
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-139
Stenting Was Performed for a Spiral Dissection of an Open Vessel, Followed by a Bailout
By Toku Sakashita, Atsushi Sakamoto
Presenter
Toku Sakashita
Authors
Toku Sakashita1, Atsushi Sakamoto1
Affiliation
IMS Fujimi General Hospital, Japan1,
View Study Report
TCTAP C-139
Coronary - Complication Management
Stenting Was Performed for a Spiral Dissection of an Open Vessel, Followed by a Bailout
Toku Sakashita1, Atsushi Sakamoto1
IMS Fujimi General Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
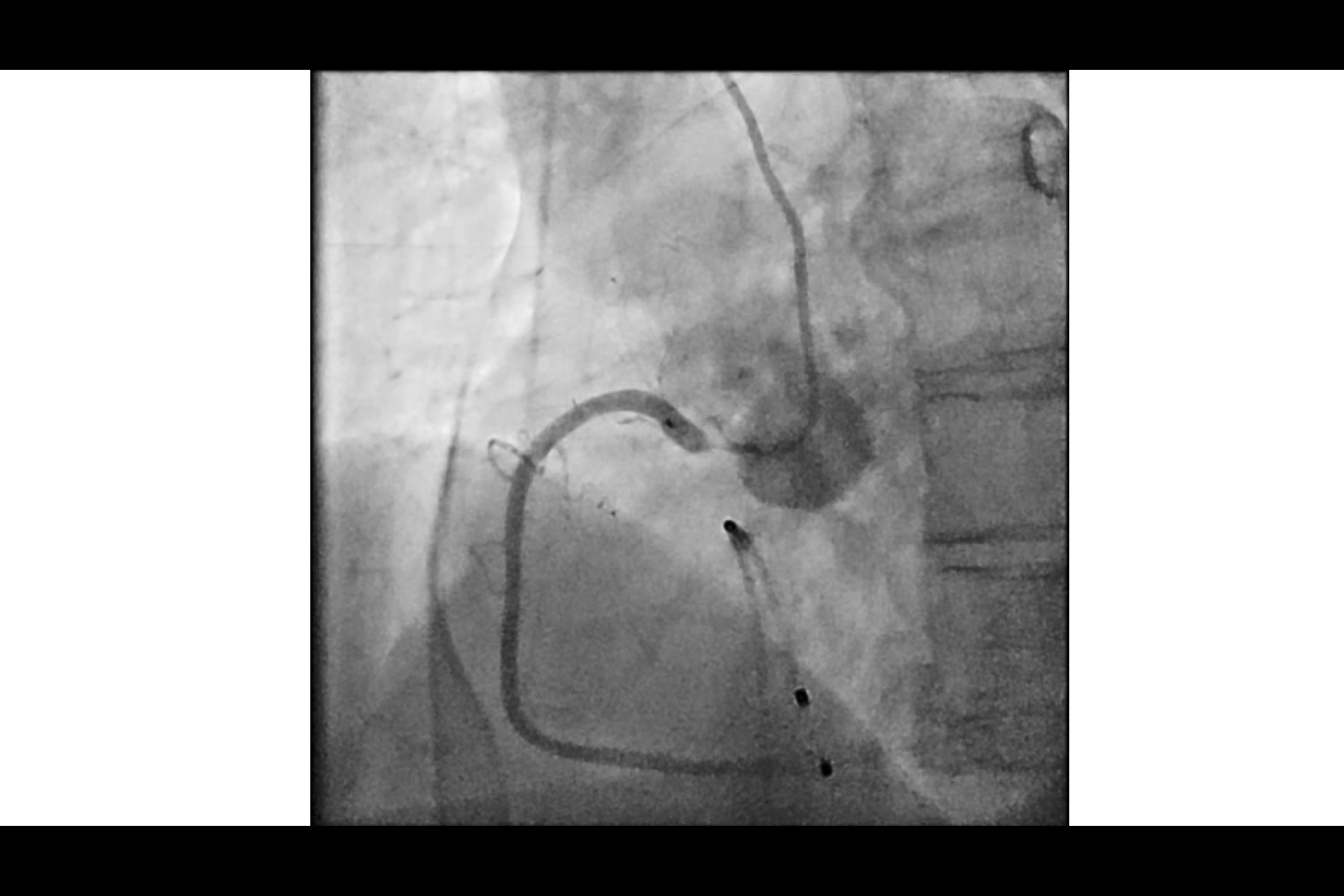
The patient was a 90-year-old woman. She underwent emergency cardiac catheterization due to STEMI.The findings were RCA 99%, #5-6 90%, and #7 90%, so PCI was performed on the RCA.The progress after PCI was uneventful, and cardiac rehabilitation also progressed without any issues.The decision was made to perform staged PCI on the remaining branch.
Relevant Test Results Prior to Catheterization
After the myocardial infarction, peak CK levels rose to approximately 1000.Echocardiogram showed inferior hypokinesis, but cardiac contractility was maintained with an LVEF of 62%, and no valvular disease was found.Blood samples showed mild renal dysfunction with Cr of 1.04 mg/dl and eGFR of 38. The patient was taking oral antiplatelet drugs, but no anemia was found.
Relevant Catheterization Findings
Because the right coronary artery had an abnormal origin, a diagnostic catheter compatible with both the right and left sides was used to insert a treatment catheter.
A guide extension catheter was used in combination and a stent was placed protruding from the entrance.
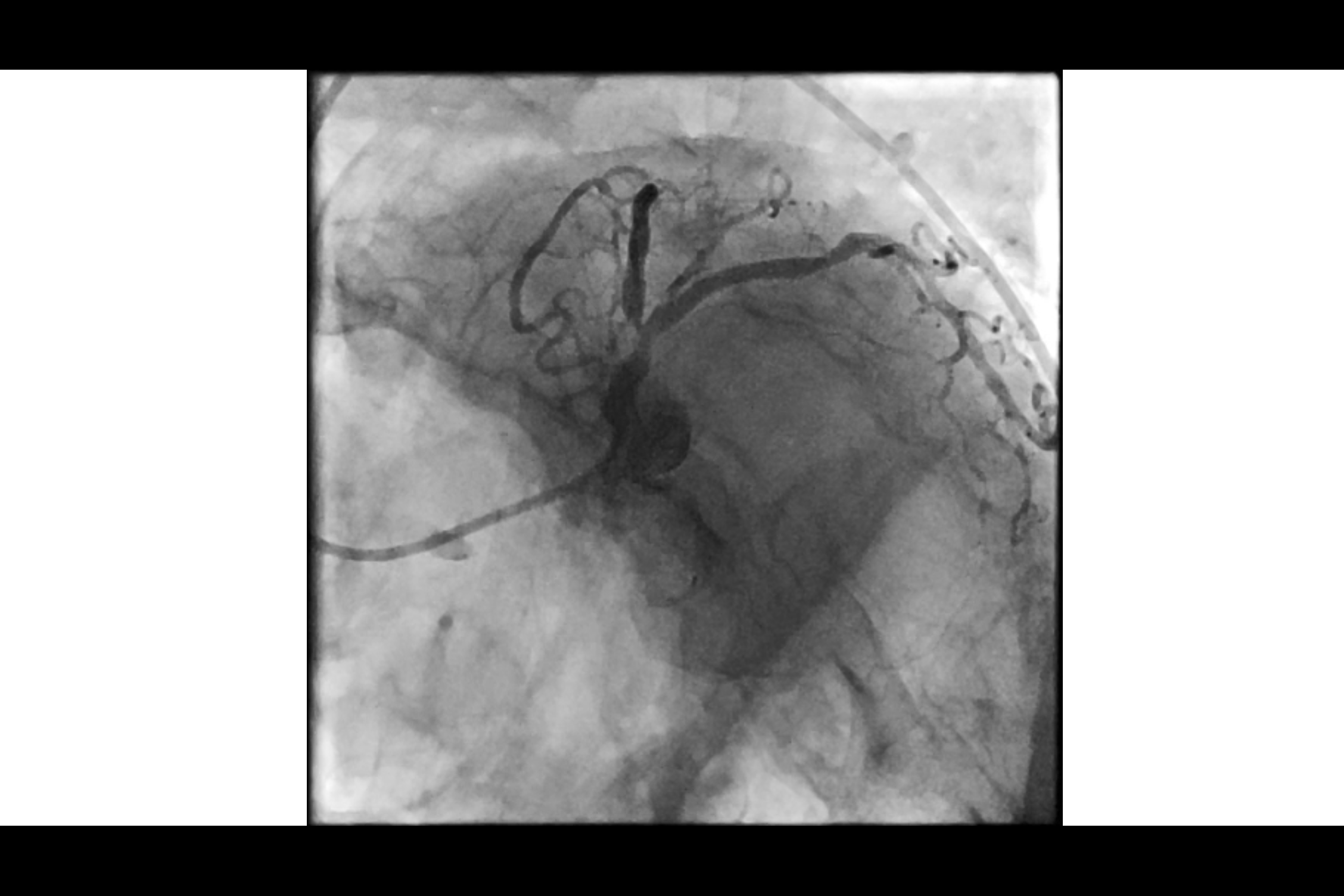
The left coronary artery was found to be #5-6 90%, #7 90%, so staged PCI was performed.
Although cutting using DCA is often performed, the decision was made to proceed with POBA → stent due to the patient's advanced age.
A guide extension catheter was used in combination and a stent was placed protruding from the entrance.
The left coronary artery was found to be #5-6 90%, #7 90%, so staged PCI was performed.
Although cutting using DCA is often performed, the decision was made to proceed with POBA → stent due to the patient's advanced age.
Interventional Management
Procedural Step
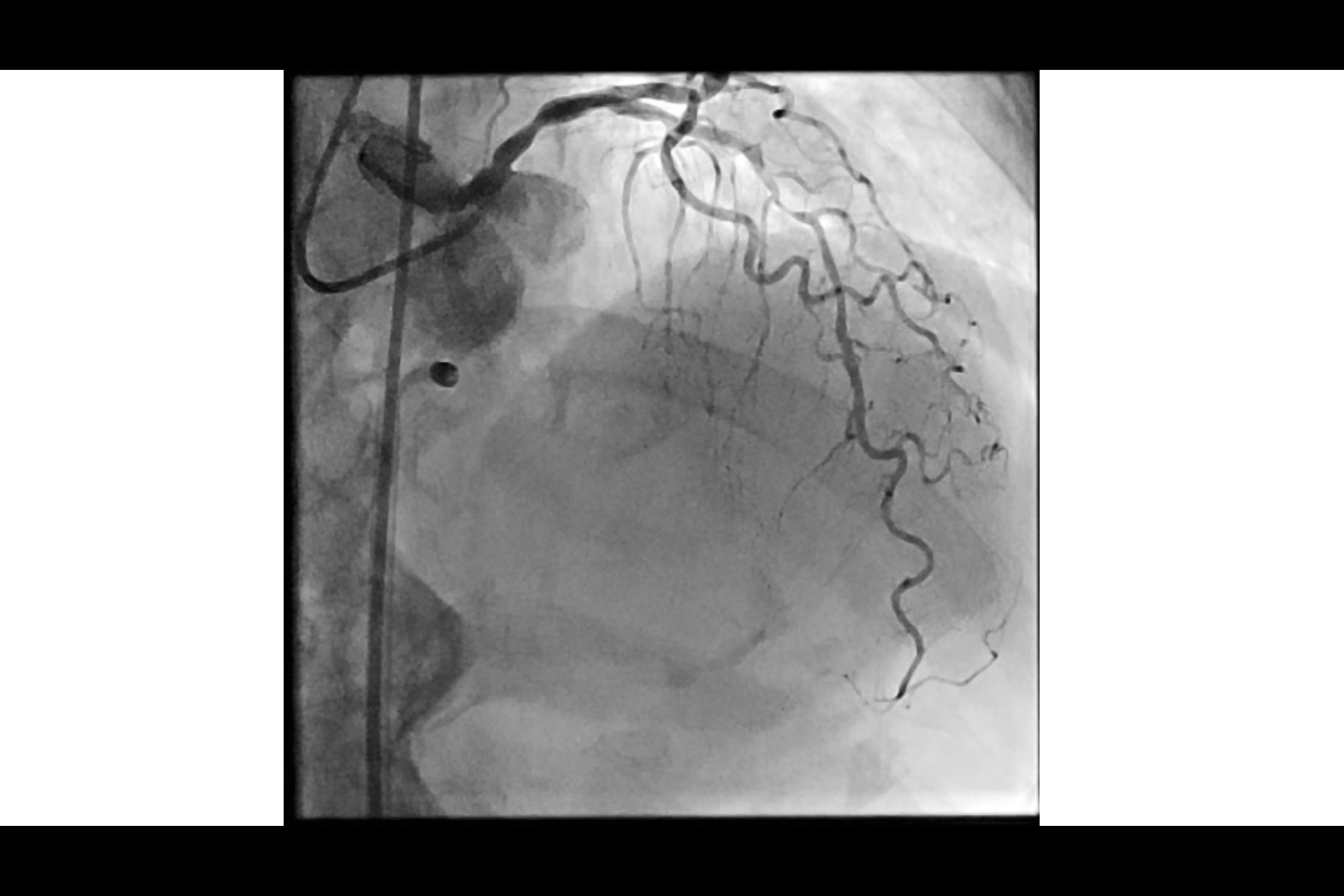
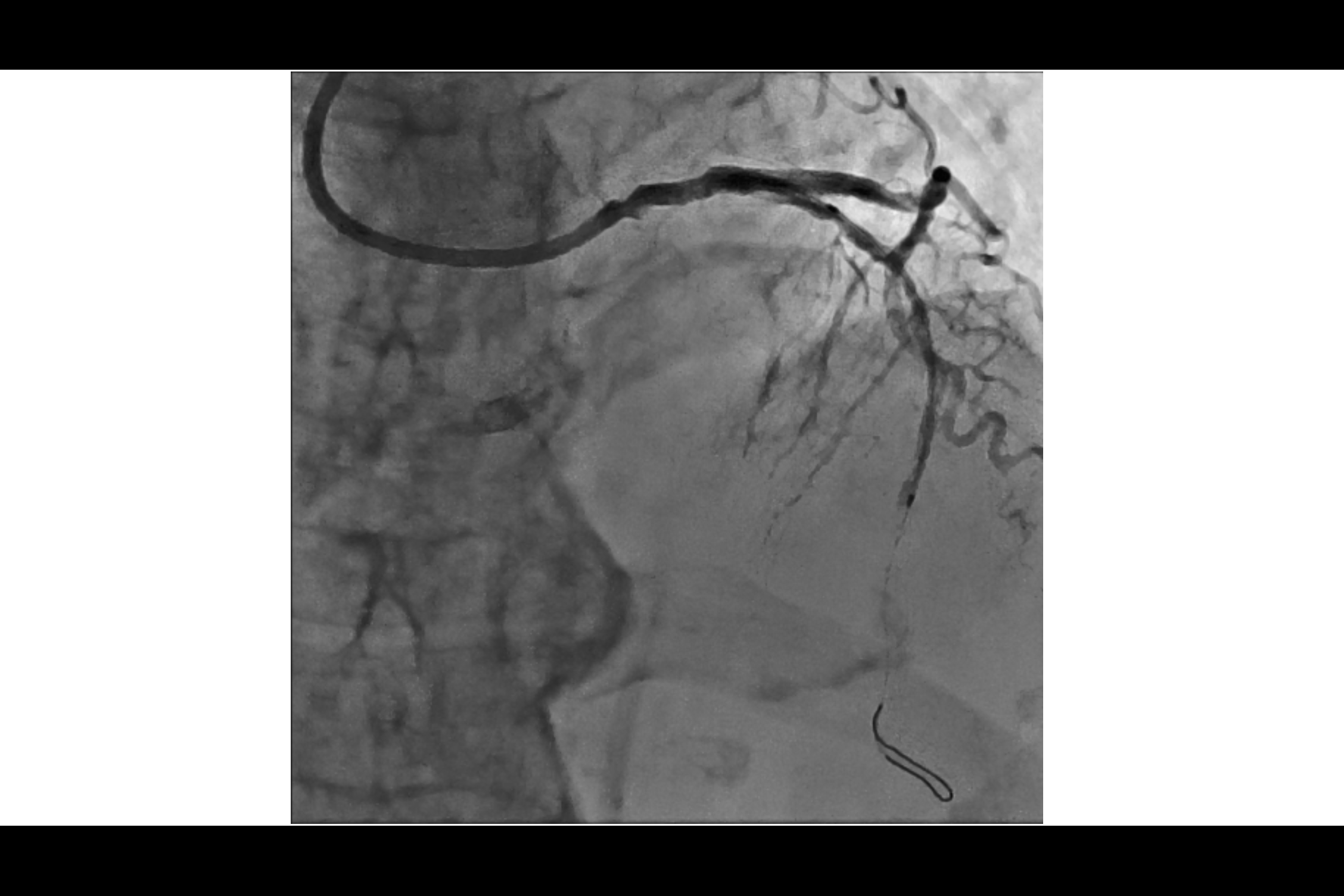
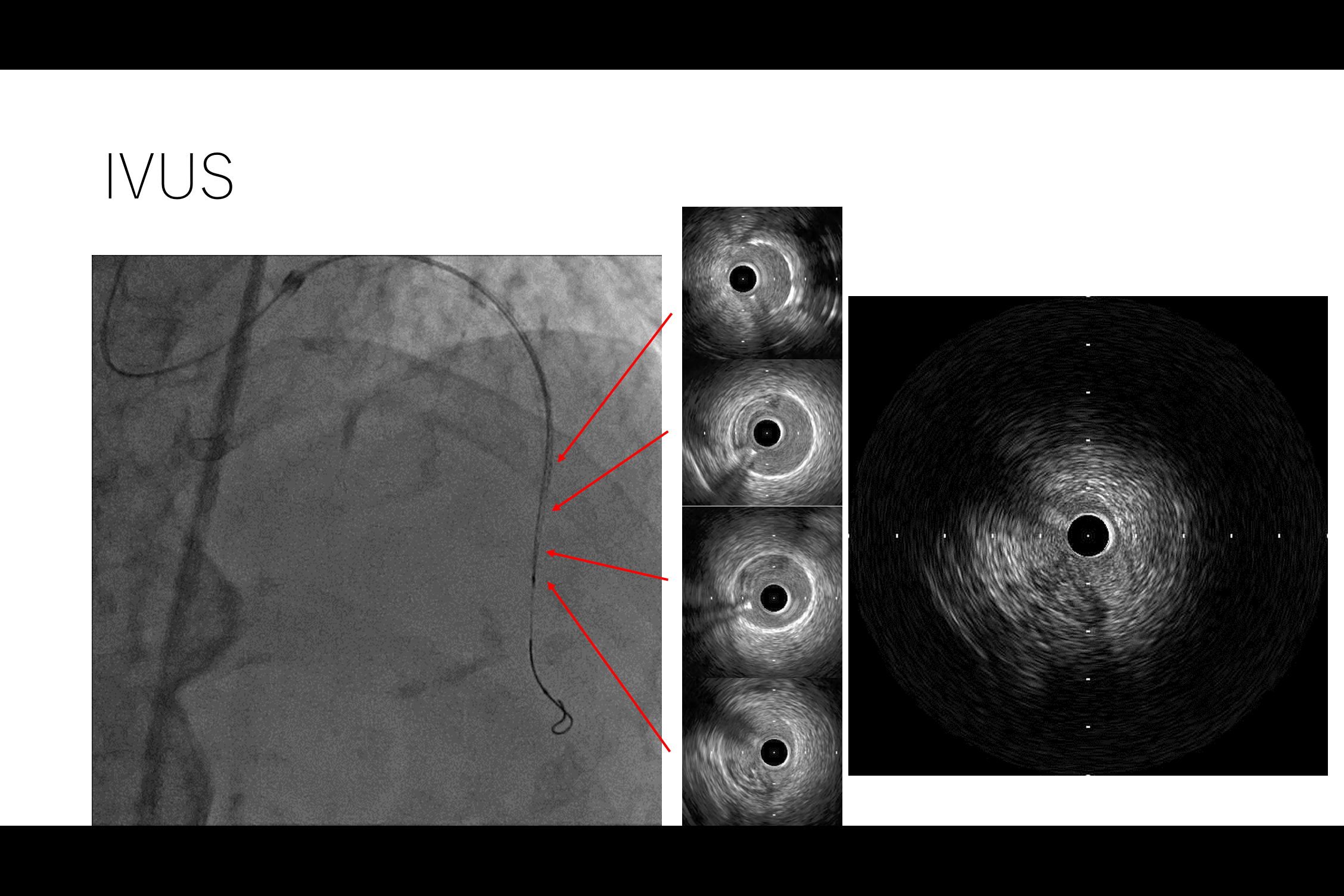
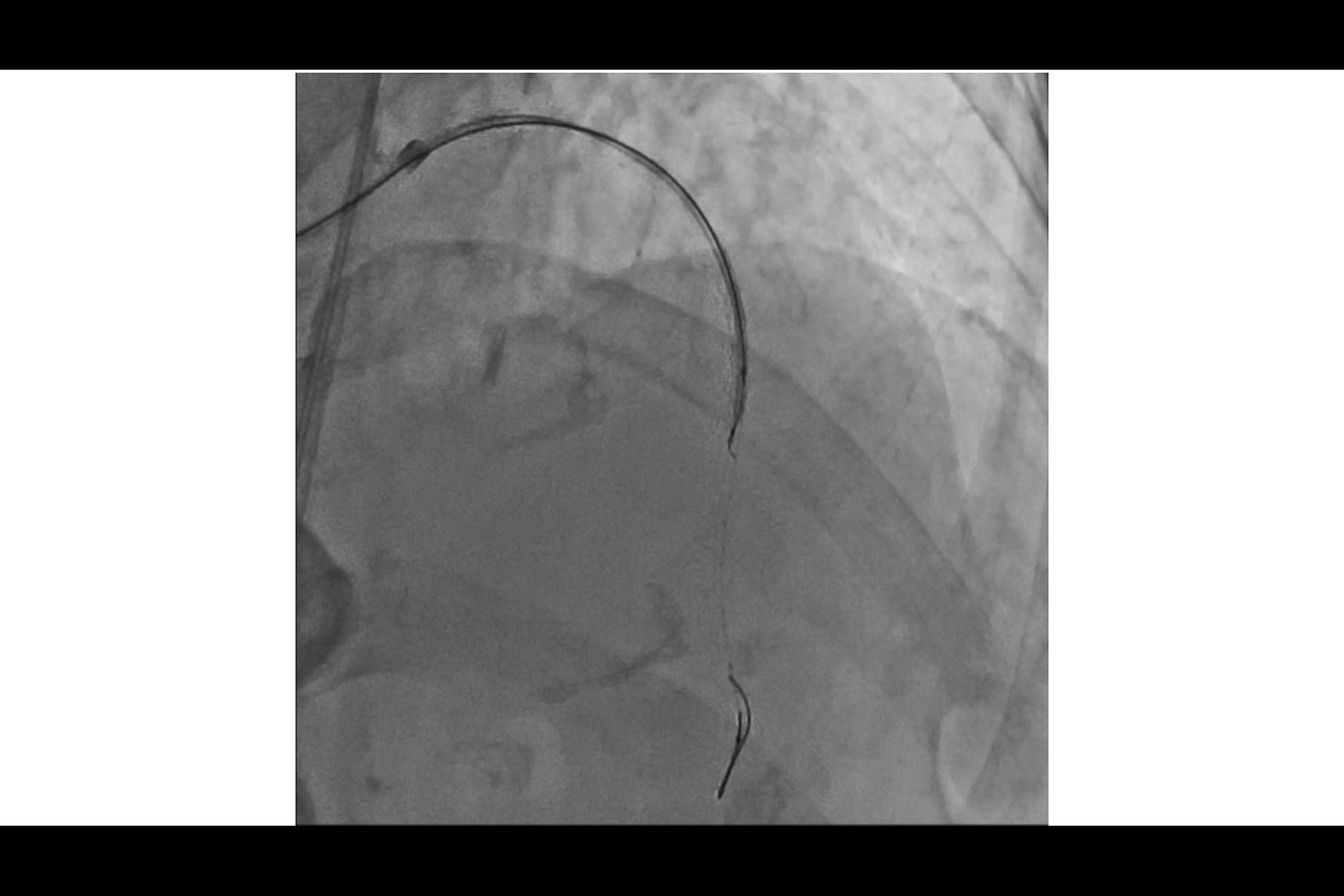
As planned preoperatively, the lesion was balloon dilated and a stent was attempted to be placed, but the wire came out.The wire was reinserted and the stent was placed.There was no flow, and the patient experienced chest pain.Observation of the lesion with IVUS revealed that the stent had been placed in the subintima.In order to bail out, it was necessary to check the status of the collateral circulation from the RCA, but this was difficult due to the anomaly of origin.In this case, the only option was antegrade, so IVUS guide Tip detection ADR was performed and the wire had to be returned from the false lumen to the intimal space.An 8Fr sheath was inserted into the right femoral artery, and the true lumen was able to be returned to the IVUS guide using the Conquest Pro12ST.
Case Summary
As a fundamental premise, IVUS should have been chacked at the moment the wire came out.
In this case, LAD was occluded, and a bailout was necessary.
Collateal sause chack was important, but due to the origin anomaly, the only option was IVUS guide TDADR.
Stenting was performed for a spiral dissection of an open vessel, followed by a bailout using IVUS guide TDADR.
In this case, LAD was occluded, and a bailout was necessary.
Collateal sause chack was important, but due to the origin anomaly, the only option was IVUS guide TDADR.
Stenting was performed for a spiral dissection of an open vessel, followed by a bailout using IVUS guide TDADR.