
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-054
IVUS Guided Rota-Tripsy in a Severely Calcified Critical Left Anterior Descending Artery Stenosis
By Saurabh Dhumale, Saroj Kumar Choudhury, Debdatta Bhattacharyya
Presenter
Saurabh Dhumale
Authors
Saurabh Dhumale1, Saroj Kumar Choudhury1, Debdatta Bhattacharyya1
Affiliation
Narayana Hospital RN Tagore Hospital, India1,
View Study Report
TCTAP C-054
Coronary - Complex PCI - Calcified Lesion
IVUS Guided Rota-Tripsy in a Severely Calcified Critical Left Anterior Descending Artery Stenosis
Saurabh Dhumale1, Saroj Kumar Choudhury1, Debdatta Bhattacharyya1
Narayana Hospital RN Tagore Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 73-year-old diabetic, hypertensive gentleman presented to ER with complaints of progressive angina and shortness of breath for the past 3 days. Upon investigation, his blood work revealed elevated Hs-Troponin I levels 5340 ng/L, elevated NTPro-BNP levels 4360 pg/ml, raised serum creatinine 1.35 mg/dl and raised capillary blood glucose 188 mg/dl. He was managed initially with intravenous diuretics, low molecular weight heparin and vasodilators.


Relevant Test Results Prior to Catheterization
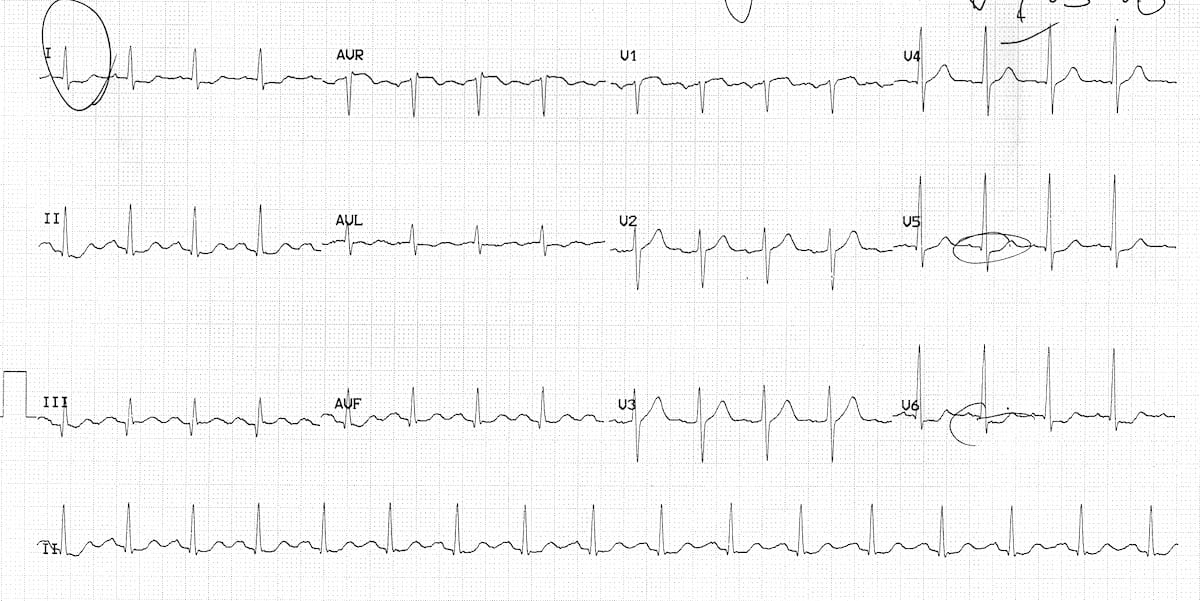
His ECG revealed non-specific ST changes, while ECHO-Doppler revealed an eccentrically dilated LV with hypokinesis with preserved muscle mass in the LAD territory with LV ejection fraction of 44%. There was no significant valvular abnormality or any evidence of pulmonary hypertension.
Relevant Catheterization Findings
After initial efforts at stabilization, patient was taken up for angiogram. His angiogram revealed a chronic total occlusion with JCTO score 3 in the dominant right coronary artery with retrograde filling from the left coronary system, the left circumflerx was a small sized vessel with minor plaquing, while the left anterior descending artery was effectively the single surviving major vessel with a long segment calcific tubular stenosis from the ostium extending up to the mid part (max 95%).
Interventional Management
Procedural Step
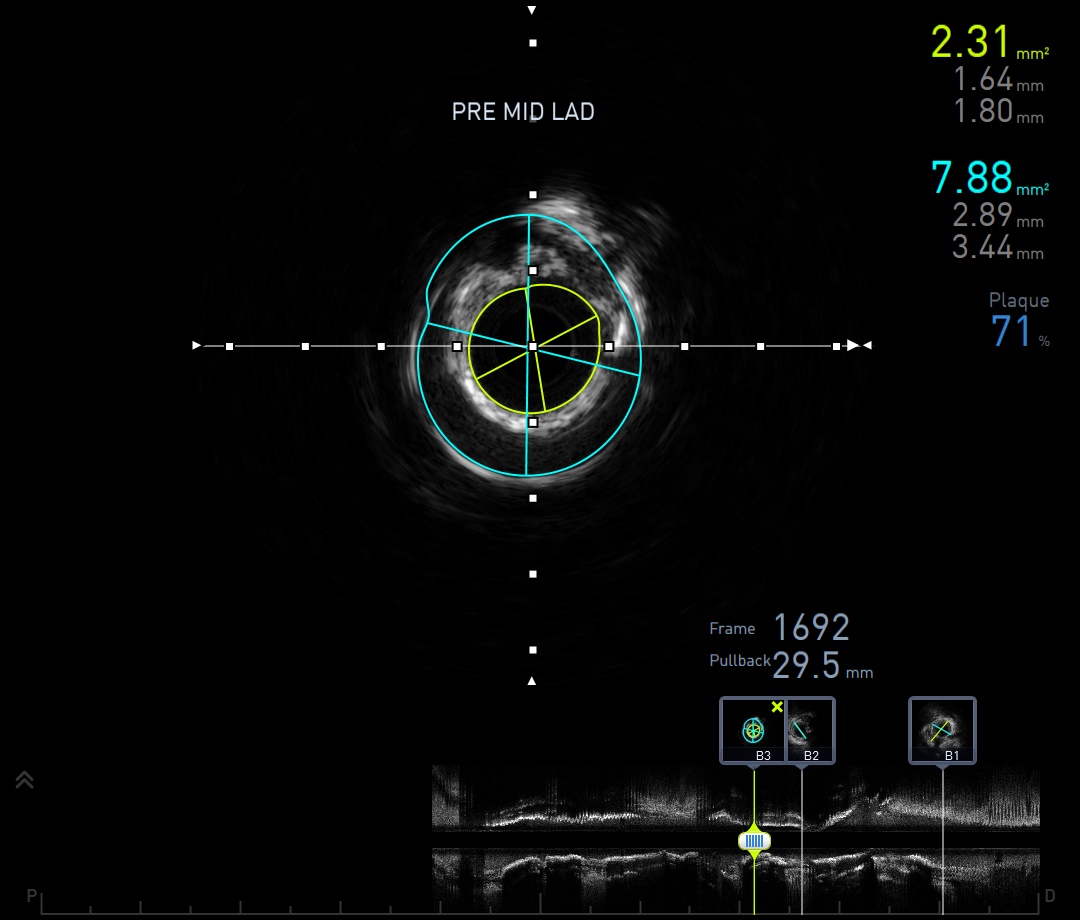
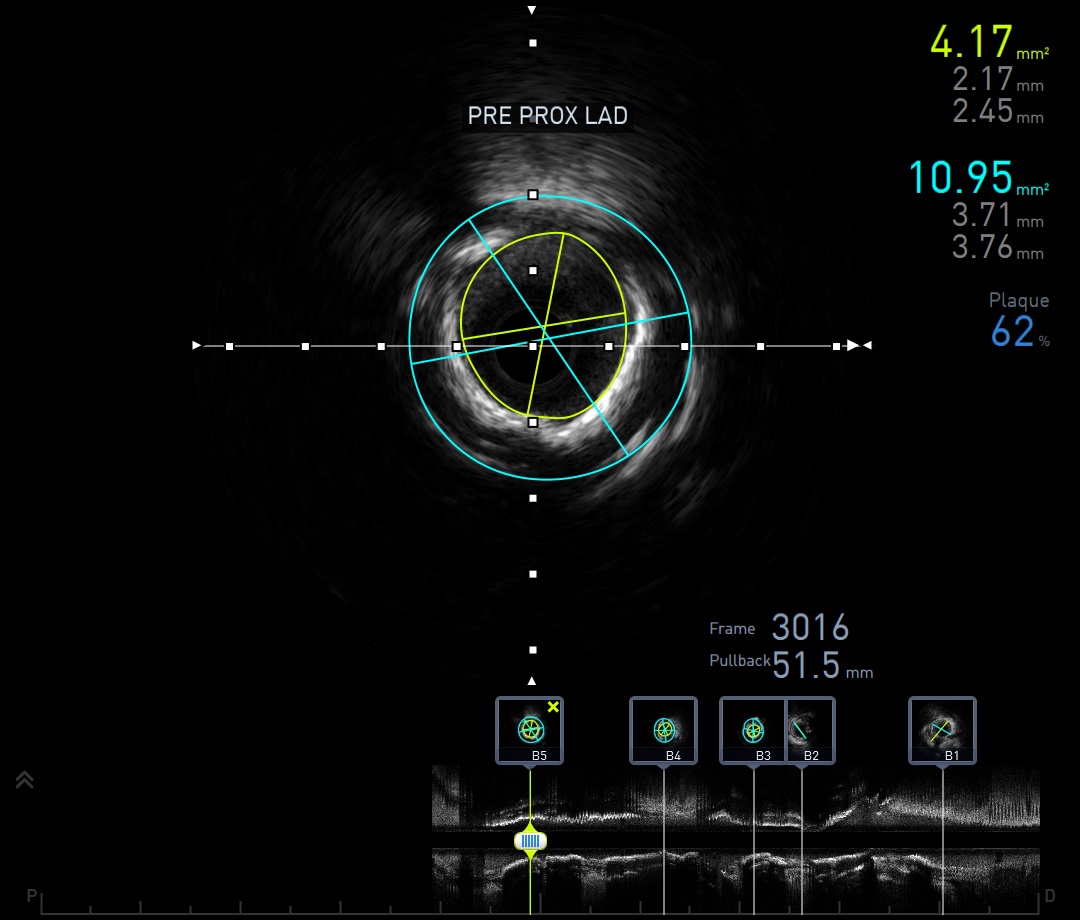
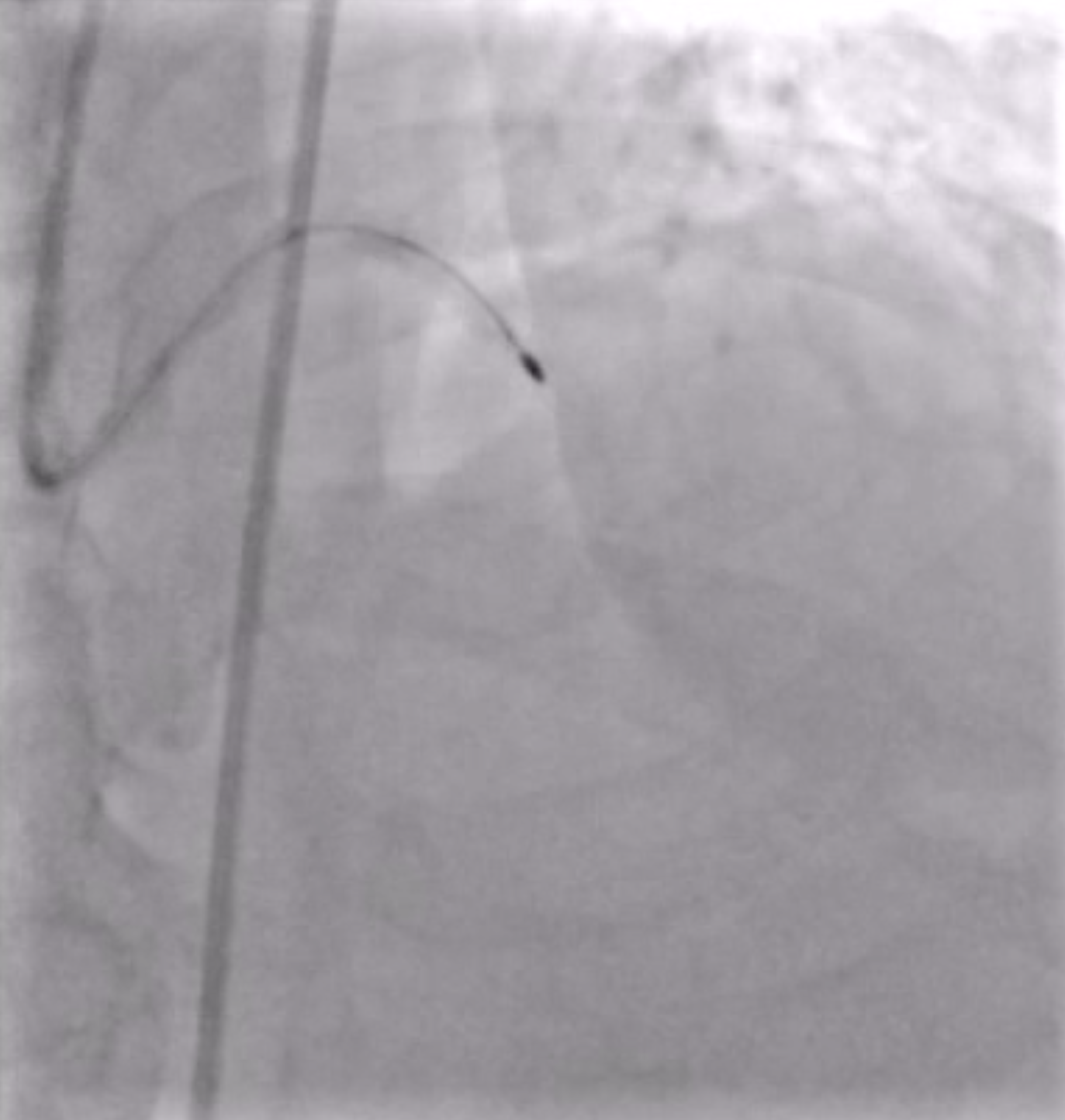
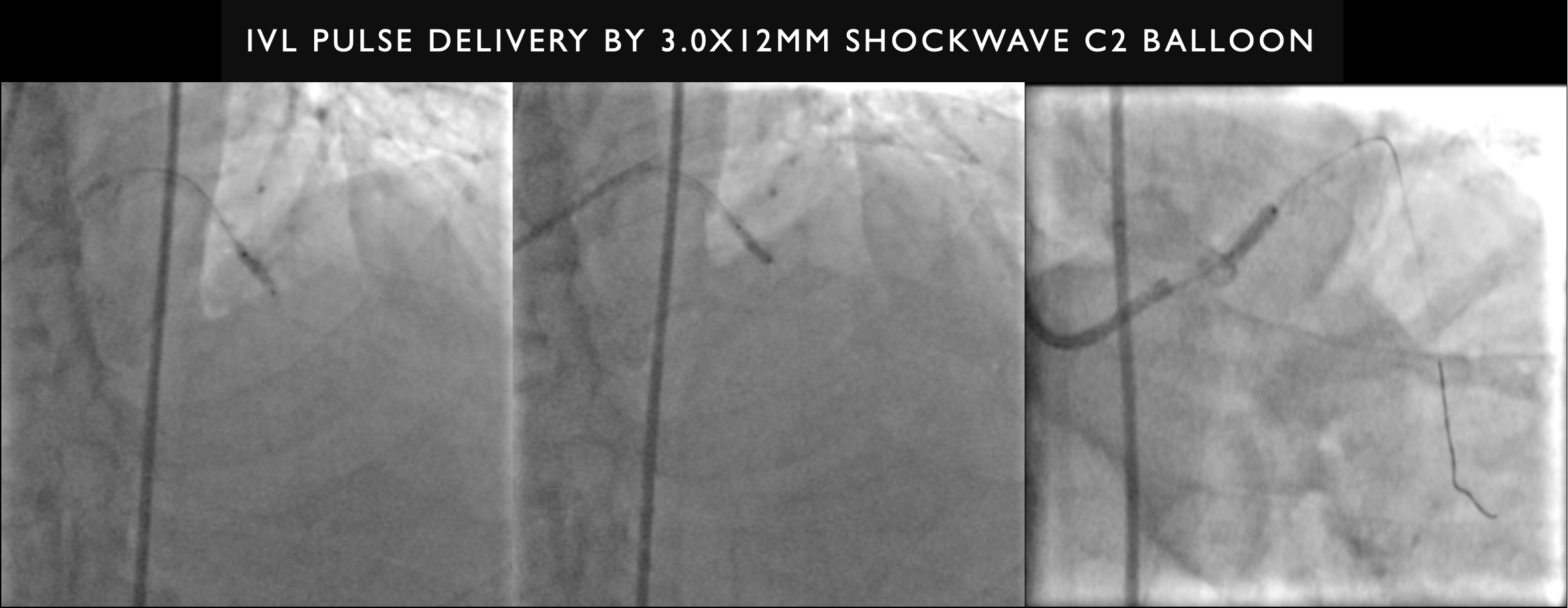
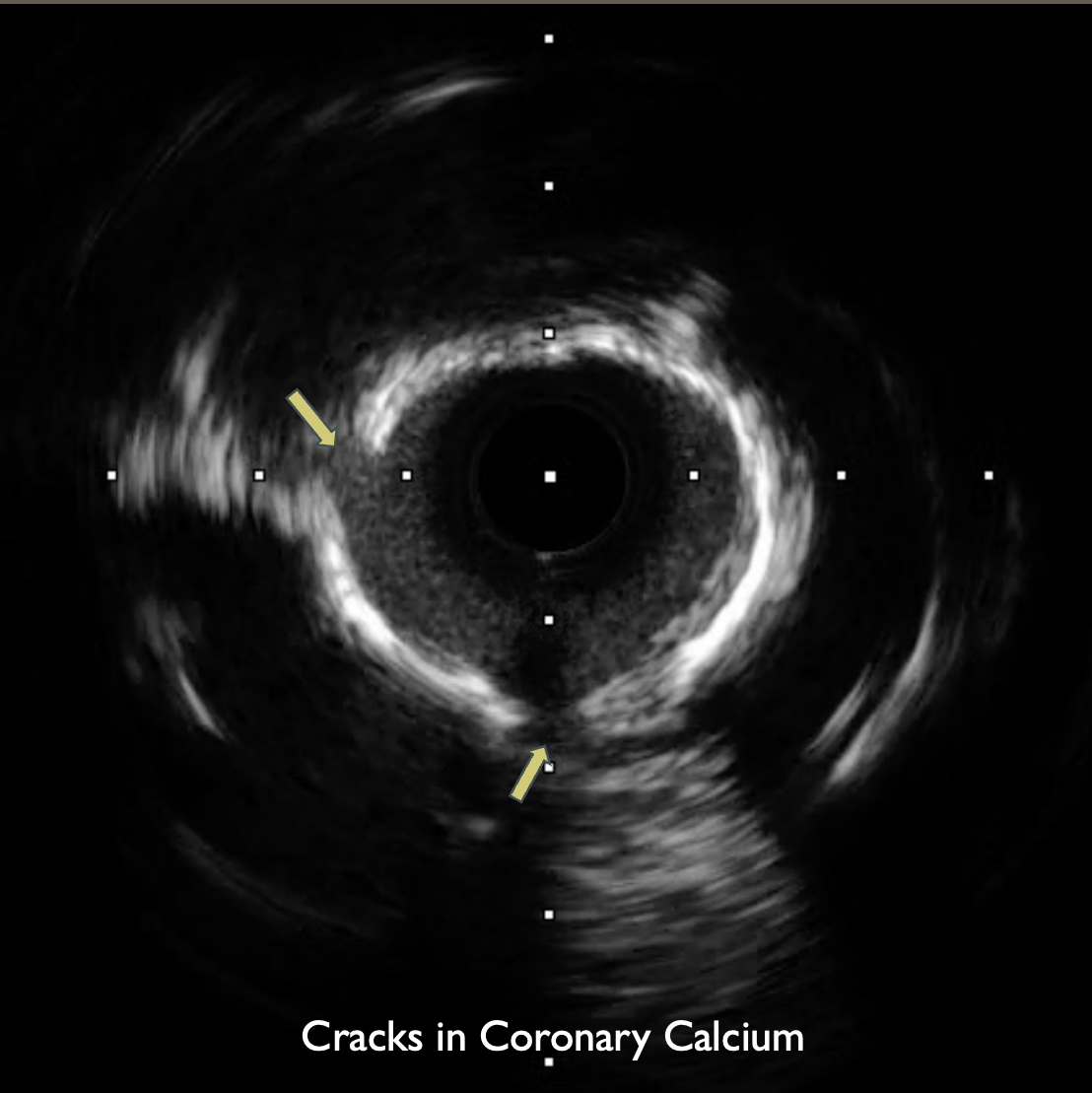
After careful deliberation and heart team approach, it was decided to proceed with PCI to LAD with Imaging and calcium modification. The left anterior descending artery(LAD) was wired, IVUS was attempted, however, the IVUS catheter wont cross the lesion. Rotablation with 1.5mm burr was started. After initial resistance for burr crossing, we could finally cross and polish the lesion. Post rotablation, IVUS revealed concentric calcium without significant modification and cracking. Intravascular Lithotripsy was employed to create further cracks in the calcium. Post IVL, serial post-dilatations were done with 2.5mm, 3mm and 3.5mm non-compliant balloons. Once the lesion was modified, IVUS run was taken to confirm adequate bed preparation. Said IVUS run confirmed adequate lumen gain and several cracks in the coronary calcium. A 3.5X48mm DES was deployed successfully from proximal to mid left anterior descending artery. The stent was post-dilated with a 3.5mm non-compliant balloon. Final IVUS run revealed adequate stent expansion, apposition and no edge dissection.

Case Summary
Single surviving major arteries are often challenging to treat. Calcification in such cases brings in additional challenge. Imaging and optimum use of calcium modification devices are key in achieving long term success. Our patient had a CTO with JCT score-3 in the RCA, the left circumflex was a small calibre vessel, most of the cardiac circulation was dependent on the LAD which had long tubular stenosis with extensive calcification in the mid and proximal parts. Rotablation and intravascular lithotripsy used in tandem guided by intravascular ultrasound helps in achieving excellent luminal gain as evidenced in this case.