
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-229
Mechanical Rotational Atherectomy Followed by Balloon Angioplasty of the Right Superficial Femoral Artery With Stenting
By Konstantin Zavialov, Teymur Ibragimov
Presenter
Konstantin Zavialov
Authors
Konstantin Zavialov1, Teymur Ibragimov1
Affiliation
Bashkir State Medical University, Russian Federation1,
View Study Report
TCTAP C-229
Endovascular - Iliac / SFA Intervention
Mechanical Rotational Atherectomy Followed by Balloon Angioplasty of the Right Superficial Femoral Artery With Stenting
Konstantin Zavialov1, Teymur Ibragimov1
Bashkir State Medical University, Russian Federation1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Patient L, 65 years. Complaints: intermittent claudication when walking up to 100 meters, especially on the right. History of the disease: Considers himself ill for about 3 years. The onset of the disease is gradualDiagnosis: Atherosclerosis. Occlusion of the right femoral artery. CAN 2B. Condition after endovascular transluminal balloon angioplasty of the right superficial femoral artery with stenting on 2022.
Relevant Test Results Prior to Catheterization
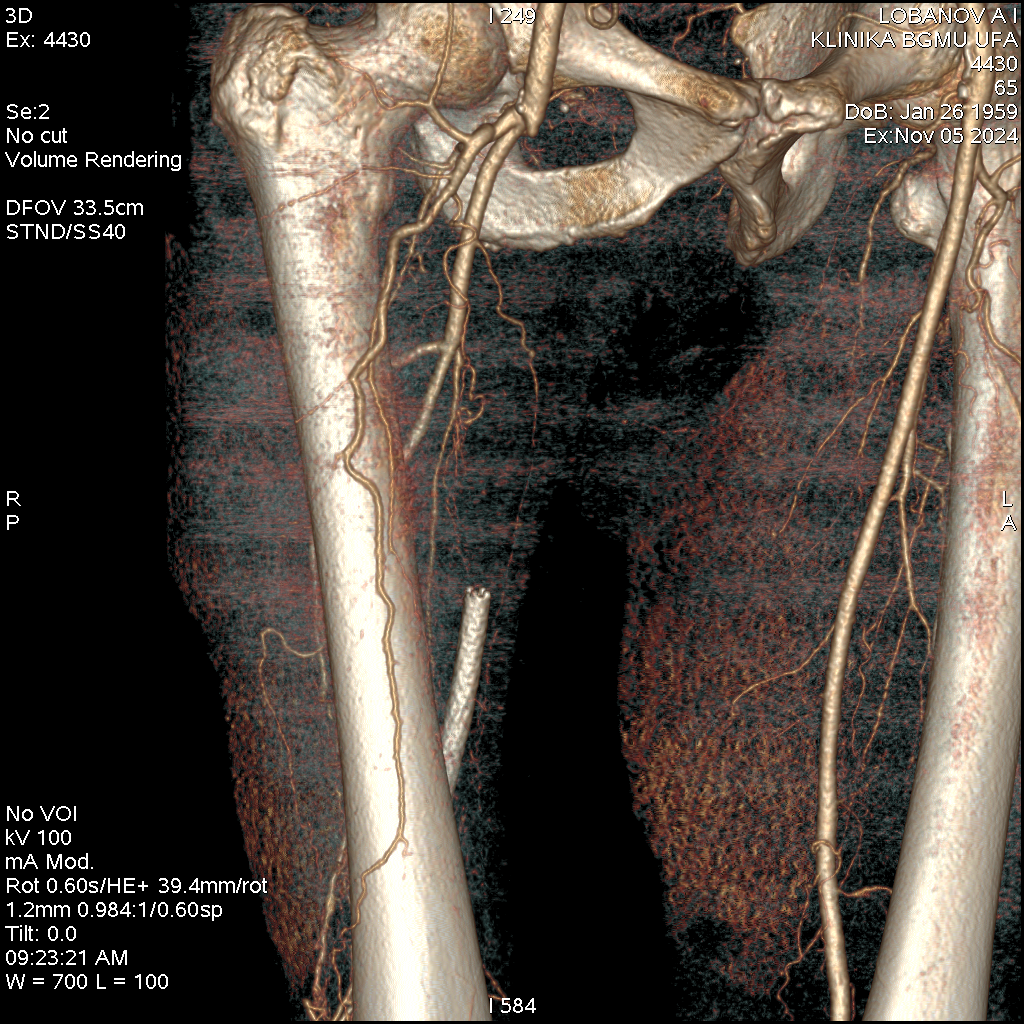
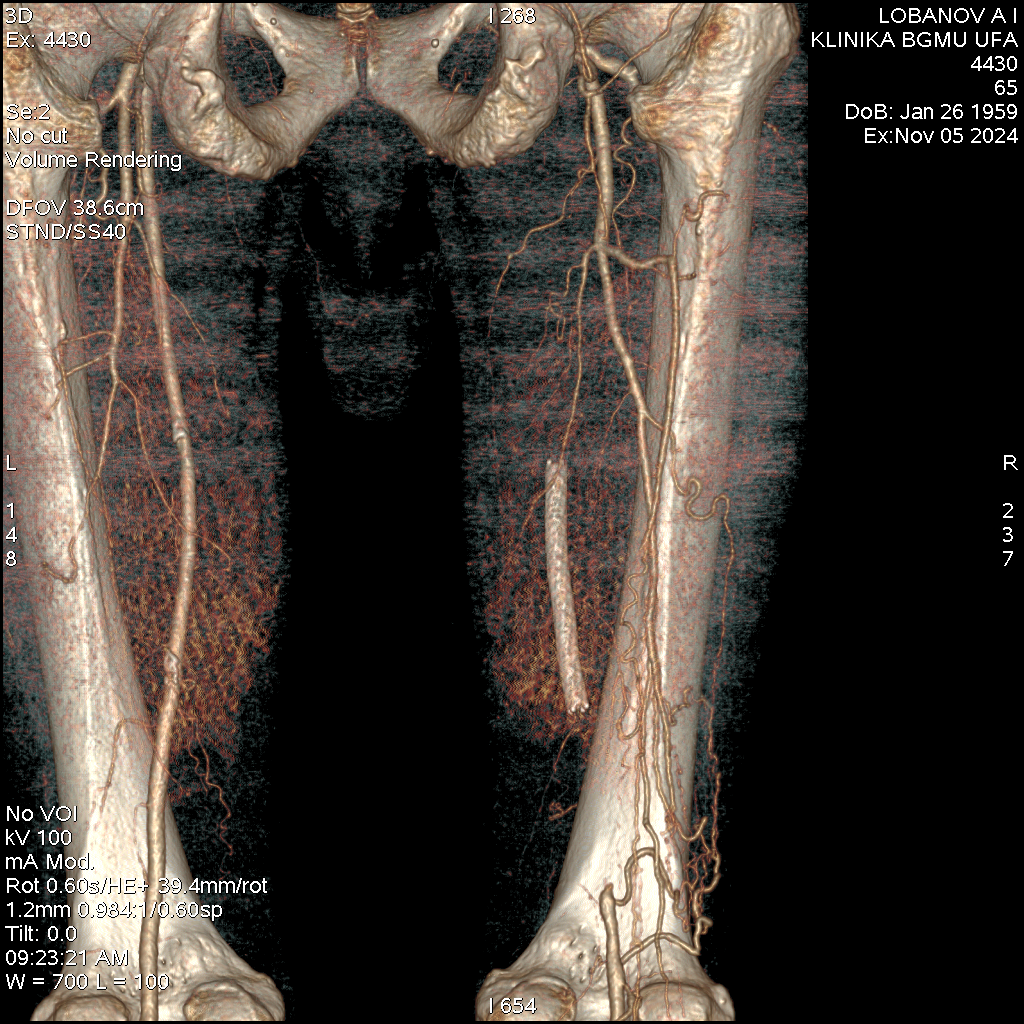
Occlusive lesion: right SFA; total stent thrombosis of the right SFA; right TPS; right PTA; right IBA; left SBA. Stenosis: infrarenal aorta up to 28%; right OBA up to 24%; left OBA up to 20%; left SFA up to 21%.
Relevant Catheterization Findings
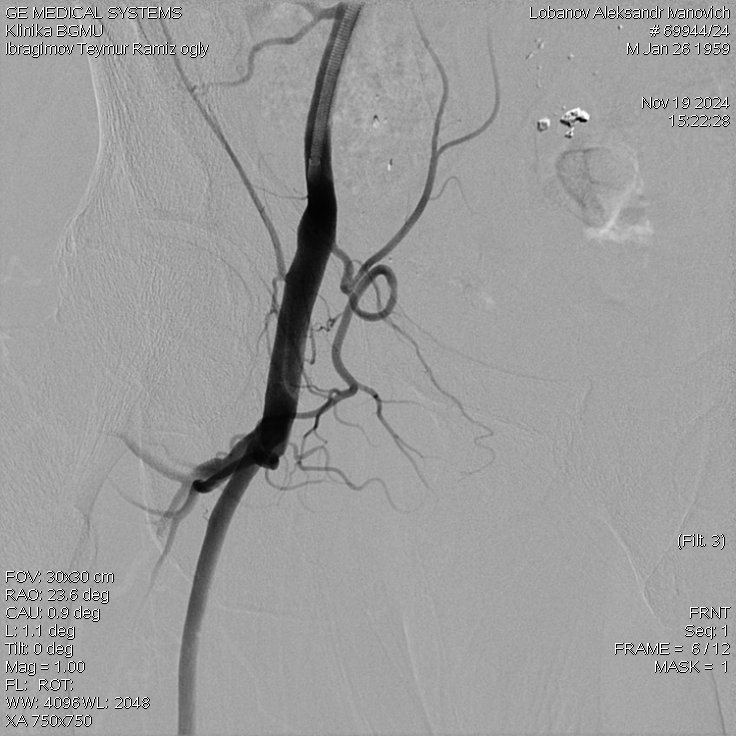
Occlusion of the right superficial femoral artery from the mouth with restoration of contrast in the popliteal artery above the knee joint space; a non-functioning stent is visualized in the projection of the middle third of the superficial femoral artery.
Interventional Management
Procedural Step
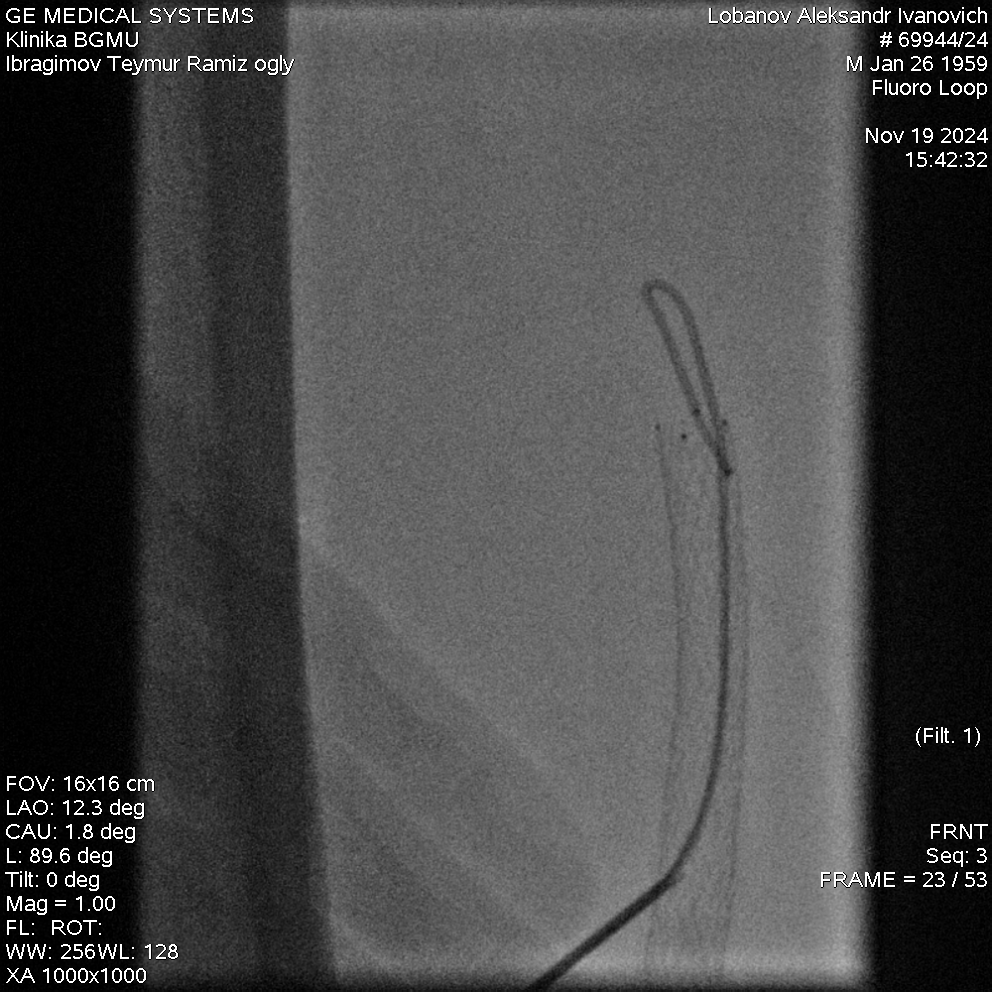
The left common femoral artery was retrogradely punctured, and the contralateral iliac artery was catheterized. A Destination 7Fr 45 cm introducer catheter was installed. With a 0.035" 260.0 cm guidewire, it was not possible to antegradely recanalize the occlusion. The right superficial femoral artery was retrogradely punctured at the stent level. With a 0.035" 260.0 cm Roadrunner guidewire, retrograde recanalization of the superficial femoral artery was performed at the level of the middle and upper third of the thigh, the guidewire was brought out through the Destination 7Fr 45 cm introducer catheter. Antegrade recanalization of the superficial femoral artery was performed. A Boston Scientific Jetstream XC atherectomy catheter was inserted through the Command ES 0.014" 300.0 cm guidewire, and atherectomy of the superficial femoral artery was performed. A Ranger 6.0*150 mm balloon catheter was inserted through the Command ES 0.014" 300.0 cm guidewire. Balloon angioplasty of the superficial femoral artery was performed. A filling defect of the superficial femoral artery at the orifice with stenosis of up to 85% is visualized. An Isthmus 6*19 mm stent system was inserted through the 0.035" 260.0 cm guidewire. The stent was implanted at the level of the orifice of the superficial femoral artery.
Case Summary
In endovascular surgery practice, standard arterial puncture techniques are widely used and well-established. However, in some non-standard clinical situations, there is a need for alternative approaches to puncture, which help preserve vital vessels. This is especially relevant for patients with chronic lower limb ischemia, where it is often necessary to preserve the only functioning artery, such as the tibial artery. In such cases, the use of non-standard puncture techniques can be crucial in preventing further deterioration of blood circulation and preserving limb function