
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-198
The Wrong Way Is Right! - A Total Occlusion Lesion Caused by Stent at False Lumen
By Wei-Cheng Chang
Presenter
Wei-Cheng Chang
Authors
Wei-Cheng Chang1
Affiliation
Tri-Service General Hospital, Taiwan1,
View Study Report
TCTAP C-198
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
The Wrong Way Is Right! - A Total Occlusion Lesion Caused by Stent at False Lumen
Wei-Cheng Chang1
Tri-Service General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
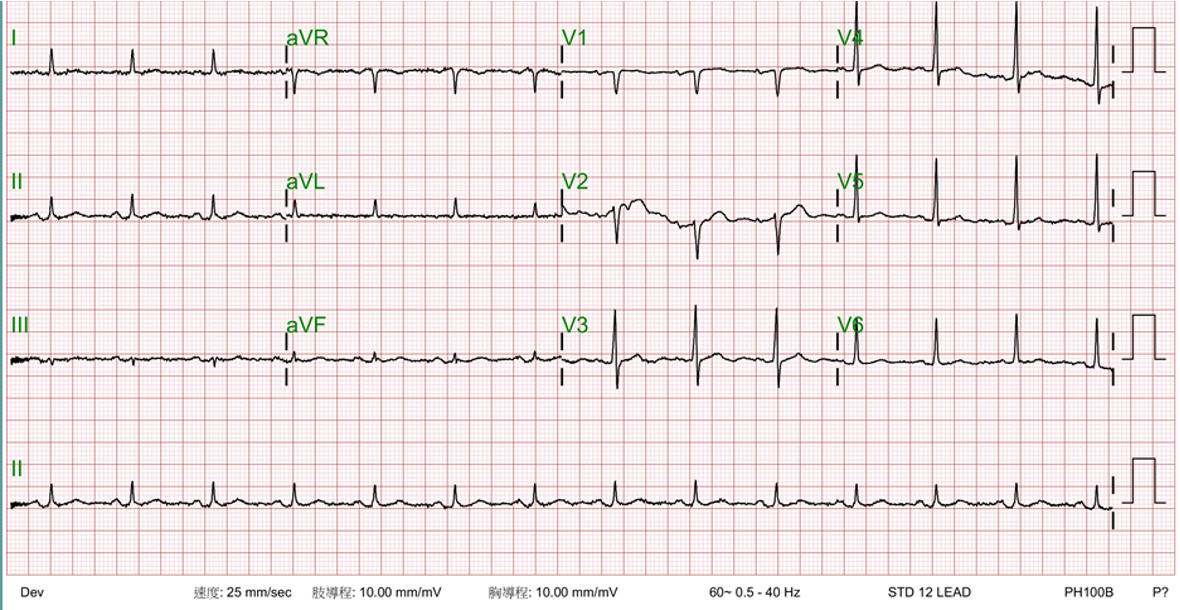
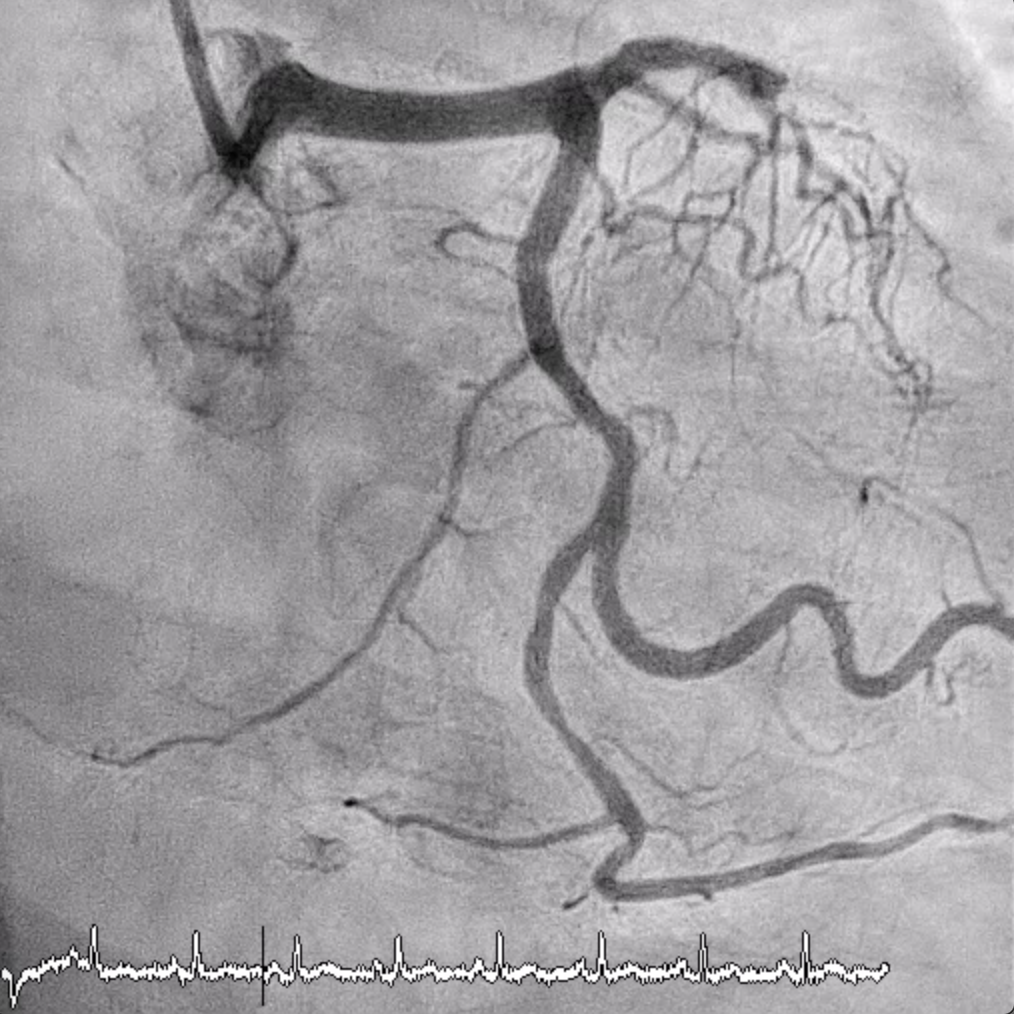
A 69-year-old man with a history of type 2 diabetes, hypertension and type B aorta dissection status post stunting. He had angina and accepted stenting at proximal to middle part of left anterior descending artery coronary due to chronic total occlusion one year ago at other hospital. Few months later, he had progressed angina and went to this cardiovascular out-patient department for further management. Coronary angiography showed type IV in-stent restenosis (total occlusion).

Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
1. LMCA: Luminal irregularity
Interventional Management
Procedural Step
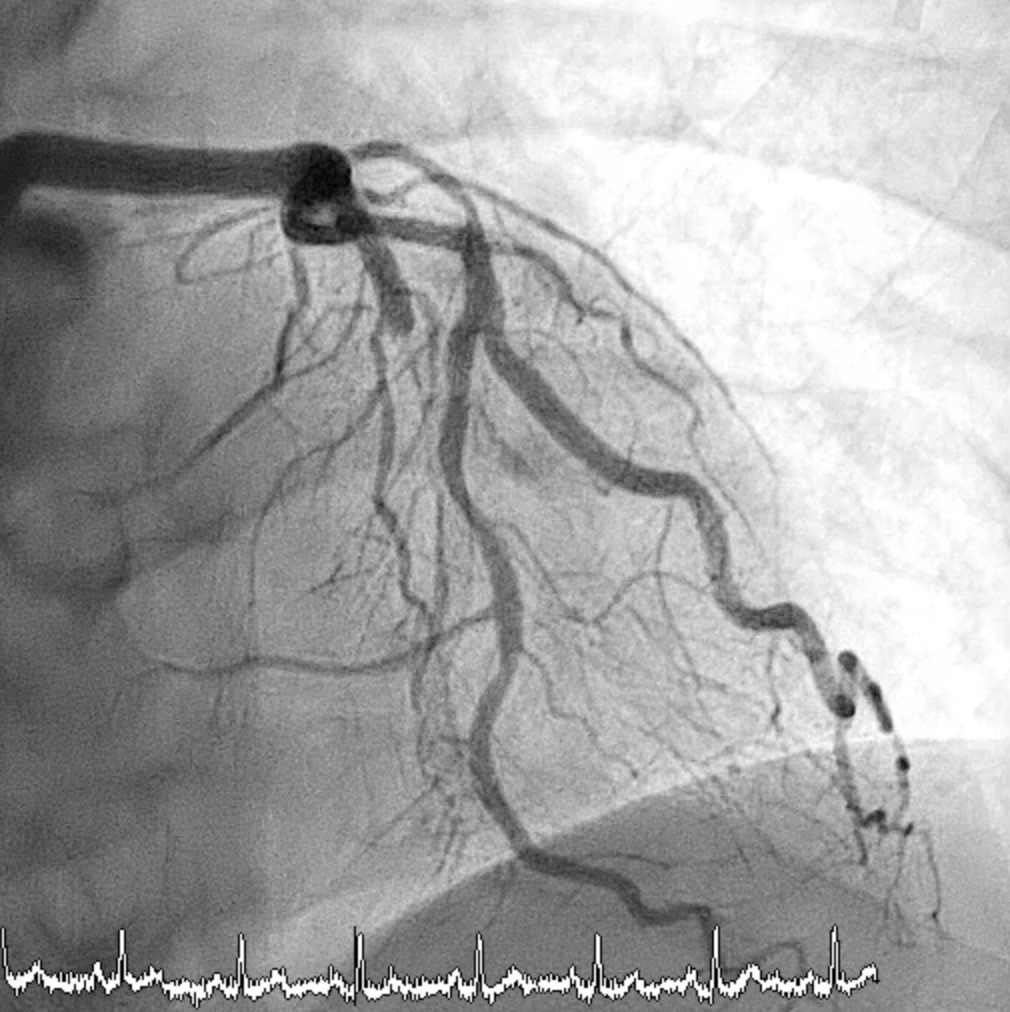
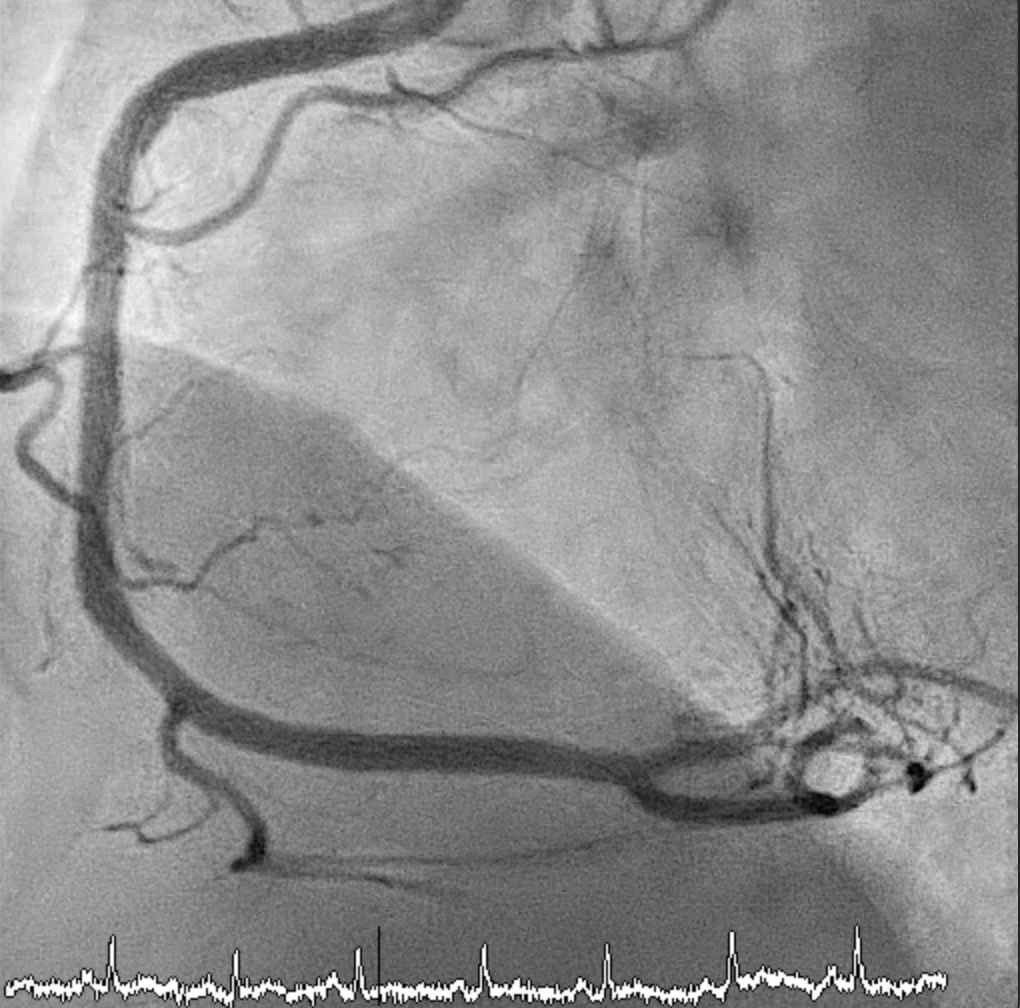
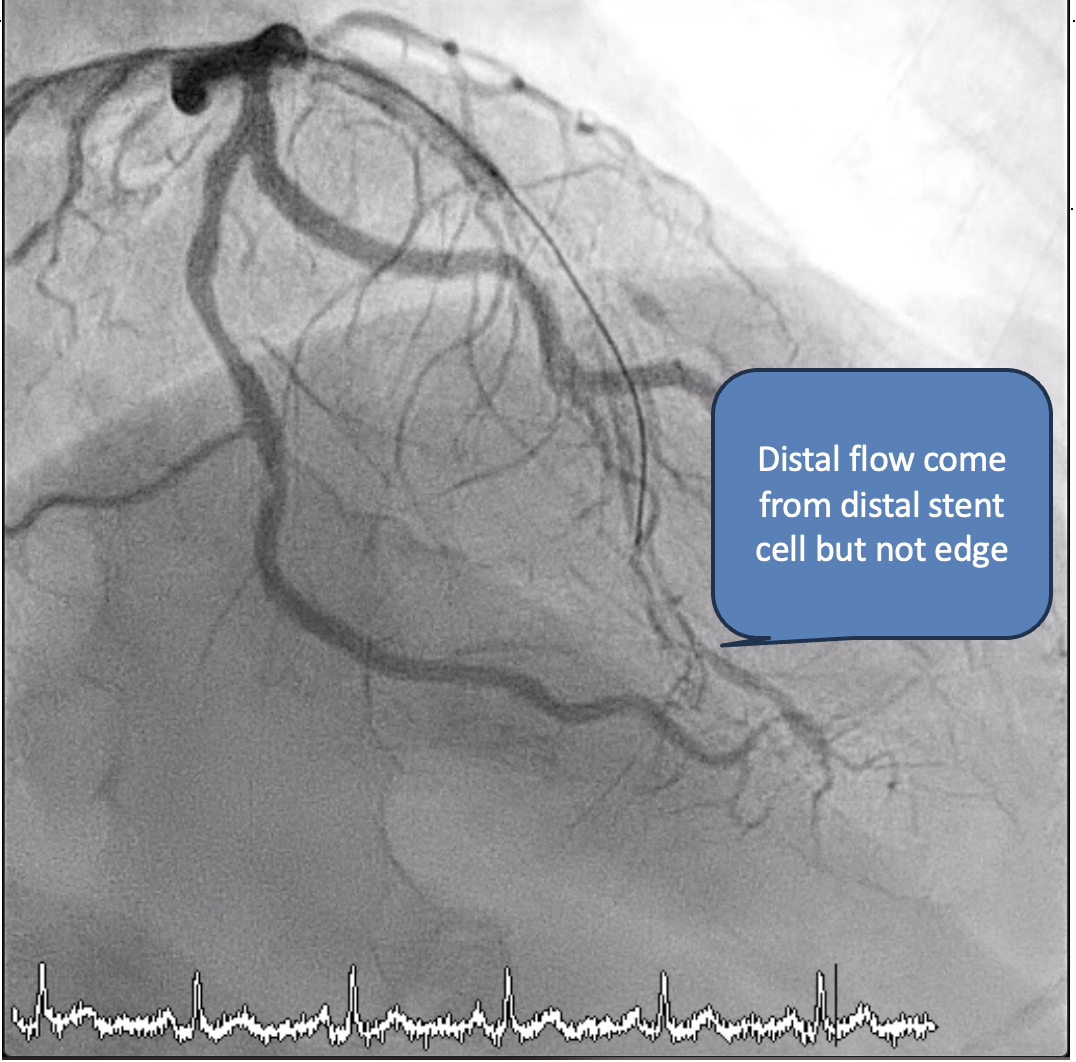
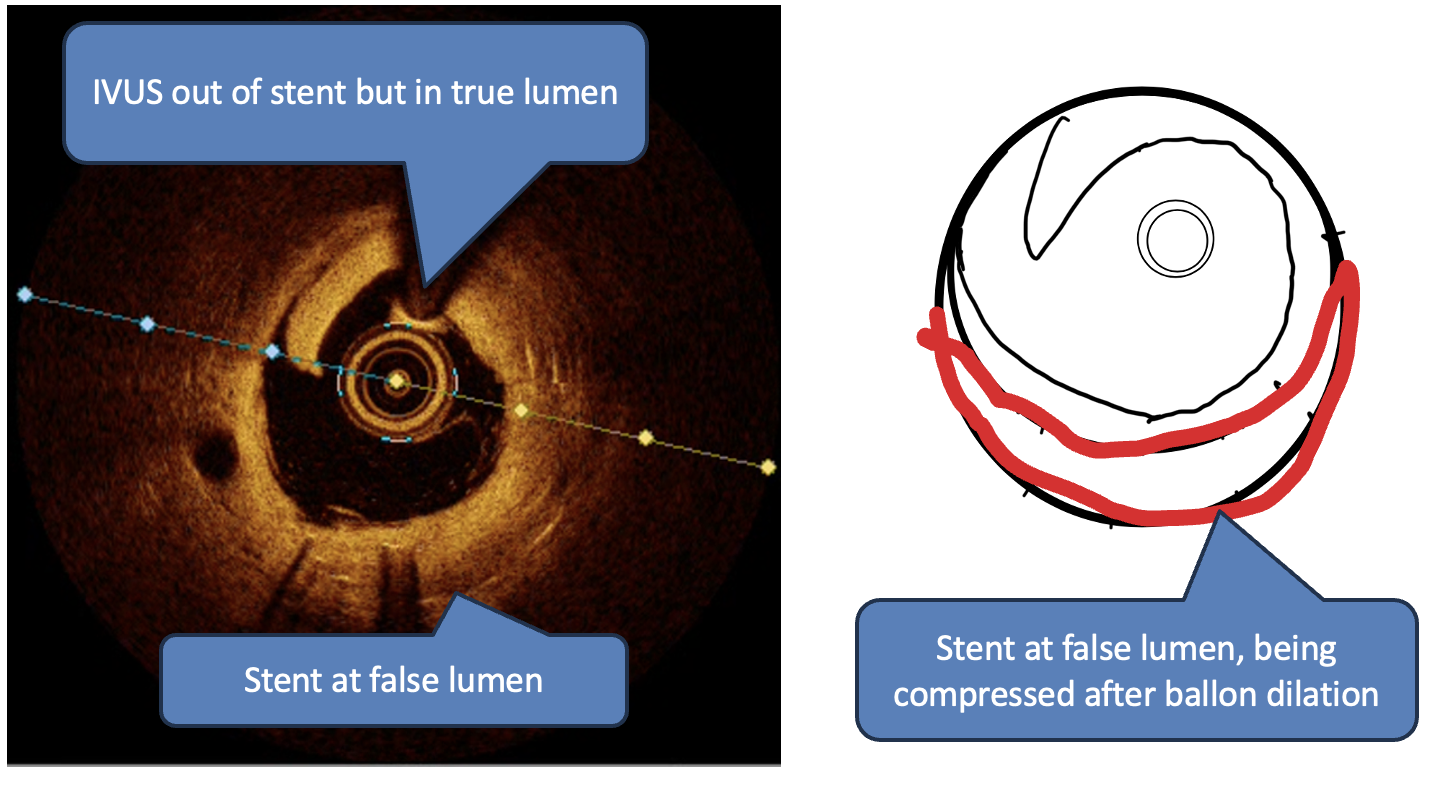
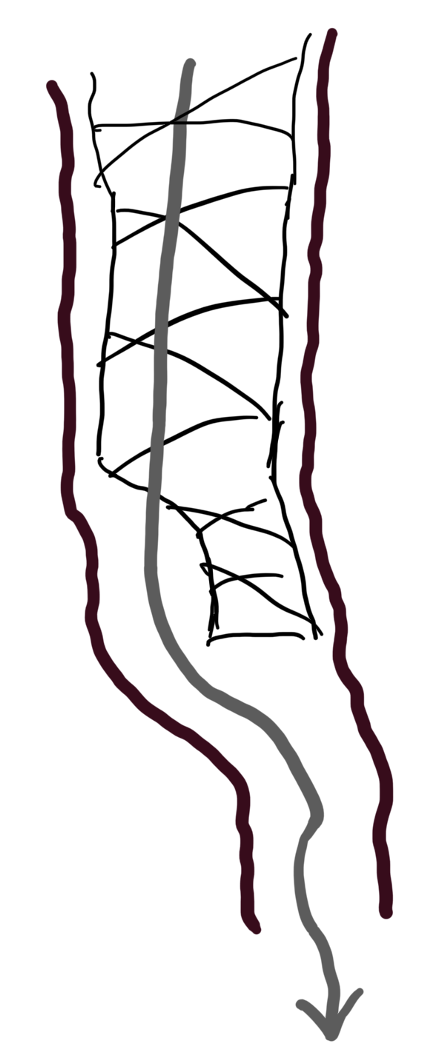
Wires was loaded in microcatheter and crossed proximal to middle total occlusive in-stent restenosis lesion but failed to cross the CTO cap just at distal sent edge. After several attempts. Following angiography showed faint flow pass through the distal stent edge to distal LAD. But the flow seems not to cross the distal stent edge. Escalated wire to conquest Pro 12 with microcatheter and puncture the distal stent cell. The wire finally went into the possible true lumen, after balloon dilation and checked by the IVUS. It was confirmed that the previous stent distal edge was deployed at false lumen. Then ISR lesion was dilated by NC and DEB. Two years later, CAG showed TIMI 3 flow to distal but recurrent ISR at proximal to middle LAD stent. But no total occlusion at distal stent edge.
Case Summary
Usually, the way of wiring the total occlusion lesion which secondary to in-stent restenosis is let the wire at central of stent. However, our wire can’t cross the distal stent edge. Fortunately, following angiography give us a hint that the stent maybe deployed at false lumen, at we did cross into the true lumen from distal stent cell. And it was confirmed by IVUS. We didn’t stent at distal stent edge but dilated it by drug-eluting balloon only. It showed no total occlusion after two years later.