
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-216
A Challenging Case Report: Concomitant M/T TEER in Post Infarct Papillary Muscle Rupture
By Su Min Lim, Senthilraj Thangasami, Antonio Felipe Leite Simao, Bin Wang, Xiang Chen, Xu Chen, Mao Long Su, Yan Wang
Presenter
Su Min Lim
Authors
Su Min Lim1, Senthilraj Thangasami1, Antonio Felipe Leite Simao1, Bin Wang1, Xiang Chen1, Xu Chen1, Mao Long Su1, Yan Wang1
Affiliation
Xiamen Cardiovascular Hospital, China1,
View Study Report
TCTAP C-216
Structural - Mitral Valve Intervention - Transcatheter MV Repair
A Challenging Case Report: Concomitant M/T TEER in Post Infarct Papillary Muscle Rupture
Su Min Lim1, Senthilraj Thangasami1, Antonio Felipe Leite Simao1, Bin Wang1, Xiang Chen1, Xu Chen1, Mao Long Su1, Yan Wang1
Xiamen Cardiovascular Hospital, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
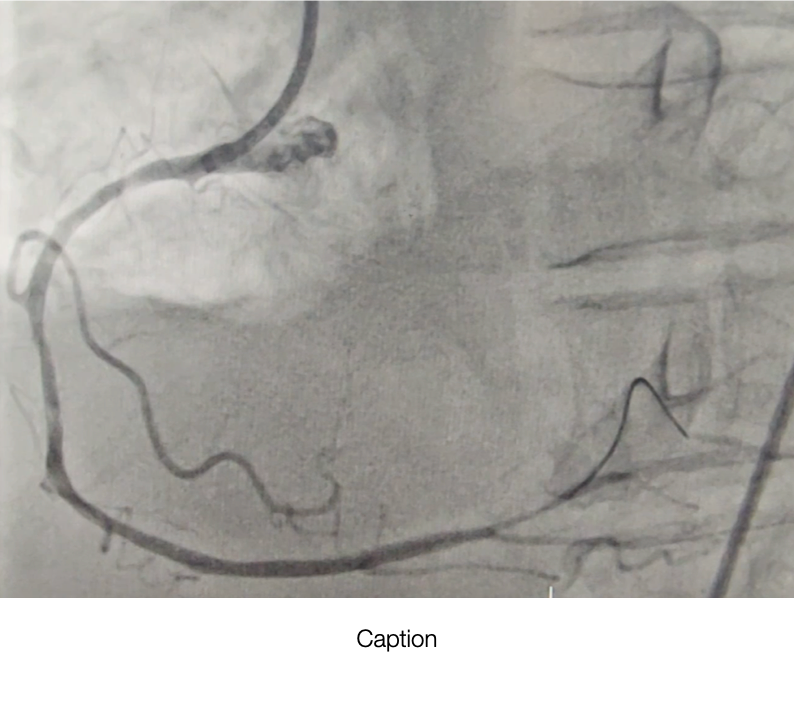
85-year-old male presented with Inferior STEMI in cardiogenic shock, pulmonary oedema and atrial fibrillation. Coros & PCI done, dRCA was stented. However patient remained persistent hypotensive despite PCI ,IABP and fluid challenge. ECHO revealed that the patient has severe mitral regurgitation, severe tricuspid regurgitation and ruptured chordae tendinae.

Relevant Test Results Prior to Catheterization
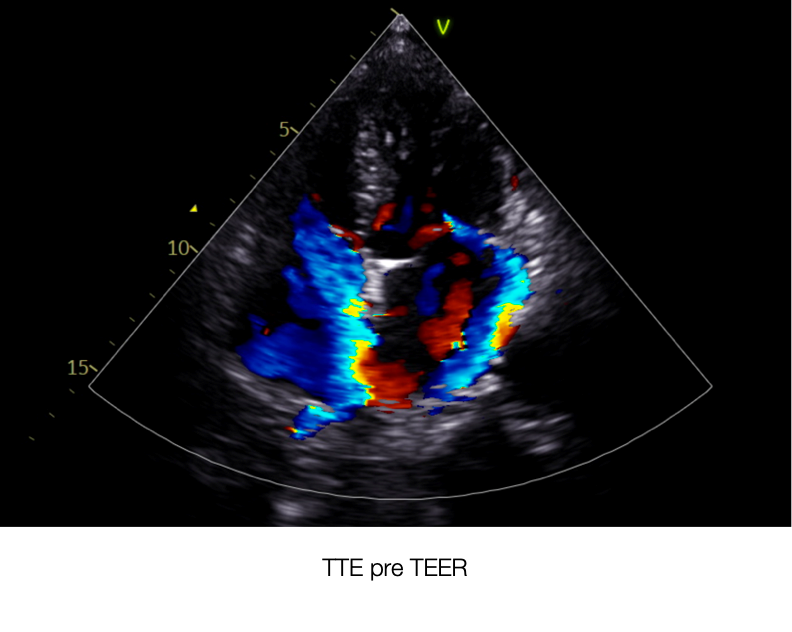
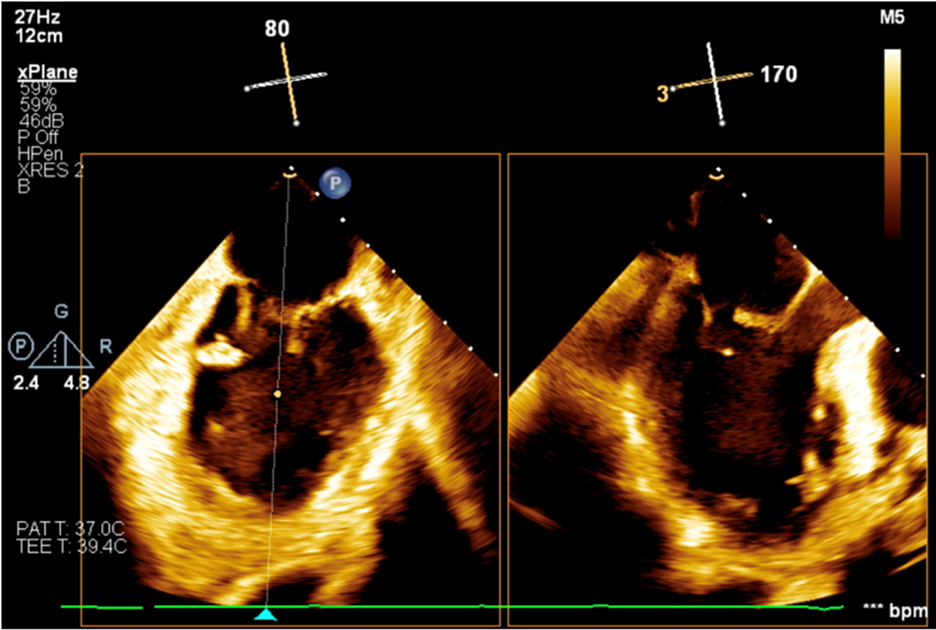
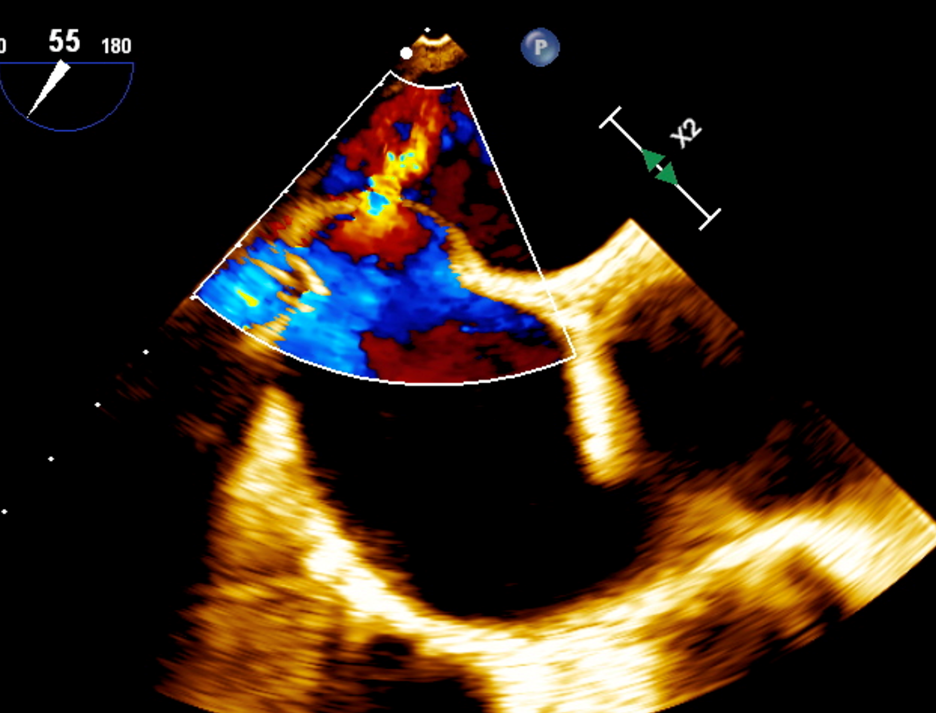
TEE pre procedure : A2 prolapse with papillary muscle ruptured ( DMR 4+), A2 Flail gap 7.7mm , flail width 9.5mmA2 anterior leaflet length 29mm, posterior leaftlet 13mmMVA 4.39cm2Baseline MPG 2mmHg
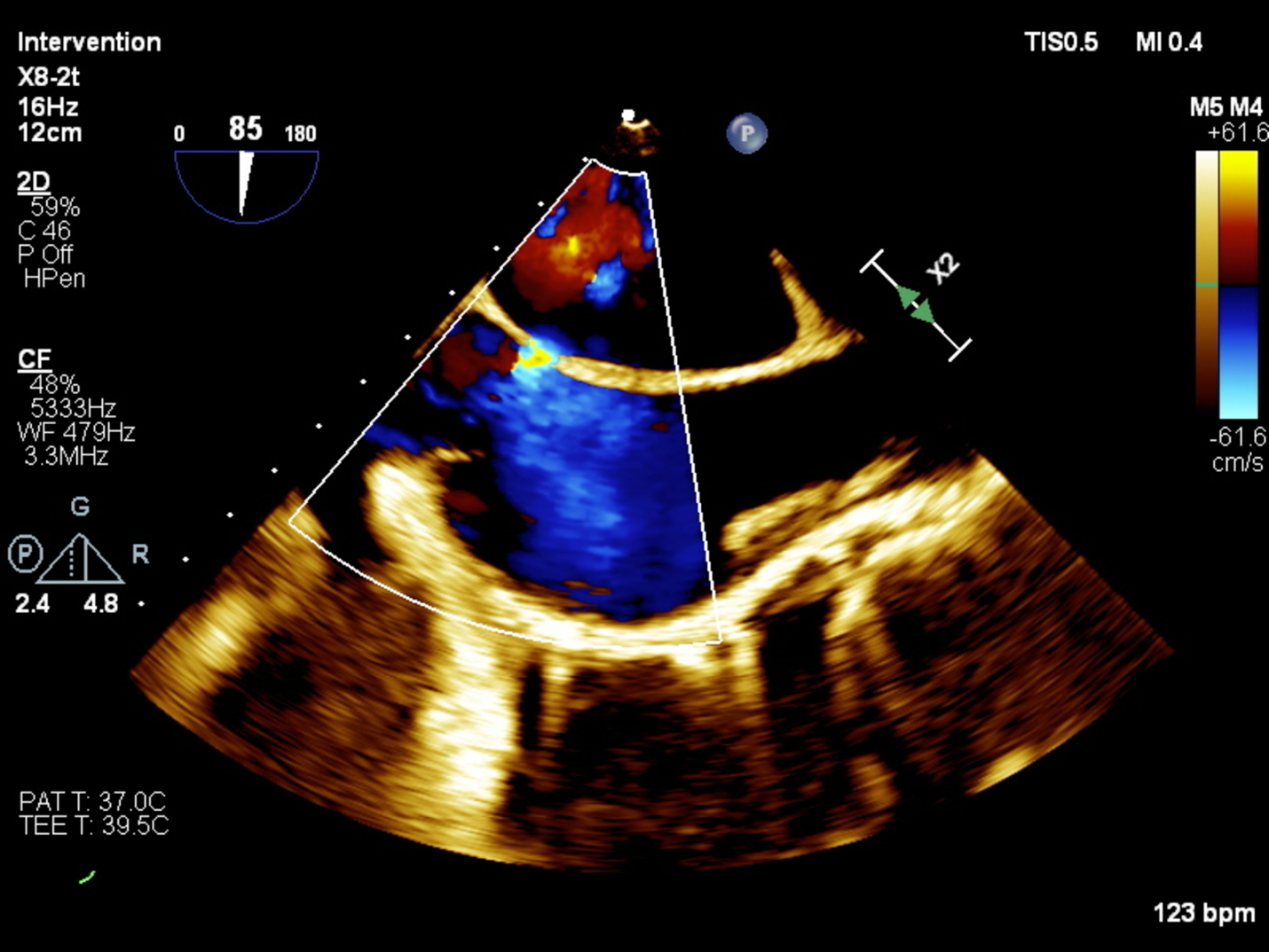
Severe TR with prolapsed posterior leaflet. Flail gap 8.7mmPosterior leaflet length 31mmSeptal leaflet length 16mmRegurgitant jet from posteroseptalVena contracta 18mm ( flail gap)Baseline MPG 1mmHgRUPV & LUPV systolic flow reversal seenLeft hepatic vein systolic flow reversal seen
Severe TR with prolapsed posterior leaflet. Flail gap 8.7mmPosterior leaflet length 31mmSeptal leaflet length 16mmRegurgitant jet from posteroseptalVena contracta 18mm ( flail gap)Baseline MPG 1mmHgRUPV & LUPV systolic flow reversal seenLeft hepatic vein systolic flow reversal seen
Relevant Catheterization Findings
There were severe mitral regurgitation with A2 prolapse & ruptured chordae tendinae. There is also concomitant severe tricuspid regusgitation.
Interventional Management
Procedural Step
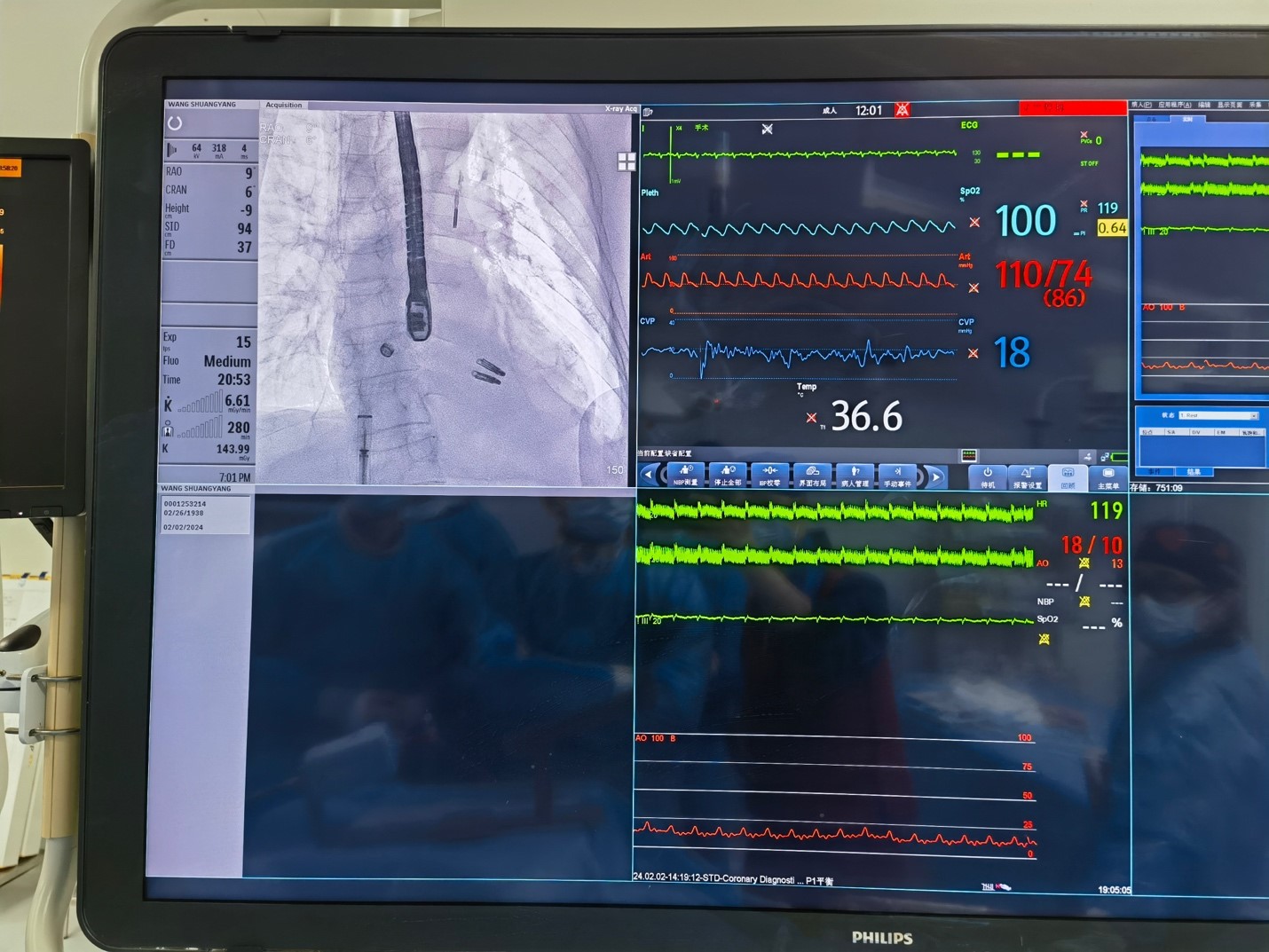
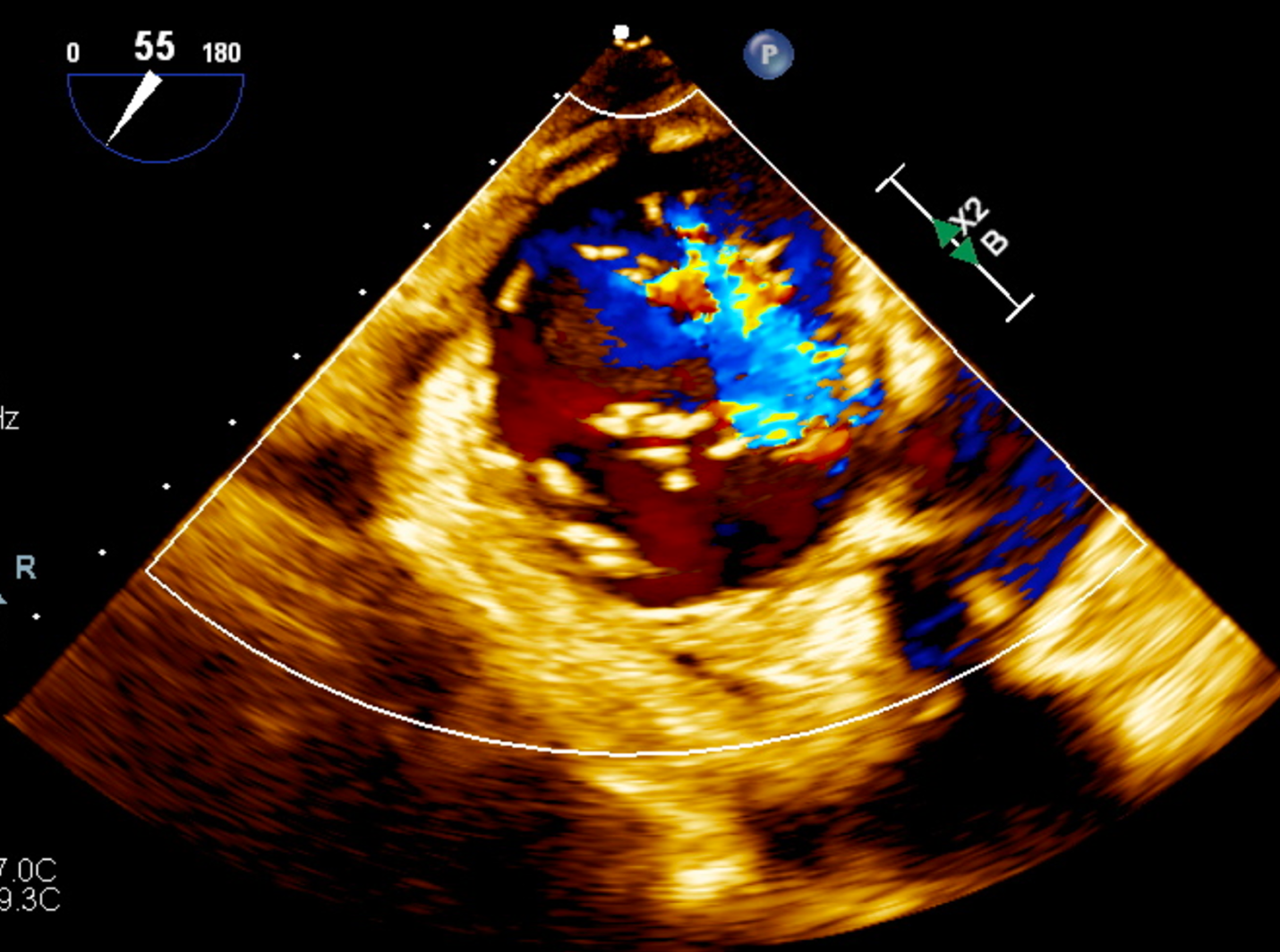
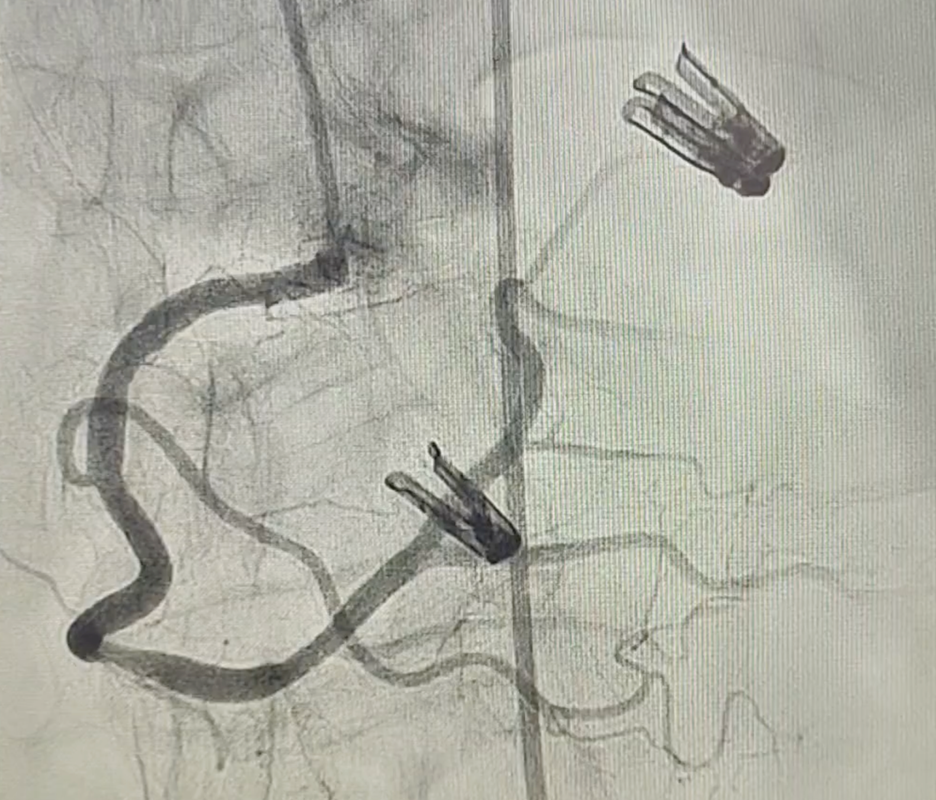
Two mitral clips were applied and achieved MR reduction to 1+.
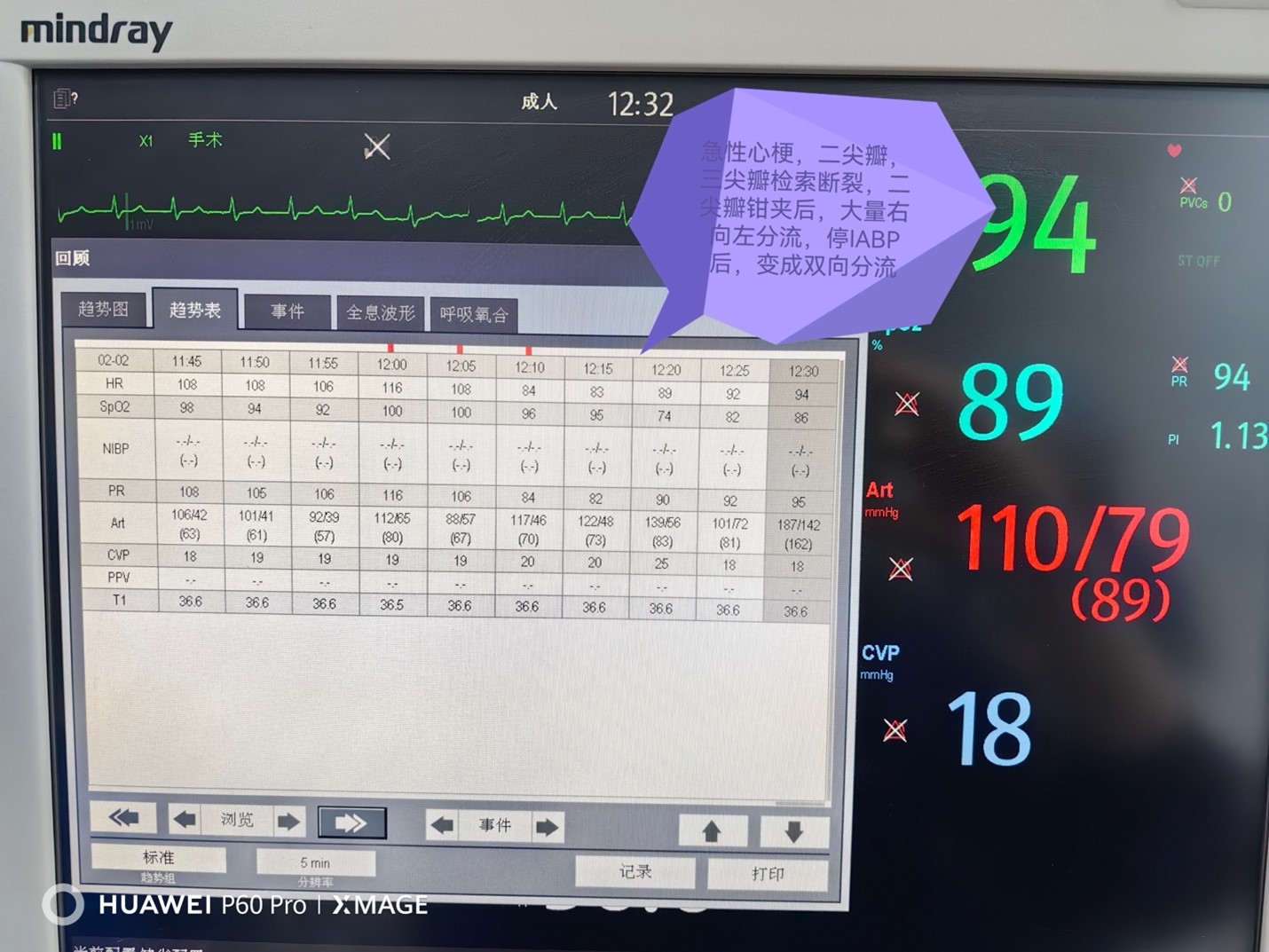
Upon withdrawal of the steerable guide catheter into the RA, we noted right to left shunt in the transseptal puncture site and worsening of TR, drop in oxygen saturation requiring increased ventilator setting. IABP was stopped and it became bidirectional shunt. There were 2 potential options. Either putting in a ASD closure device or to intervene TR. In view of severe TR even before M TEER , presence of AF and worsening of TR after M TEER, . Decision was made to intervene TR as a combined procedure.
The same Mitral clip system was used for T TEER with the miskey method. There was no tri clip system available at the time of the event. TOE transgastric view showed a postero-septal jet and one XTR was applied. Final check there was only left to right shunt at the IAS. Patient oxygenation improved and able to wean off IABP.
Upon withdrawal of the steerable guide catheter into the RA, we noted right to left shunt in the transseptal puncture site and worsening of TR, drop in oxygen saturation requiring increased ventilator setting. IABP was stopped and it became bidirectional shunt. There were 2 potential options. Either putting in a ASD closure device or to intervene TR. In view of severe TR even before M TEER , presence of AF and worsening of TR after M TEER, . Decision was made to intervene TR as a combined procedure.
The same Mitral clip system was used for T TEER with the miskey method. There was no tri clip system available at the time of the event. TOE transgastric view showed a postero-septal jet and one XTR was applied. Final check there was only left to right shunt at the IAS. Patient oxygenation improved and able to wean off IABP.
Case Summary
The decision to proceed to Mitral clips instead of surgical treatment was made in view of patient’s high surgical risk. Further TEER of tricuspid valve using the Mitra Clips system was under the circumstances the only option available at the moment in order to give the patient a chance of life. The iatrogenic shunt reversal was probably due to concomitant severe TR and afterload mismatch after MR correction.