
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-223
A Transcatheter Pulmonary Valve Implantation of the Conduit via Transjugular Access
By Elena Golukhova, Karen Petrosian, Gulamzhan Dadabaev, Baizak Sagymbaev, Aleksei Staferov
Presenter
Aleksei Staferov
Authors
Elena Golukhova1, Karen Petrosian1, Gulamzhan Dadabaev1, Baizak Sagymbaev1, Aleksei Staferov1
Affiliation
Bakulev Scientific Center of Cardiovascular Surgery, Russian Federation1,
View Study Report
TCTAP C-223
Structural - Pulmonic Valve Intervention
A Transcatheter Pulmonary Valve Implantation of the Conduit via Transjugular Access
Elena Golukhova1, Karen Petrosian1, Gulamzhan Dadabaev1, Baizak Sagymbaev1, Aleksei Staferov1
Bakulev Scientific Center of Cardiovascular Surgery, Russian Federation1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
The patient is a 17-year-old male with dextro-transposition of the great arteries and a ventricular septal defect. At one year, he underwent a Rastelli procedure with a 20-mm pulmonary allograft. Six years later, the defunct allograft was replaced with a 25-mm allograft. He has since been on macitentan for pulmonary arterial hypertension. He presented with reduced physical tolerance and fatigue and was deemed a candidate for transcatheter pulmonary valve replacement based on clinical findings.
Relevant Test Results Prior to Catheterization
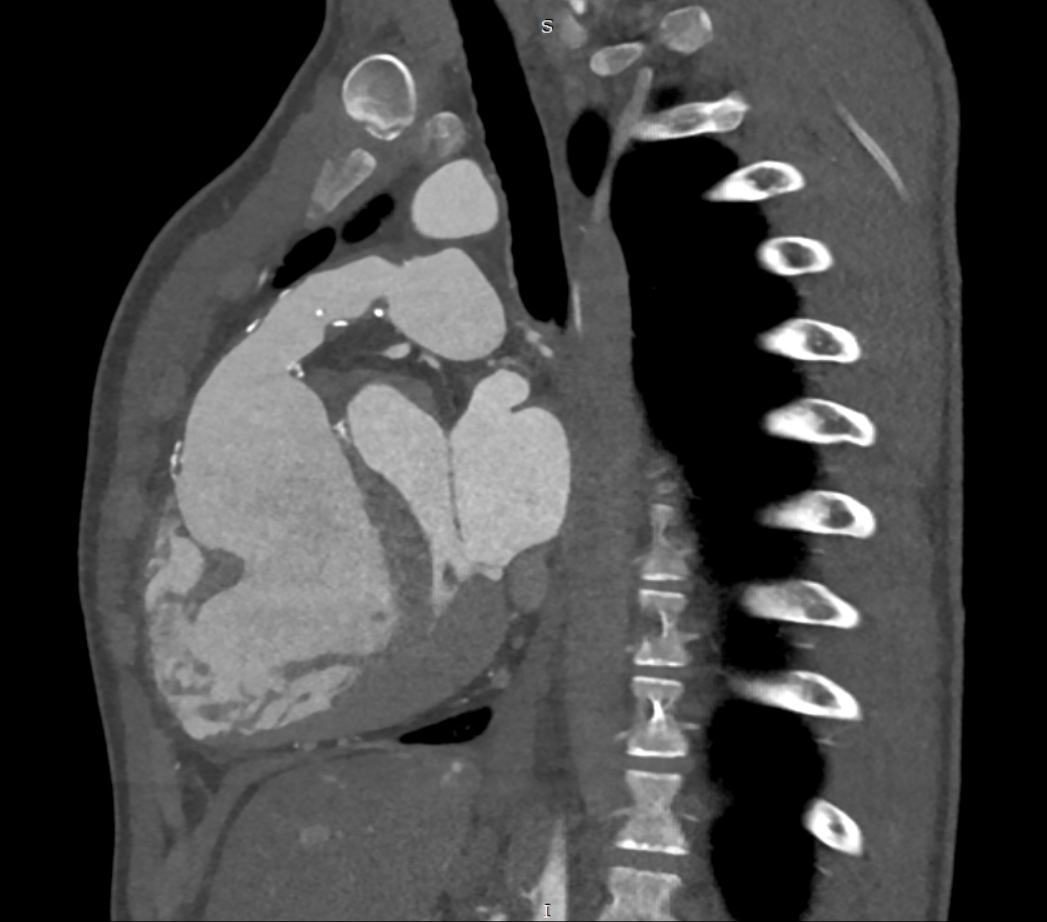
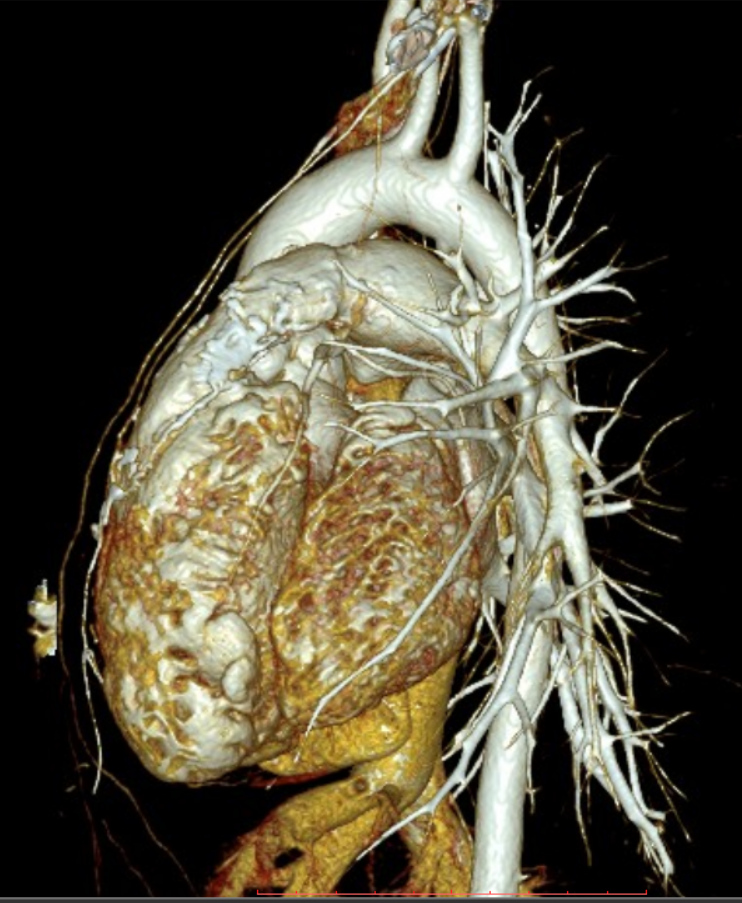
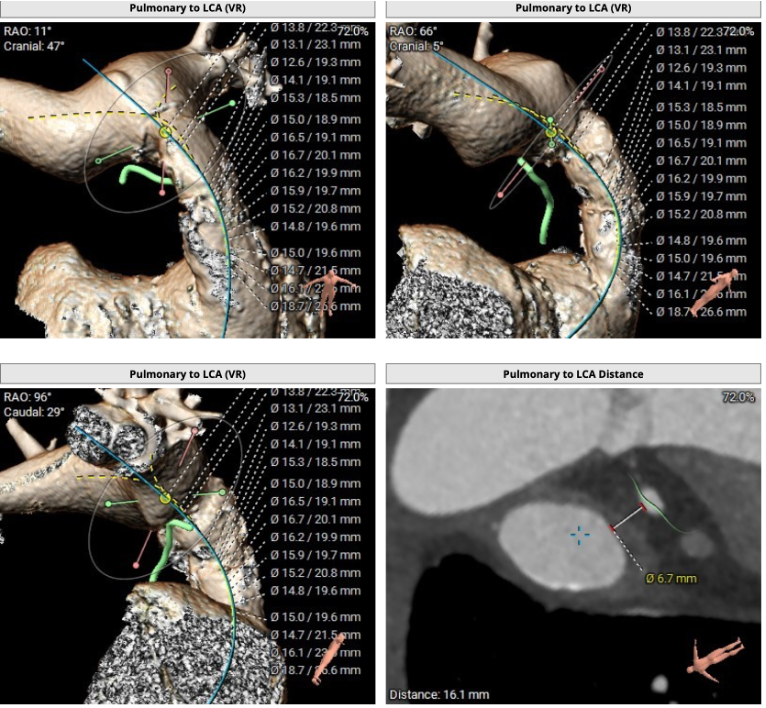
CT scan revealed calcinosis stenosis in the proximal part of the conduit, while echocardiography showed a reduced right ventricular ejection fraction of 35% and a peak gradient at the pulmonary artery of 60-65 mmHg, left ventricular ejection fraction was 59%.
Relevant Catheterization Findings
Invasive pressure measurements indicated pulmonary artery pressure of 36/20/21 mmHg. at an arterial pressure 117/59/74 mmHg. Systolic gradient between right ventricle and left atrium - 60 mmHg, right atrial pressure was 11 mmHg.
Interventional Management
Procedural Step
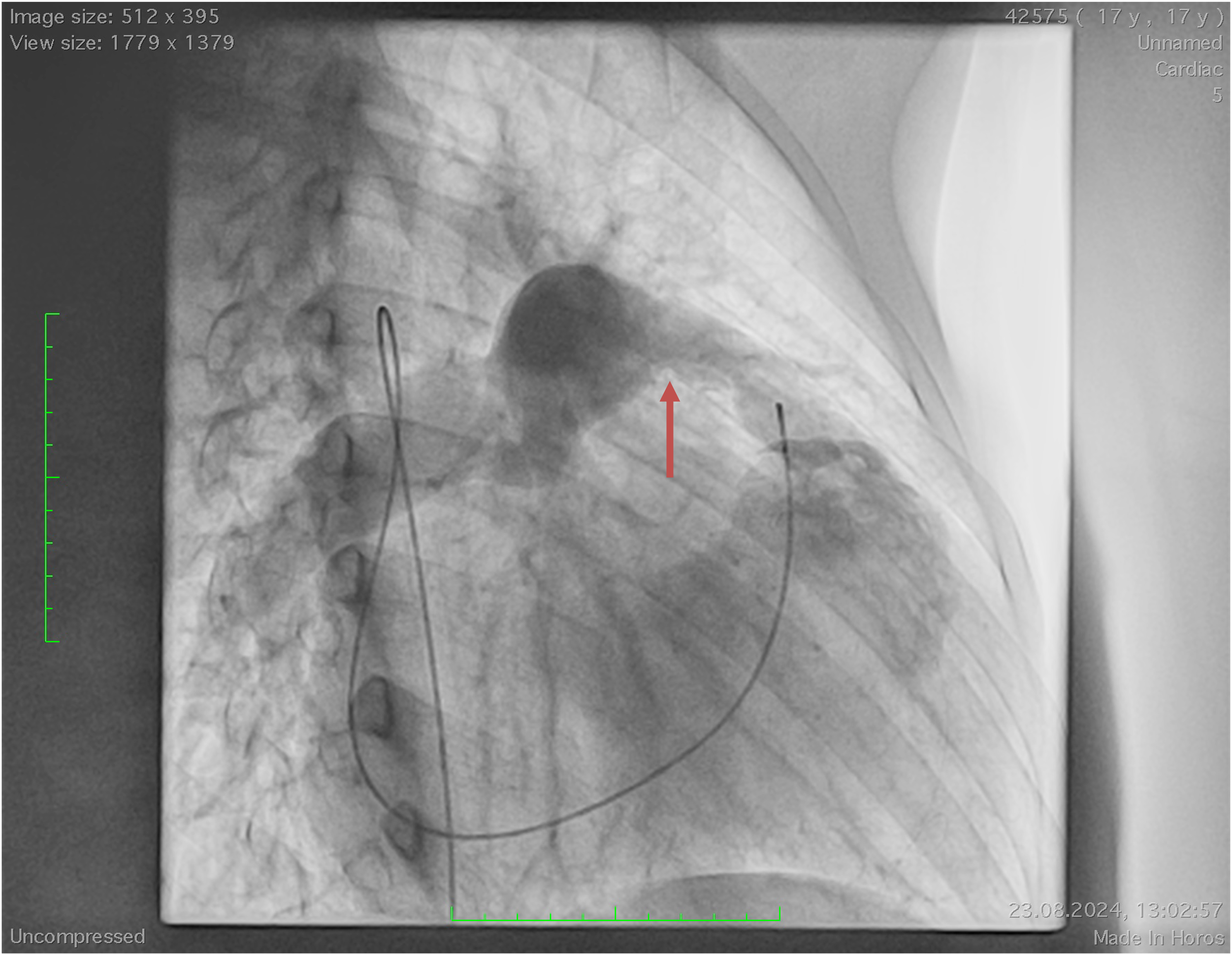
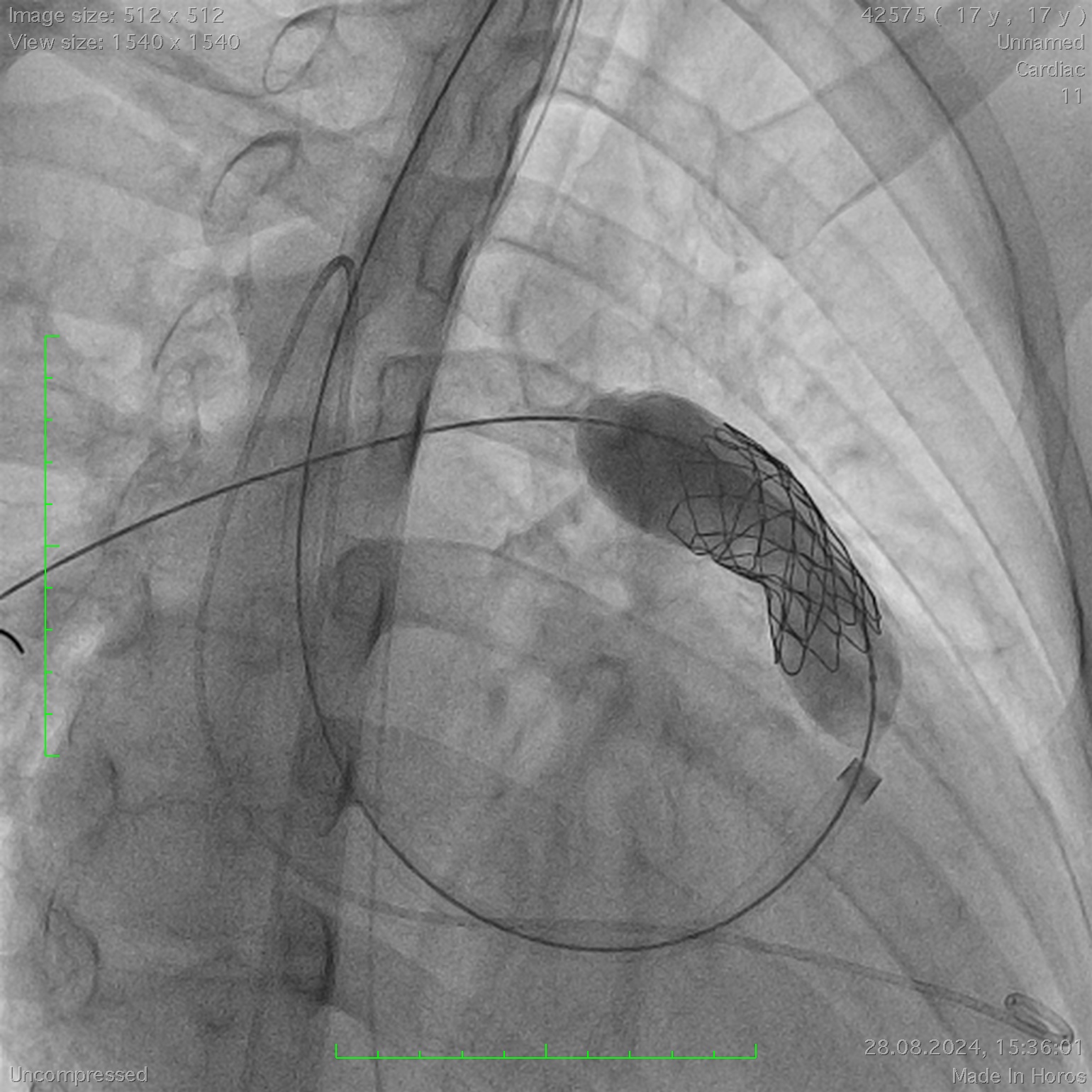
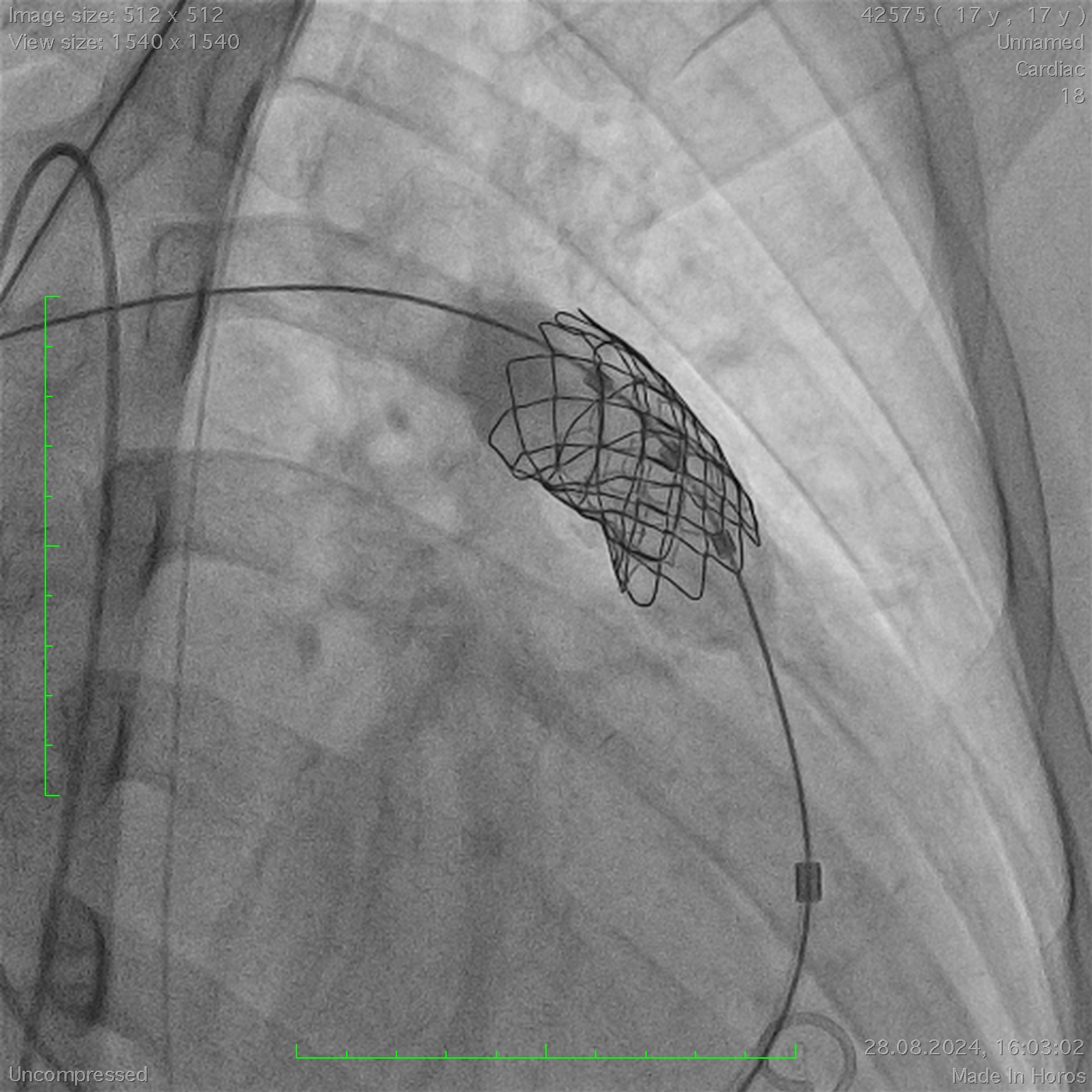
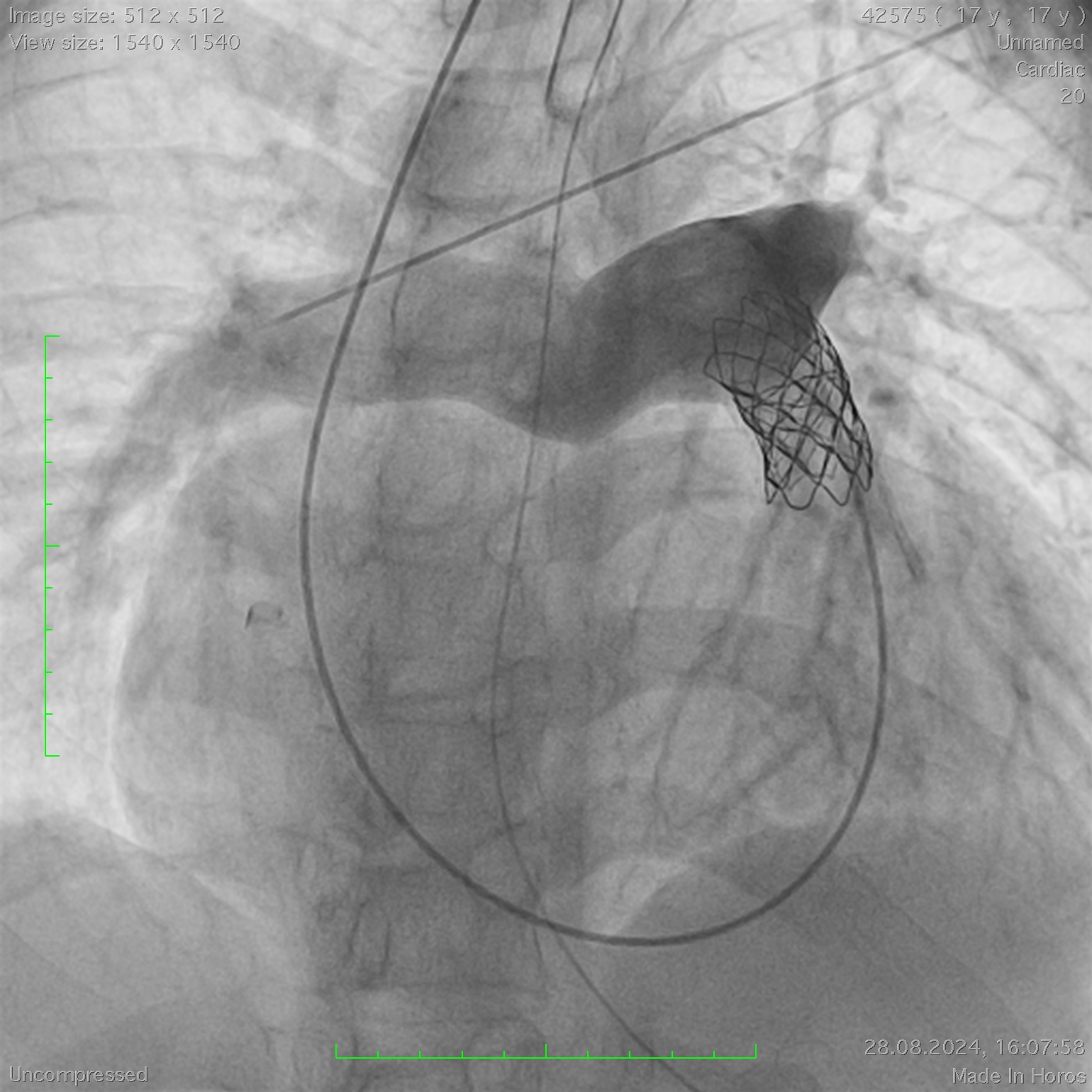
The procedure was performed via transjugular access due to the absence of the hepatic segment of the inferior vena cava, which made the transfemoral approach infeasible. After achieving an activated clotting time (ACT), a Lunderquist guidewire (Cook Medical, USA) was advanced into the right pulmonary artery. Using this guidewire, a 45-80 mm CP Covered Stent (NuMED, USA) was implanted within the conduit using a 20-mm balloon-in-balloon (BiB) catheter (NuMED, USA). Subsequently, a 20-mm Myval valve (Meril Life Sciences, India) mounted on a 20-mm balloon was advanced over the guidewire to the location of the previously implanted stent. After accurate positioning, the valve was deployed within the stent. Ultrasound imaging confirmed the absence of paravalvular leaks, and the gradient across the conduit was measured at 14 mmHg. The patient was discharged on the fifth day in good condition. Follow-up evaluation is recommended in twelve months.
Case Summary
In patients who have undergone the Rastelli procedure for congenital heart disease, conduit dysfunction is a common and significant issue. These patients often require multiple reoperations throughout their lifetime. In this context, stent implantation within the conduit, combined with transcatheter pulmonary valve implantation (TPVI), represents a safe, minimally invasive, and efficient alternative to open-heart surgery. This approach reduces surgical risks, shortens recovery times, improves long-term outcomes, and enhances the patient’s overall quality of life, making it a valuable option for managing conduit-related complications.