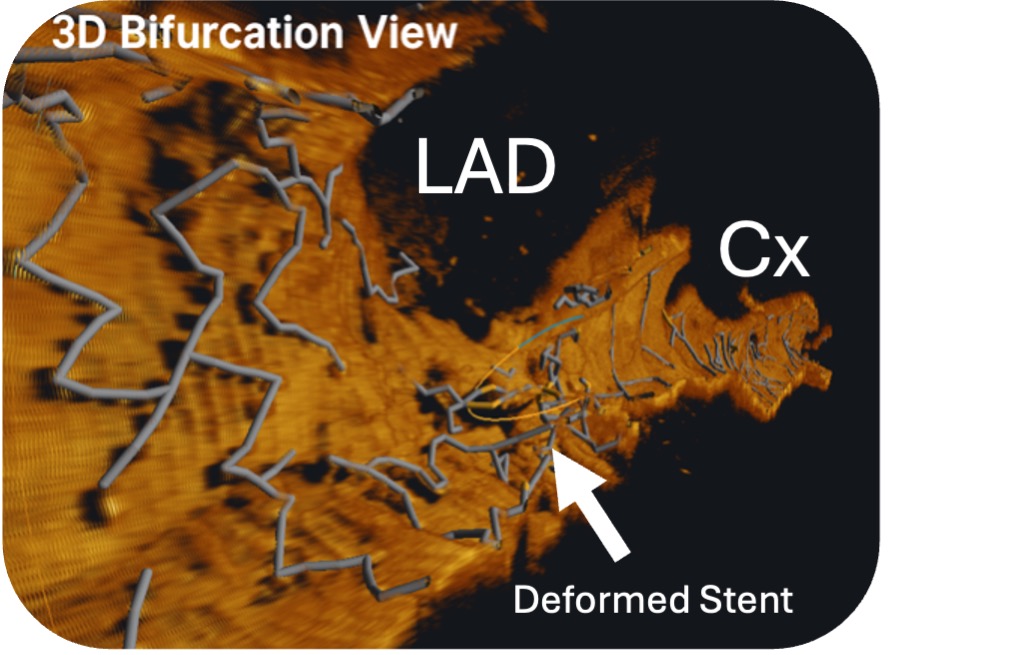
IVUS of the LCx suggested stent deformation at the ostium with associated thrombus. Optical coherence tomography (OCT) confirmed deformation of the ostial LCx stent away from the carina with associated thrombus and incomplete stent coverage at the carina side of the ostium. To solve this problem we stented from the LCx into the left main as a reverse culotte. We then performed proximal optimisation technique (POT) with a 5.0mm non-compliant (NC) balloon and subsequently recrossed (mid to distal into the LAD. The recess wire position was confirmed on OCT. We then performed sequential high pressure inflations and a final KISS with a 4.0mm NC balloon in the LAD and 3.5mm NC balloon in the LCx. Finally a repeat POT in the LMCA.
Case Summary
The mechanism of the stent deformation was sub-optimal and distal wire recrossing into the LCx during the bifurcation stenting. Initially when the DK crush was first described Chen and colleagues (Chin Med J 2005;118(20):1746-1750) recommended a proximal recross in DK Crush, however, more recently there has been a shift to achieve a more distal recross to minimise the neocarina. Unintentional stent deformation is an underrecognized and common problem. This case highlights the importance of optimal wire re-cross when performing bifurcation stenting with DK crush. Intravascular imaging should be used to confirm recross wire position for optimal outcomes