
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-207
Triple Trouble in a Complex TAVI
By Debdatta Bhattacharyya, Manik Chopra
Presenter
Debdatta Bhattacharyya
Authors
Debdatta Bhattacharyya1, Manik Chopra2
Affiliation
Narayana Hospital RN Tagore Hospital, India1, Narayana Multispeciality Hospital, India2,
View Study Report
TCTAP C-207
Structural - Aortic Valve Intervention - Coronary Artery Protection / Access
Triple Trouble in a Complex TAVI
Debdatta Bhattacharyya1, Manik Chopra2
Narayana Hospital RN Tagore Hospital, India1, Narayana Multispeciality Hospital, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 75 years old frail, diabetic, hypertensive lady presented to outpatient department with history of recurrent syncope, shortness of breath on exertion. Her vital parameters were within normal limits, while on cardiovascular examination, she had Grade 4/6 ejection systolic murmur in aortic area radiating to the apex and bilateral carotids.
Relevant Test Results Prior to Catheterization
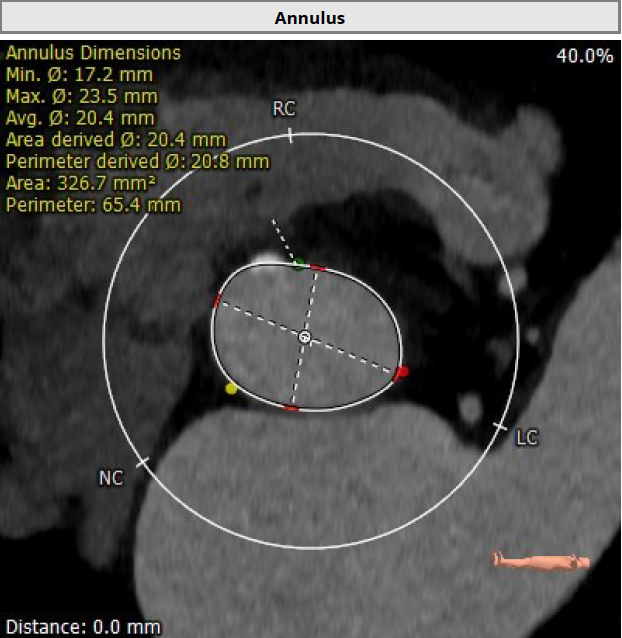
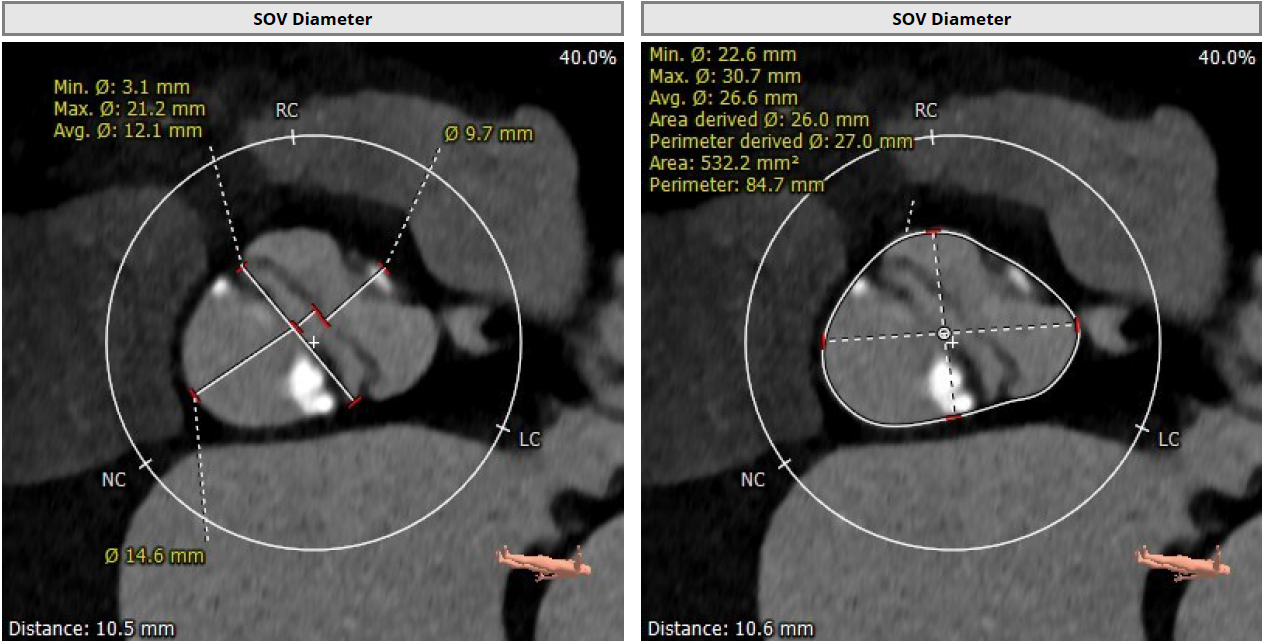
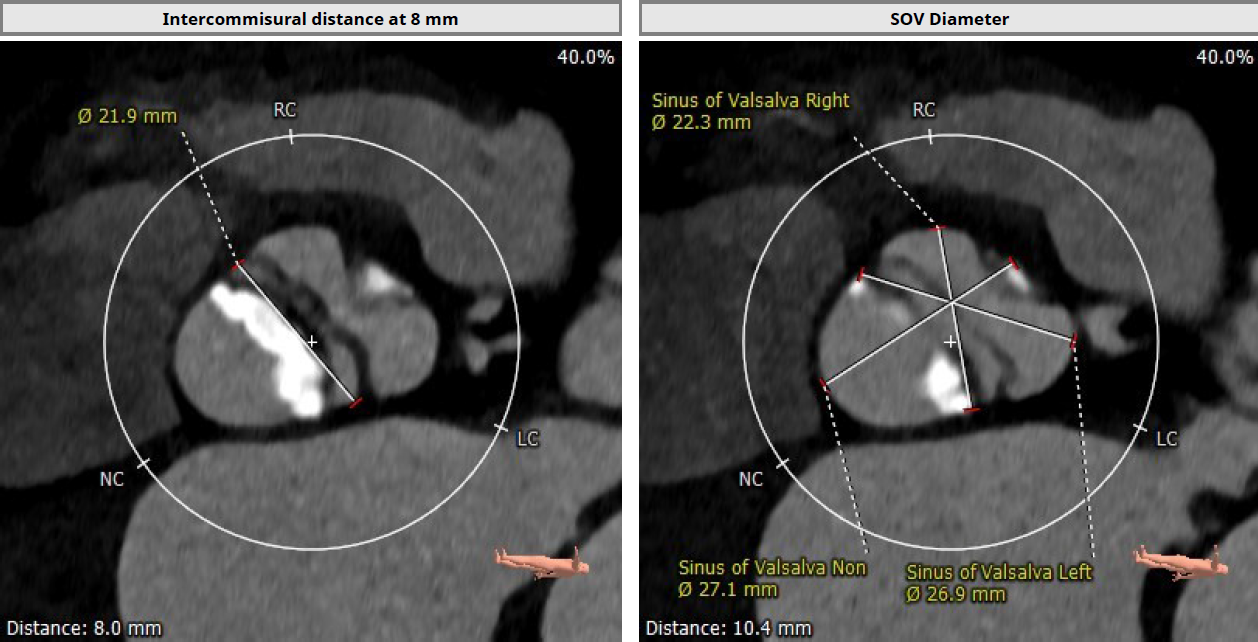
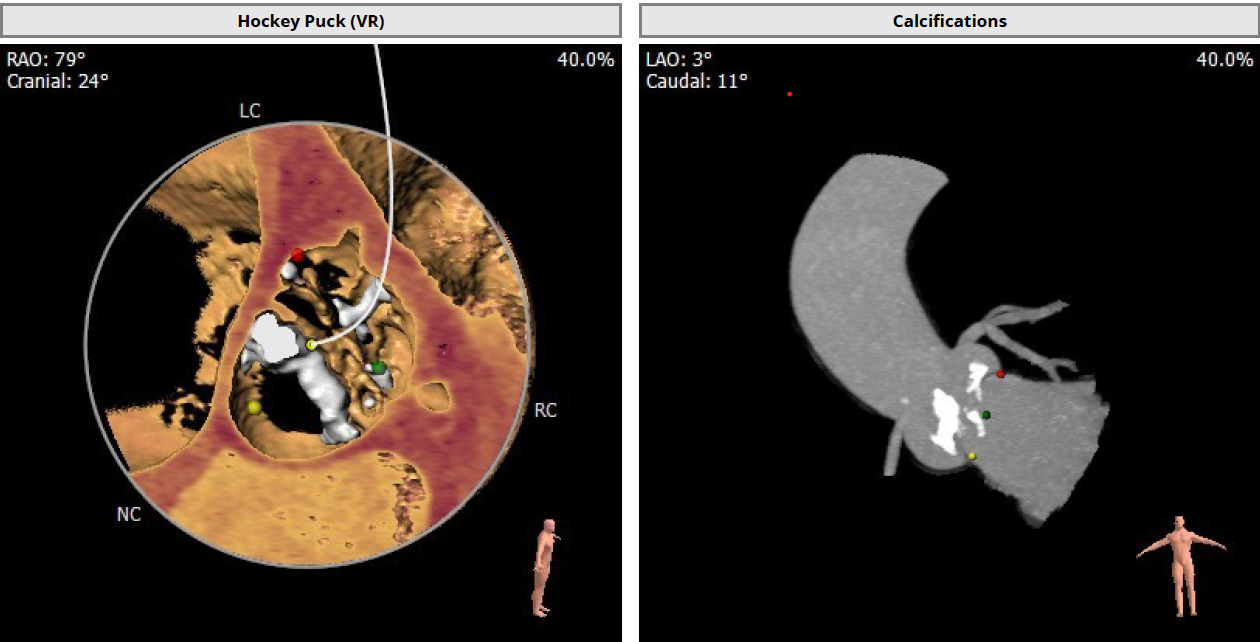
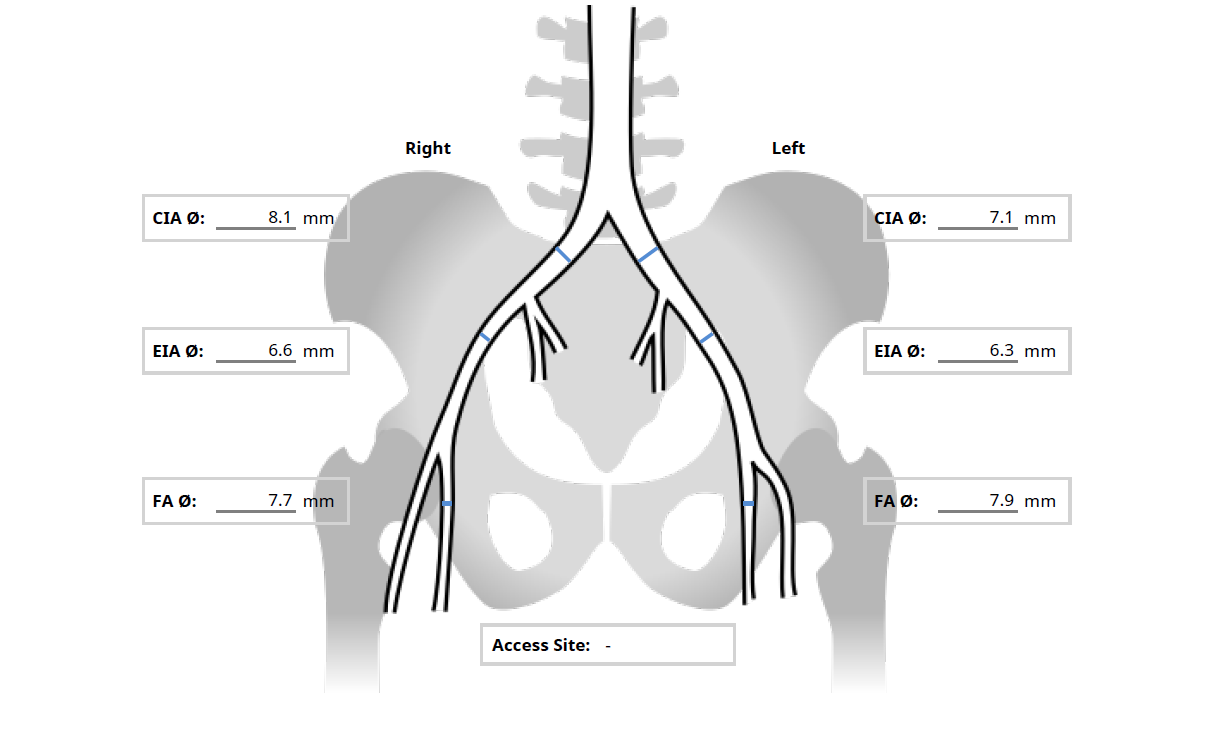
Her echocardiography revealed severe aortic stenosis with mean aortic gradient of 57mmHG along with mild AR. Her LV ejection was normal, other valves were within normal limits. A CT angiogram with 3mensio analysis showed Type 1a Bicuspid aortic valve with calcified raphe and low coronary heights (9mm for RCA, 8mm for LAD). Her peripheral access was adequate with minimum externer illiac artery diameter of 6.6mm.
Relevant Catheterization Findings
Interventional Management
Procedural Step
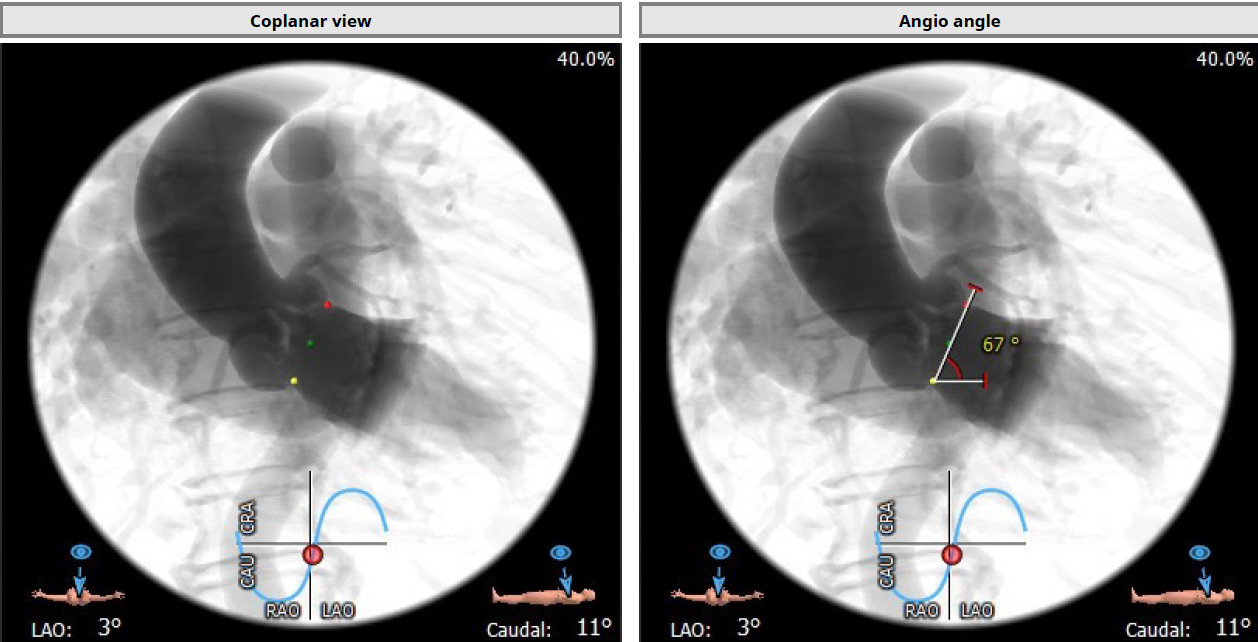
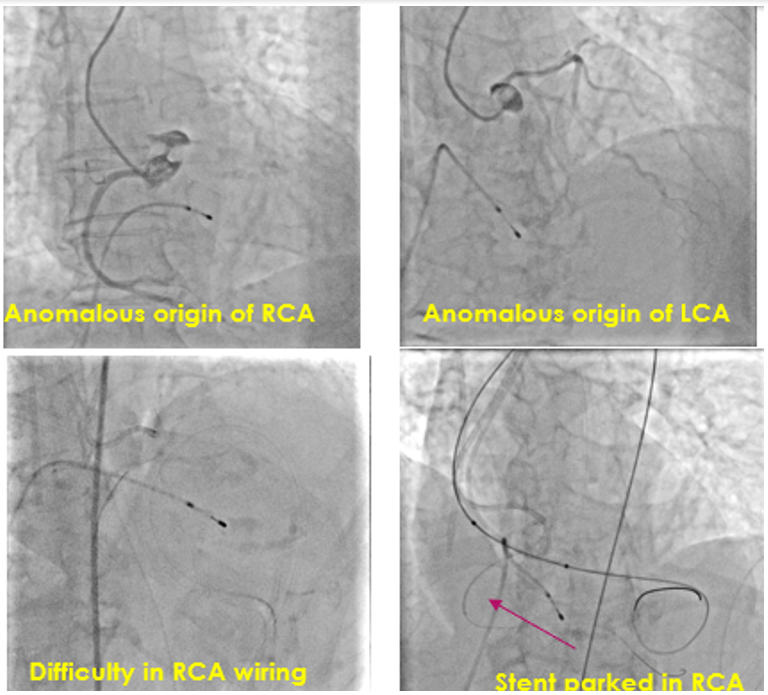
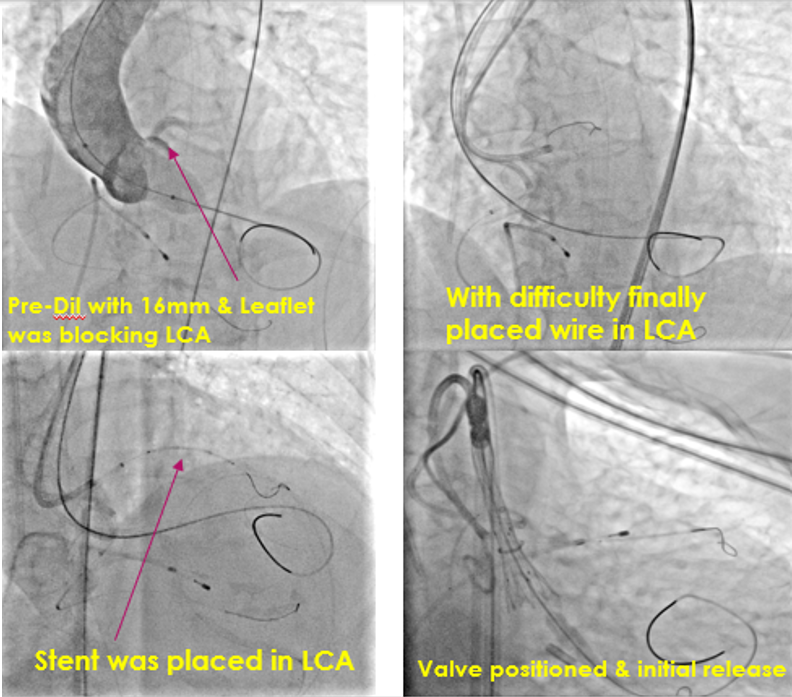
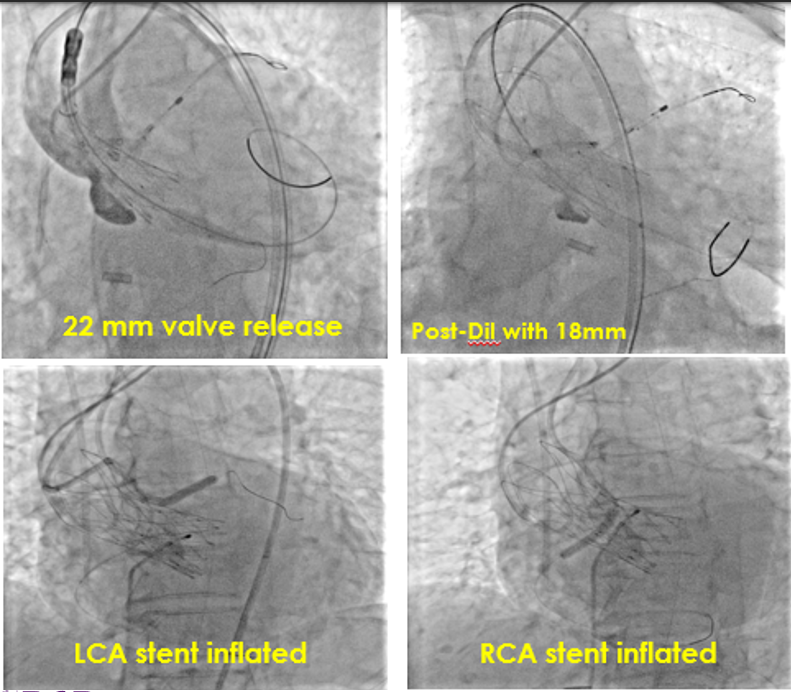
After gaining arterial access through right radial, right and left femoral arteries, selective cannulation of anomalous RCA was done via left femoral arterial route with an amplatz-1 catheter and wired. The left coronary artery could not be cannulated initially via right radial route. the aortic valve was crossed with a straight tipped wire inside an amplatz guide which was exchanged over a pigail catheter witha double curved lunderquist DC wire. Predilatation was done with an 18mm balloon. During the balloon inflationm, it was noted that left coronary artery was at risk of occlusion. After numerous attempts, LCA was selectively engagaed and wired. Thereafter, 26mm Hydra Valve (Self Expanding) under temporary pacing was deployed and the subsequent aortogram showed abscence of paravalvular leakage and threatened occlusion of RCA and LCA ostia due to upright standing native aortic valve leaflets. Chimney stenting was carried out to both left and right coronary ostia to ensure un-interrupted blood flow in the both coronary arteries. At the end of the procedure, patient developed persistent hypotension with swelling in left lower quadrant of abdomen, which was found to bea rectus sheath hematoma on ultrasound. The bleeder was found to be a branch of left inferior epigasstric artery and sealed with glue. Patient required 4 units of blood, followed by an uneventful recovery.
Case Summary
Bicuspid AV (Type 1a) with calcified raphe is a difficult subset to tackle while doing TAVR. Bilateral low coronary ostia with abnormal origins of both coronary arteries presented ac second challenge in this case. Spontaneous bleeding in a small branch of inferior epigastric artery that required sealing off with glue was the final sting in the tale.