
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-217
Snip the Leaf - Trans Mitral Valve Replacement With Lampoon
By Anuj Kapadia, Pragathi Gurram, Swaroop Bharadi, Rajeev Menon, Bhishma Chowdary, Uday Kiran Anne
Presenter
Pragathi Gurram
Authors
Anuj Kapadia1, Pragathi Gurram1, Swaroop Bharadi1, Rajeev Menon1, Bhishma Chowdary1, Uday Kiran Anne1
Affiliation
AIG Hospitals, India1,
View Study Report
TCTAP C-217
Structural - Mitral Valve Intervention - Transcatheter MV Replacement
Snip the Leaf - Trans Mitral Valve Replacement With Lampoon
Anuj Kapadia1, Pragathi Gurram1, Swaroop Bharadi1, Rajeev Menon1, Bhishma Chowdary1, Uday Kiran Anne1
AIG Hospitals, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
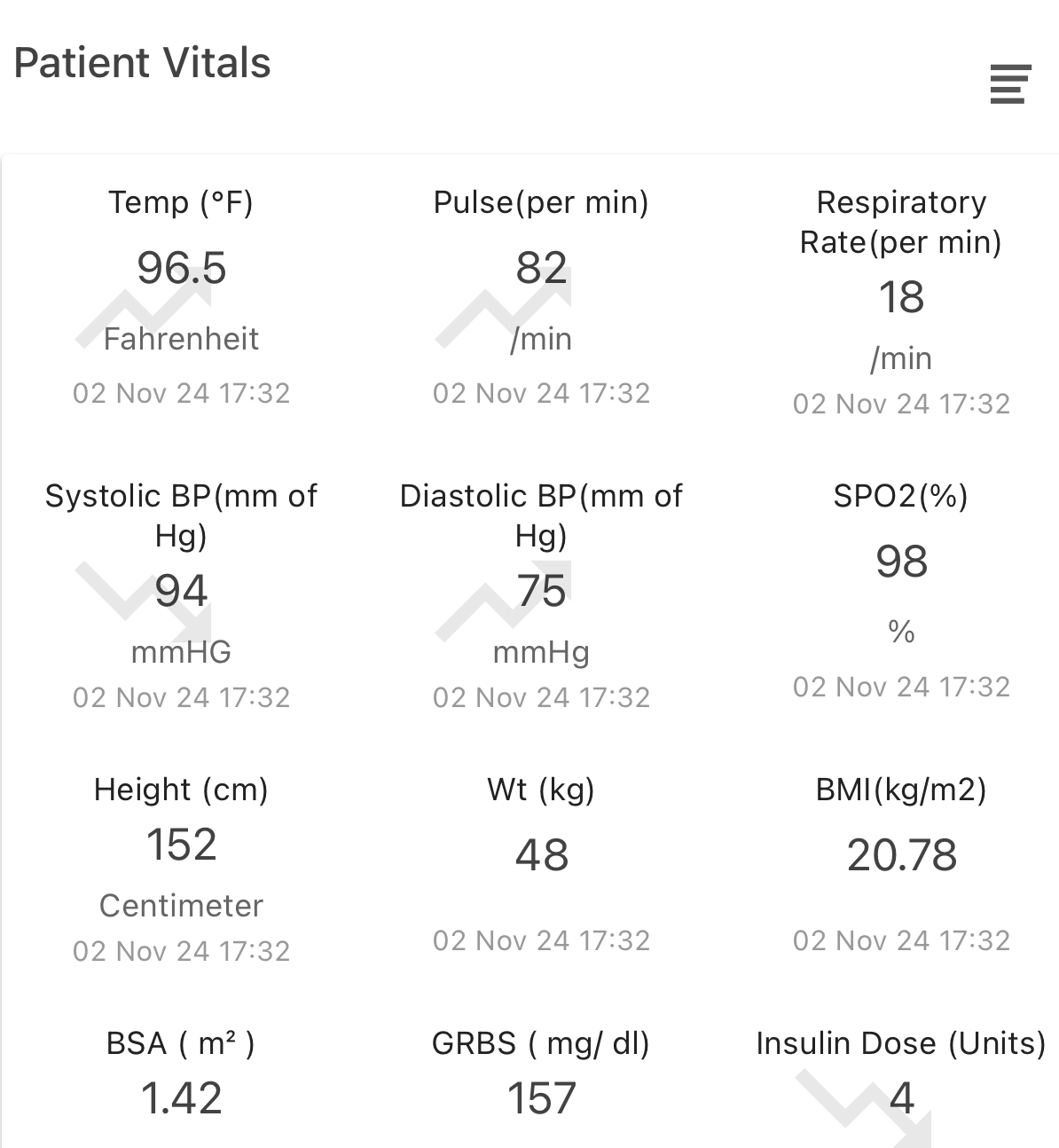
78 Year frail female with background of DM2, hypothyroidism, Right hemiparesis 10 years back, CRHD - severe MS - post closed mitral valvotomy twice, s/p mitral valve replacement (27 mm magna perimount tissue valve) 14 years back. Currently presented with worsening dyspnea, palpitations, recent admission with pulmonary edema. Pulse 102/MIN, BP 140/70 MMHG, JVP mild elevation, first heart sound normal, loud P2, MDM at apex, PSM grade 3/6 at apex, bilateral fine basal crepts.
Relevant Test Results Prior to Catheterization
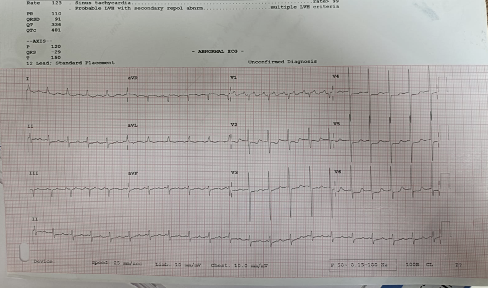
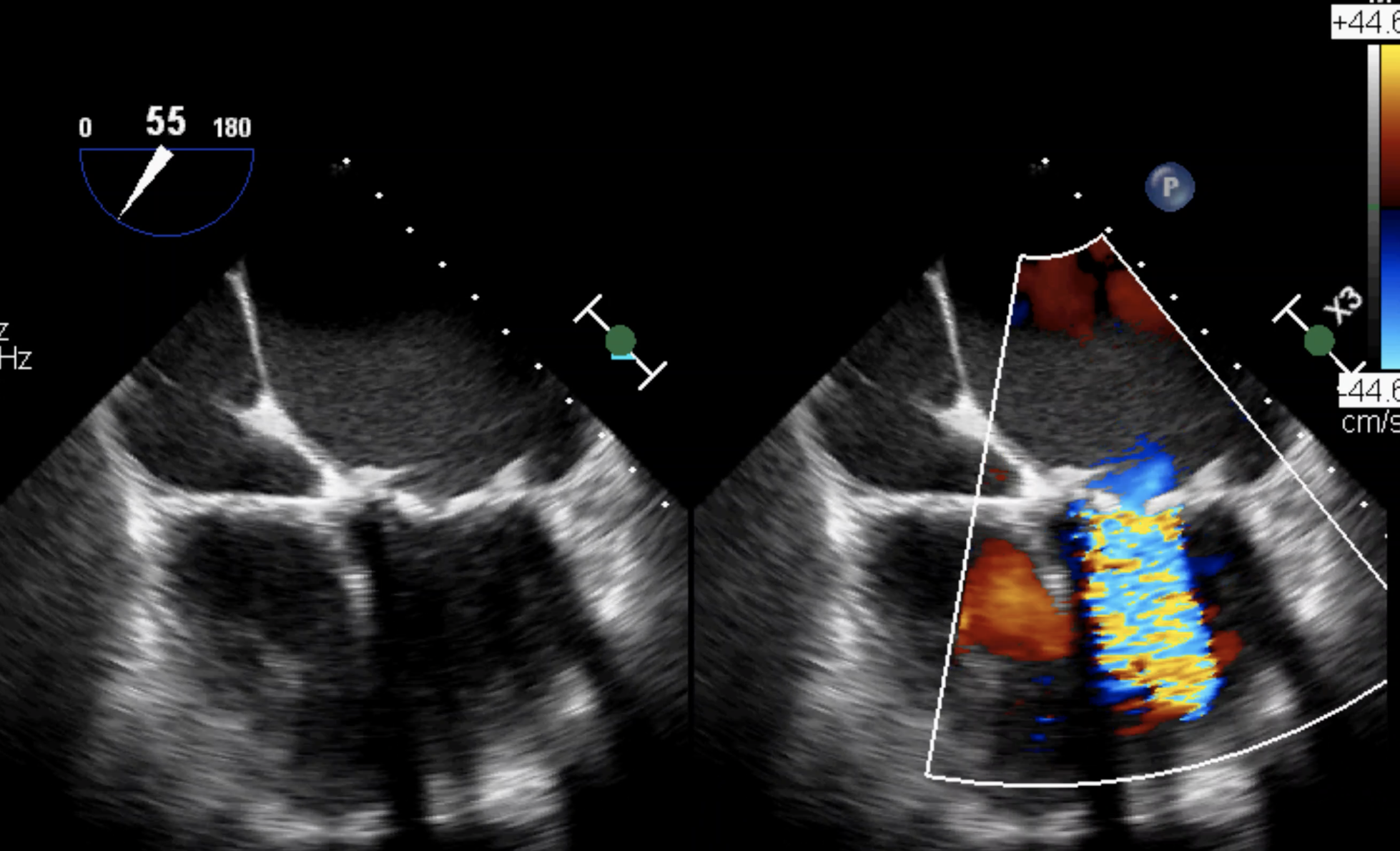
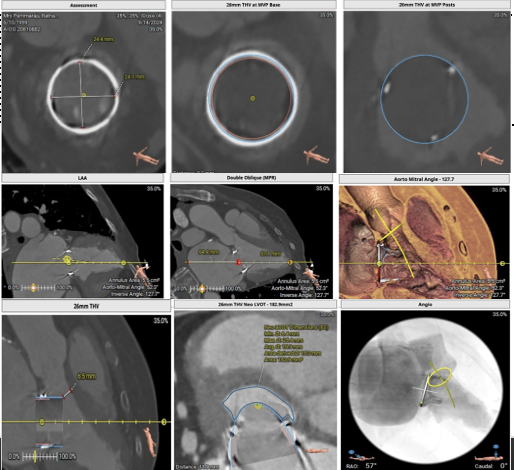
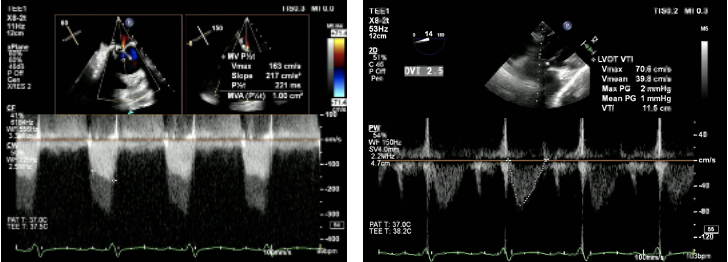
§ Hemoglobin was 11.4 GM/DL, serum creatinine 1.3 MG/DL. NT pro BNP was 567. ECG showed sinus rhythm & LVH. Echo showed Degenerative mitral bioprosthetic valve with severe restenosis, low moderate MR, PPG/MPG : 22/10 MMHG, dilated LA/LV/RA, global hypokinesia of LV, preserved LV systolic function, RV dysfunction, TAPSE – 14 MM, with severe PAH ( RVSP : 66 MMHG ). STS risk mortality score for re do MVR is 6. CT TMVR showed 26 mm valve suitable with neo LVOT of 144.3 MM2.
Relevant Catheterization Findings
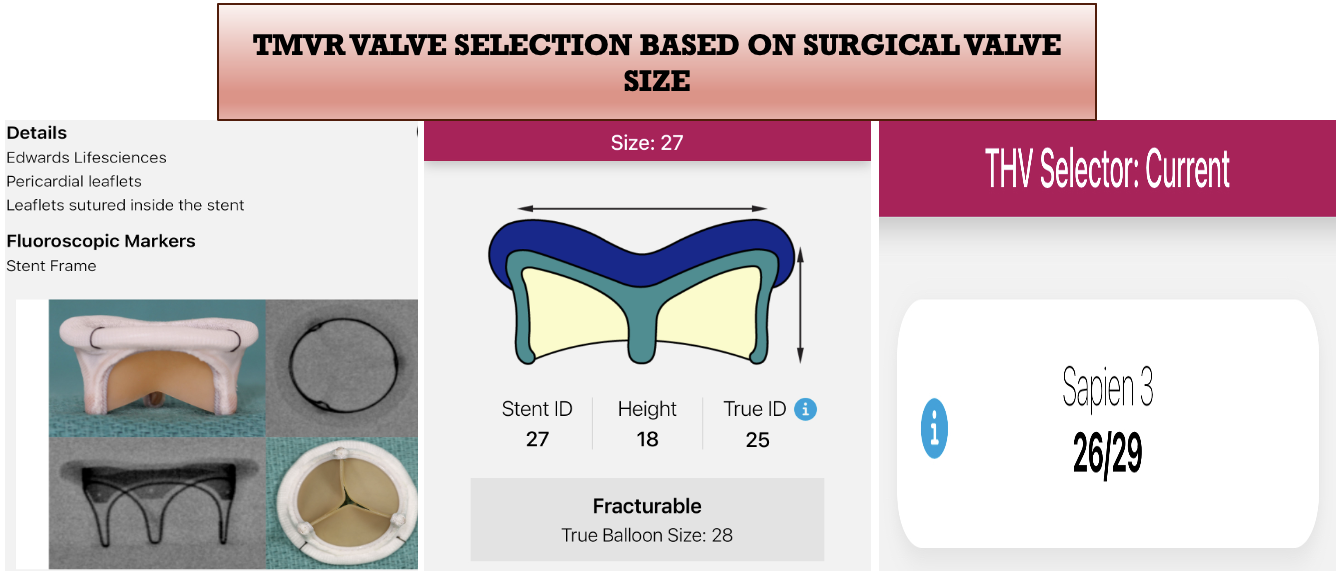
Pre operative details of bio prosthetic valve and TMVR valve sizing is done through VIV app, which showed 26 MM Sapiens valve to be appropriate with need for LAMPOON in view of narrow neo LVOT and post dilation in case of para valvular leak or patient prosthesis mismatch.
Interventional Management
Procedural Step
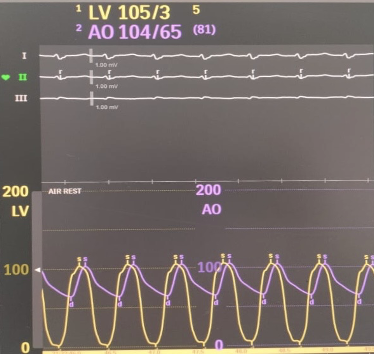
Under TEE guidance, right femoral vein as primary access, left femoral vein for TPI, left femoral access for pigtail were taken. Septal puncture was done Postero Inferiorly using SL1 8.5 sheath, with BRK needle. Later LA wire placed. SL 1 sheath exchanged with Edward sheath. Over safari 0.035, Agilis 8.5 F stearable sheath placed into LA. Exchange length terumo wire passed across the AV into ascending aorta. Pig tail catheter is exchanged with MPA catheter. A 300 CM Astato wire is taken and bent in the middle and denuded to make a flying V. Then it is passed into ascending aorta. The Astato wire is snared with Goose neck snare (20), through JR, via the left femoral artery to form an AV Loop. Once AV loop is formed Astato wire is insulated by parking microcatheter through arterial side and MPA through venous side. Once the position of the flying 'V' is confirmed in the middle of prosthetic valve leaflet, under continuous dextrose infusion the leaflet is cut with electro cautery pencil. After Lampoon, Astato wire along with AV loop is removed. Then Safari wire is place in LV with help of pigtail. Septal dilatation was done with 12x40mm Mustang balloon. The Edwards Commander delivery system, pre-loaded with Edwards Sapiens 26mm Valve.valve was positioned and deployed. Post deployment there was mild PVL noted in TEE hence the valve was dilated with 26mm Atlas Gold Balloon. After post dilatation there was no PVL. There was no neo LVOT gradient. Post OP hemodynamics were stable.
Case Summary
• Pre operative details of bio prosthetic valve details and TMVR valve sizing is done through VIV app, which showed 26 mm valve to be appropriate with need for post dilation along with LAMPOOEvaluation of Neo aortic area is crucial for TMVR to avoid Neo LV outflow tract obstruction.