
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-164
Navigating Challenges: Managing Radial Artery Perforation During Percutaneous Coronary Intervention
By Chanikarn Kanaderm
Presenter
Chanikarn Kanaderm
Authors
Chanikarn Kanaderm1
Affiliation
Central Chest Institute of Thailand, Thailand1,
View Study Report
TCTAP C-164
Coronary - Complication Management
Navigating Challenges: Managing Radial Artery Perforation During Percutaneous Coronary Intervention
Chanikarn Kanaderm1
Central Chest Institute of Thailand, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
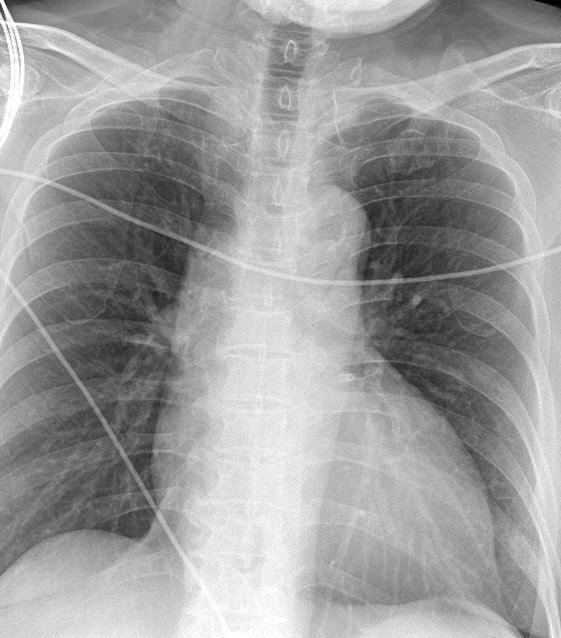
History Chief Complaint: 58 year old male presented with acute chest pain for 3 hours, radiating tothe left arm, associated with mild shortness of breath. No syncope orpalpitations.Past Medical History: Hypertension for 15 years, well-controlled withamlodipine and losartan.Dyslipidemia on rosuvastatin. Physical examination : no significant abnormal finding
Relevant Test Results Prior to Catheterization
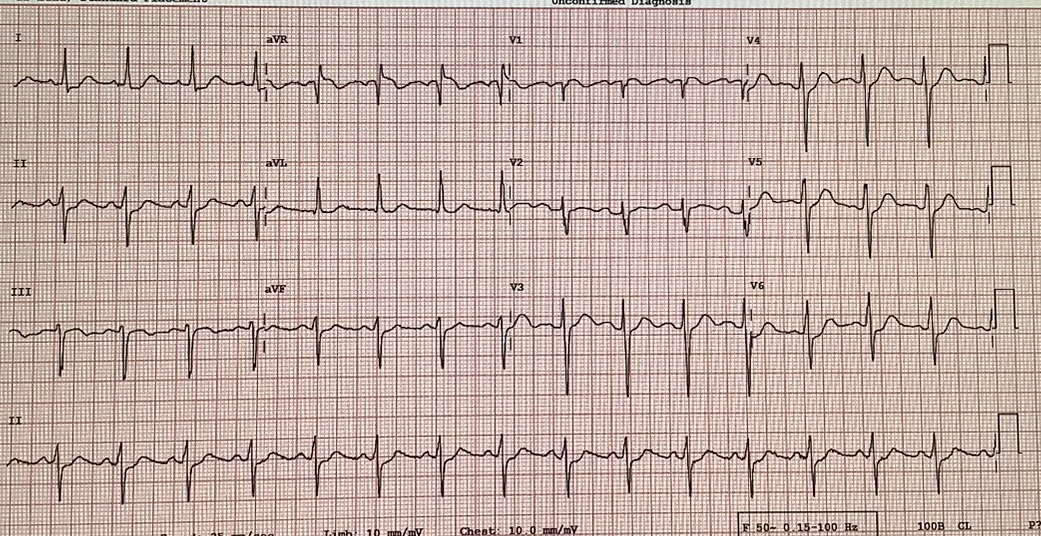
Troponin T: 1.2 ng/mL (positive)
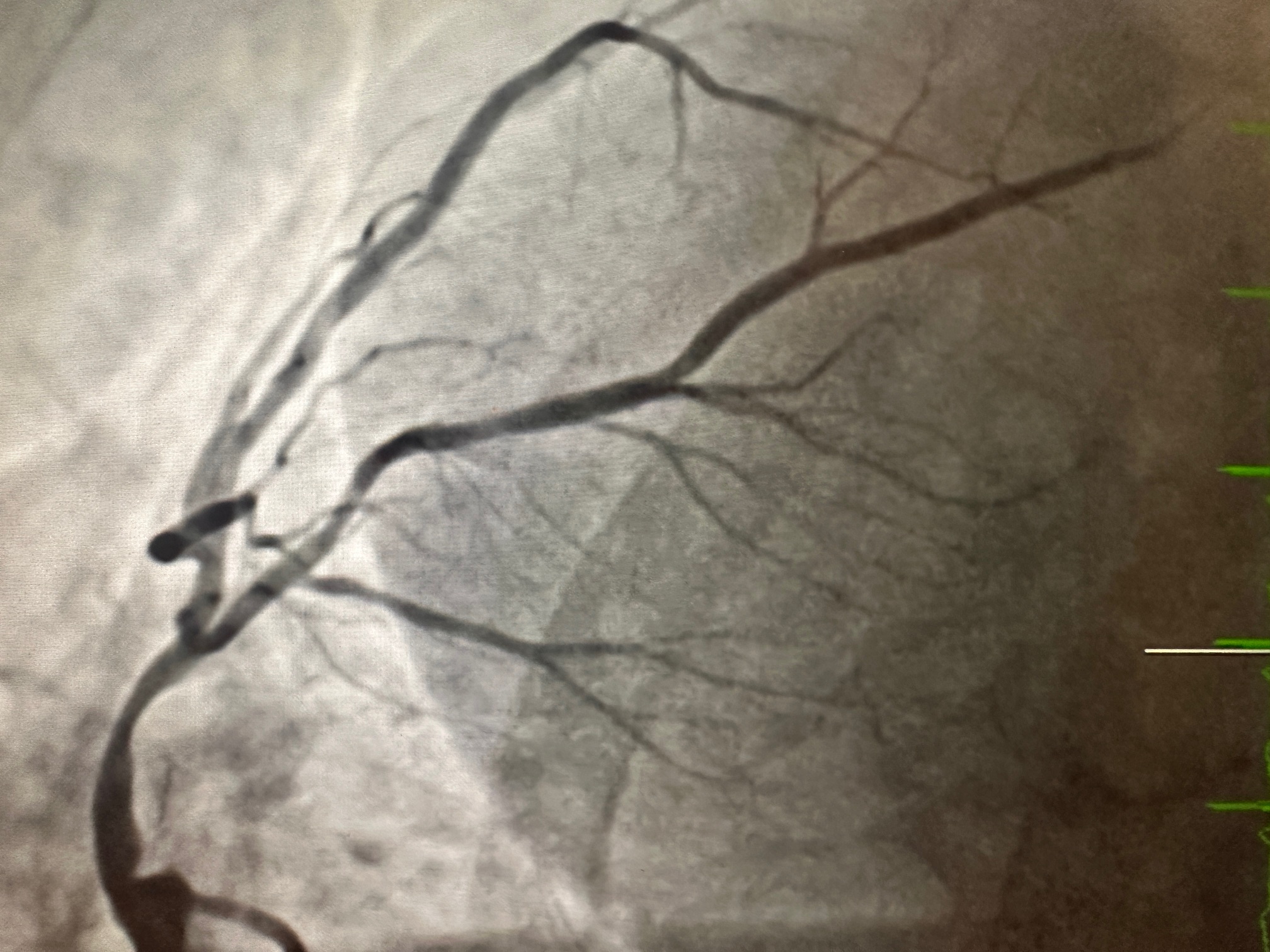
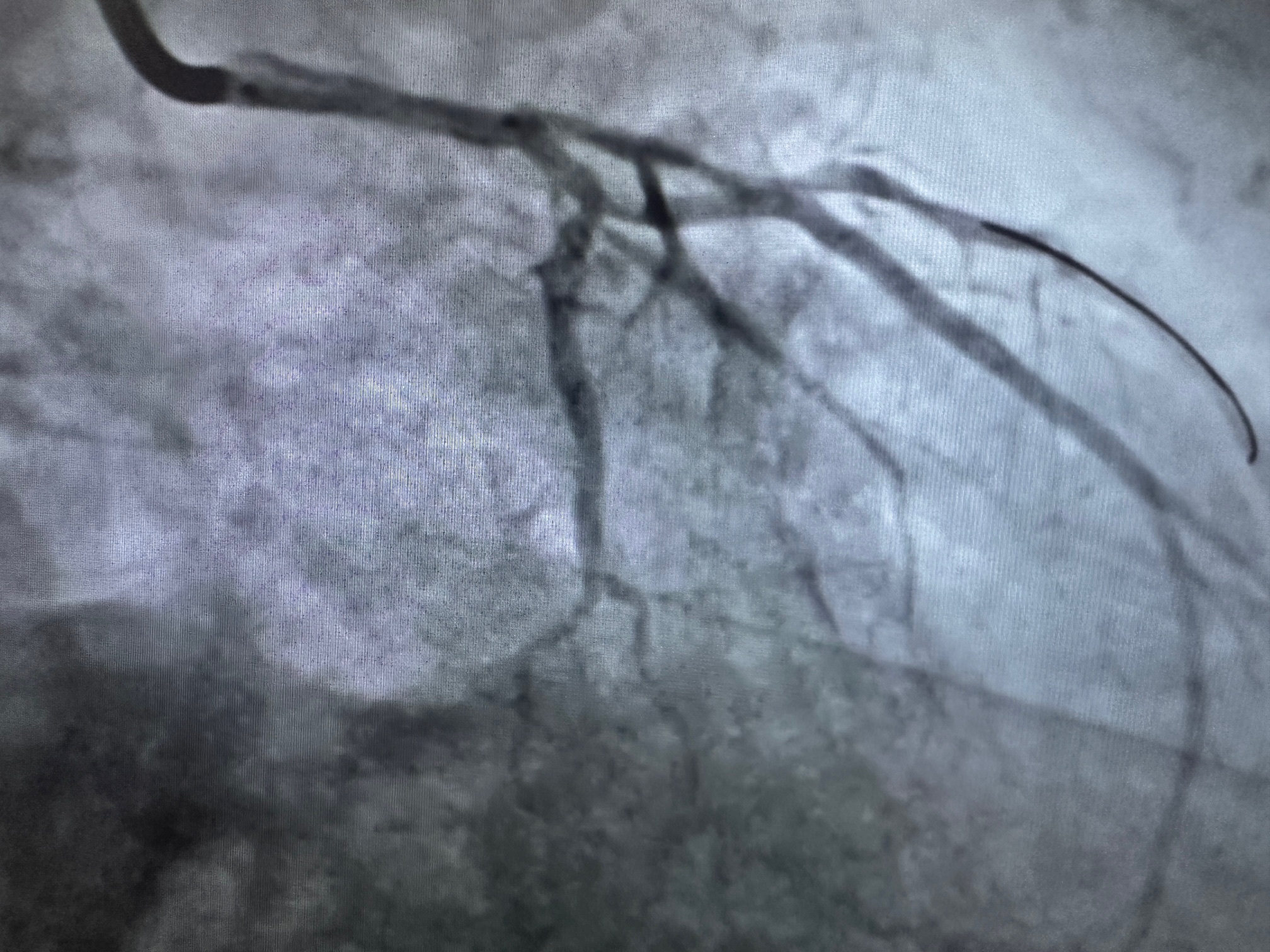
Relevant Catheterization Findings
Coronary Angiography:

Interventional Management
Procedural Step
Procedure: Ad hoc PCI to LM-proximal LAD.

- Guiding Catheter: JL Launcher via the right radial artery.
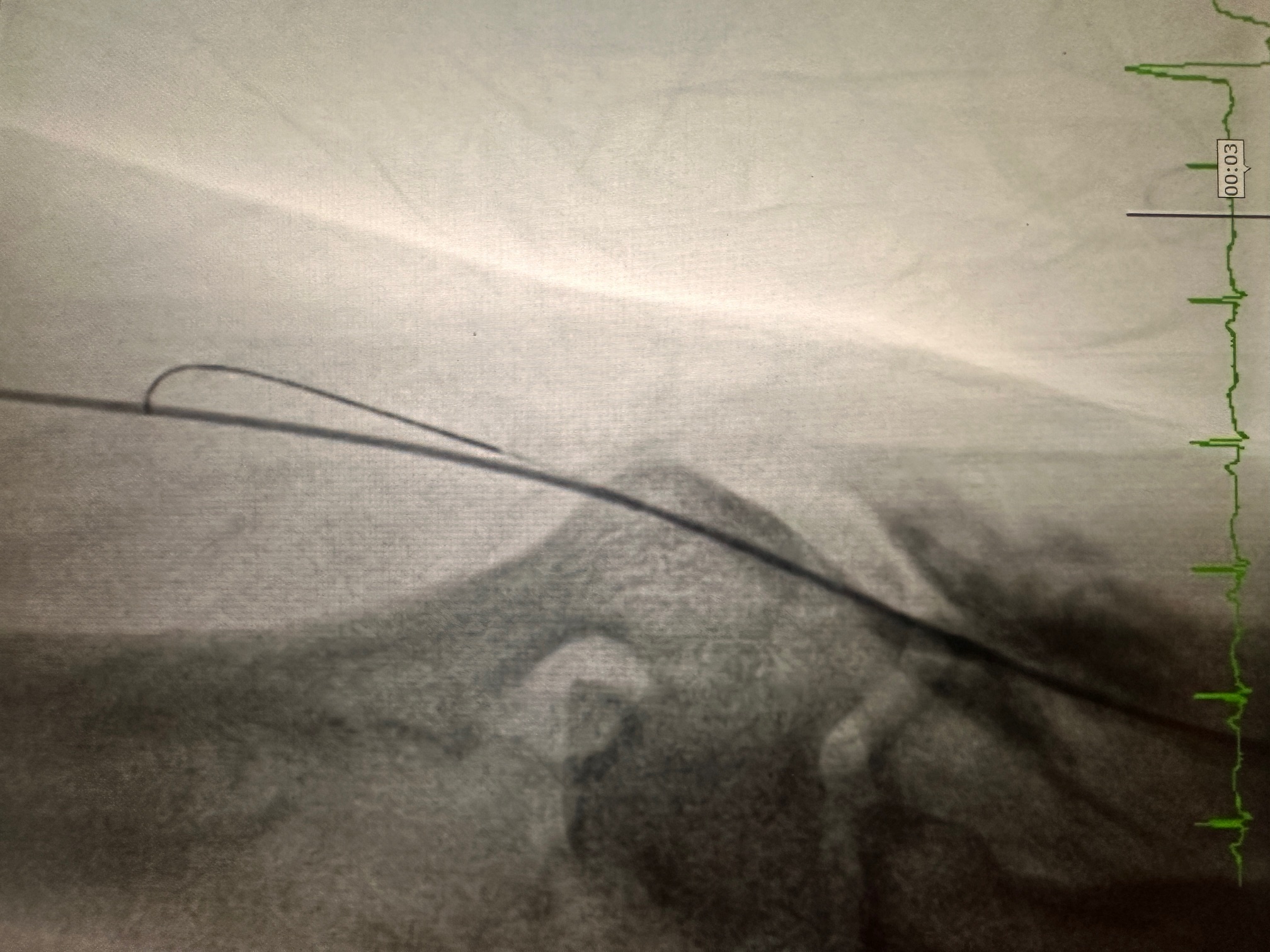
- Complication: Radial artery perforation during catheter insertion.
- Confirmed by contrast extravasation on angiography.
- Small hematoma formation observed at the perforation site.
- Management of Radial Perforation:
- Wire Navigation:
- Advanced a 0.035-inch guidewire into the aorta through the perforated radial artery.
- Introduced a 0.014-inch coronary wire alongside the 0.035-inch wire to maintain distal radial and aortic access for stabilization.
- Balloon-Assisted Technique:
- Positioned a 2.0 mm semi-compliant balloon at the edge of the guiding catheter within the radial artery.
- Inflated the balloon slightly to dilate the perforated segment, facilitating the guiding catheter's smooth passage through the radial artery into the ascending aorta.
- The technique minimized trauma while maintaining radial flow.
- PCI:
- LM-Proximal LAD lesion treated with a drug-eluting stent (DES), achieving TIMI 3 flow post-PCI.
- No further procedural complications.
- Post-Procedural Vascular Management:
- Radial artery flow preserved post-PCI.
- Mild swelling in the right arm managed with a compression dressing, arm elevation, and analgesics as needed.
- Wire Navigation:
Case Summary
The combination of dual-wire technique (0.035 and 0.014) and balloon-assisted catheter advancement offers an effective solution for managing radial artery perforation during PCI. This approach ensures procedural success while preserving vascular integrity, allowing completion of the intervention without switching access sites or compromising outcomes.