
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-099
Comprehensive Management for an Elder Patient With Complex Coronary Artery Disease and Critical Aortic Stenosis by Multidisciplinary Team
By Cheng-Yu Hung
Presenter
Cheng-Yu Hung
Authors
Cheng-Yu Hung1
Affiliation
Taichung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-099
Coronary - Complex PCI - CTO
Comprehensive Management for an Elder Patient With Complex Coronary Artery Disease and Critical Aortic Stenosis by Multidisciplinary Team
Cheng-Yu Hung1
Taichung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
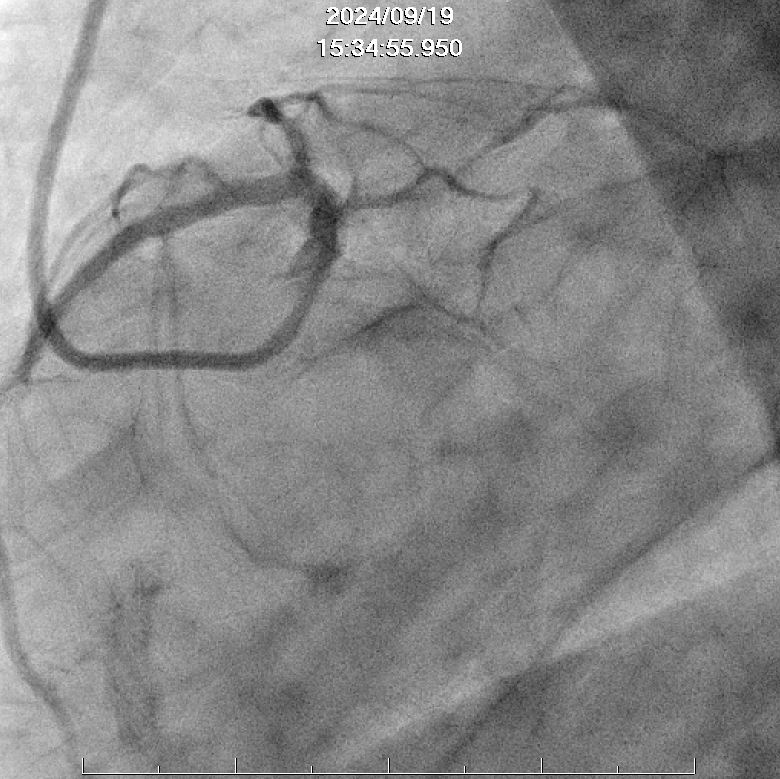
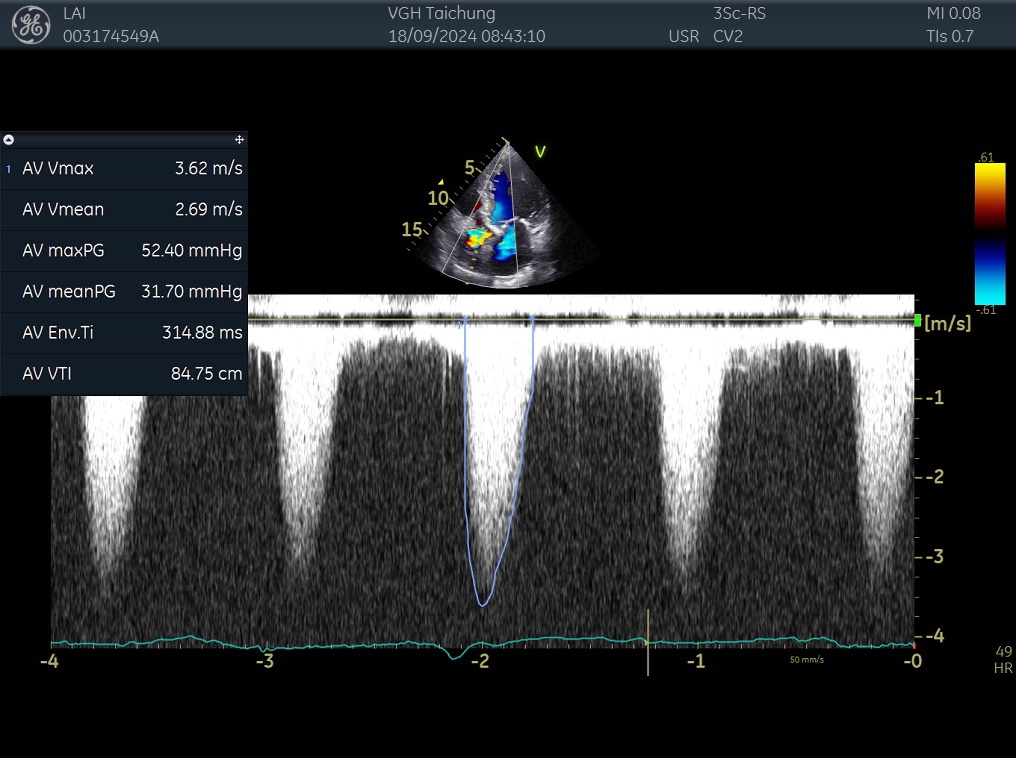
The 89 y/o male had disease history of CAD post stenting 10 years ago, heart failure, type 2 DM. He suffered from fever, productive cough and dyspnea for days and was admitted under the diagnosis of pneumonia and NSTE-ACS. The echocardiogram disclosed severe AS and first cardiac catheterization showed CTO of LCx, CTO of RCA related to ISR and de-nova stenosis over LAD middle part. PCI for LAD was done.
However, cardiac arrest with rhythm of VT/Vf developed in the following admission course.
However, cardiac arrest with rhythm of VT/Vf developed in the following admission course.
Relevant Test Results Prior to Catheterization
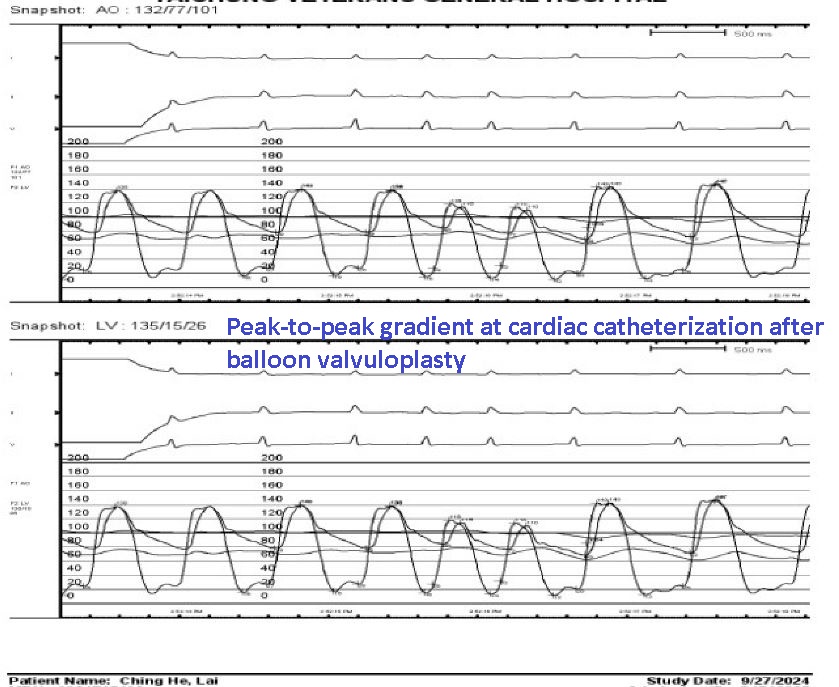
We did catheterization again. The angiogram showed patent LAD. We did balloon valvuloplasty for aortic stenosis, and trans-aortic pressure gradient decreased. We corrected electrolyte imbalance and anti-arrhythmic treatment with lidocaine was administered. However, there was still frequent ventricular arrhythmia. Pulsesless, polymorphic VT, followed by Vf attacked again, with duration of less than one minute and resolved without defibrillation. Based on electrical storm, we did PCI for RCA CTO.

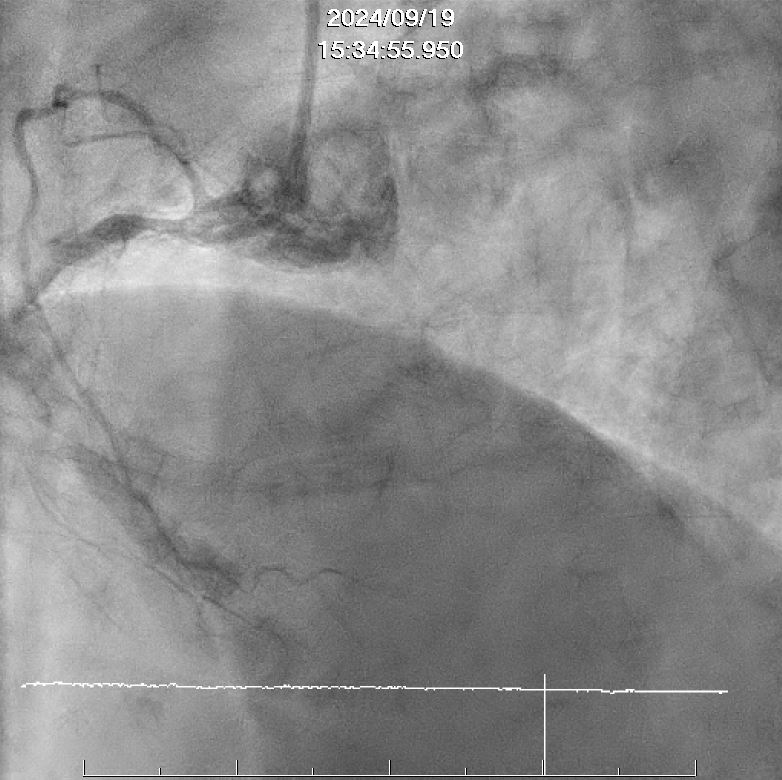
Relevant Catheterization Findings
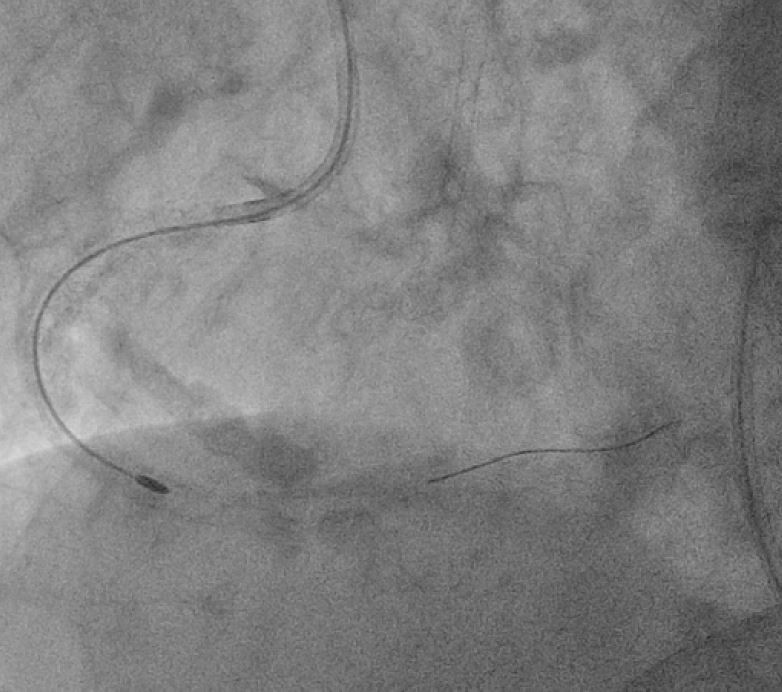
The second coronary intervention was arranged. Coronary angiography showed pattent LAD.PCI of RCA CTO was done. Microcatheter with elecalated CTO guidewires were applied. The CTO segment was finally crossed, but microcatheters cannot pass it. We did rotaablation with 1.25mm burr. Then balloon angioplasty with NC balloons and cutting balloon were done. Finally DEB was deployed.Vital signs improved after PCI and ventricualr arrhythmia subsided. The patient recieved TAVI 2 weeks after PCI smoothly.

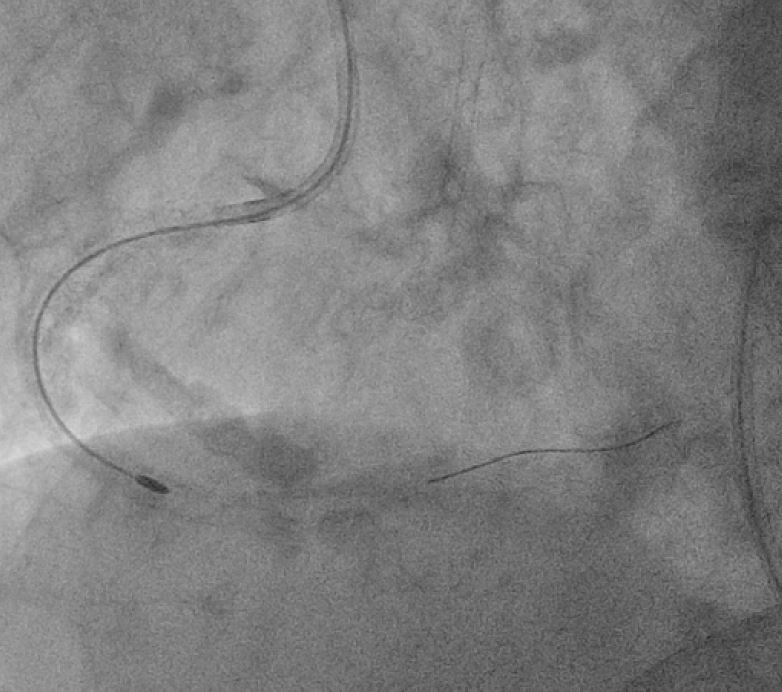

 TAVI final.JPG
TAVI final.JPG
Interventional Management
Procedural Step
Re-attempt PCI for very difficult RCA-M-D occlusive ISR was approached with SCR 3.5x7F via right femoral access. The CTO segment could finally be crossed with a Conquest pro 840, as supported by a Caravel, after all UB3, Fielder XT-R, Conquest Pro, 820 failed to go. However, the calcified lesion failed to be crossed with either Caravel, Tornus or Turnpike Gold. With Turnpike Gold in place, a rota-extrasupport wire could be advanced and parked to RCA-PL. Then the lesion was debulked with a 1.25mm burr, running for few times for polishing. After swopping to Sion Blue ES, the lesions were sequentially dilate with a 2x20mm, 2.75x12mm SC, 3x15mm NC, 3x10mm cutting for up to 18-20 bars. The RCA-P was further dilated with a 3.25x15mm NC BC, inflated up to 20 bars. The RCA-M-D and RCA-P-M lesions were finalized with a 3x40mm and a 3x40mm BB DEB, inflated up to 8 and 12 bars for 60 seconds both. 30% residual stenosis at RCA-P and RCA-M. Very good final flow. Course protracted due to difficult procedure but no complication happened.


Case Summary
The patient with complicated coronary artery disease and valvular heart disease of severe aortic stenosis encountering shock and even collapse with ventricular arrhythmia, which might be triggered by ACS and infection in the admission. It was hard but crucial to determine the priority of intervention to maximize the benefit and reduce procedural risk.
Initially the laboratory data showed elevated cardiac biomarkers and coronary angiography showed the only remaining vessel of LAD with stenosis, therefore we managed it. Then we did balloon valvuloplasty for severe aortic stenosis. Because electrical storm developed even after above intervention, we decided to manage the difficult RCA CTO lesion.
Initially the laboratory data showed elevated cardiac biomarkers and coronary angiography showed the only remaining vessel of LAD with stenosis, therefore we managed it. Then we did balloon valvuloplasty for severe aortic stenosis. Because electrical storm developed even after above intervention, we decided to manage the difficult RCA CTO lesion.