
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-028
Primary PCI in Anomalous Coronary Artery
By Goutam Datta, Ahana Dutta, Dharmendra Kumar
Presenter
Goutam Datta
Authors
Goutam Datta1, Ahana Dutta2, Dharmendra Kumar1
Affiliation
Institute of Post Graduate Medical Education and Research, India1, NRS Medical College, India2,
View Study Report
TCTAP C-028
Coronary - ACS/AMI
Primary PCI in Anomalous Coronary Artery
Goutam Datta1, Ahana Dutta2, Dharmendra Kumar1
Institute of Post Graduate Medical Education and Research, India1, NRS Medical College, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 55-year-old lady presented with acute chest pain for 4 hrs. She was also having shortness of breath, diaphoresis, dizziness. Her blood pressure was 90/60. Pulse rate was 46/min.She was nondiabetic, her renal function was normal. EKG showed ST/T elevation in lead 2, 3, aVF with complete heart block. Her ejection fraction was 40% with inferior wall hypokinesia in echocardiography. She was planned for Primary PCI.
Relevant Test Results Prior to Catheterization
Her HB was 12.8 Gm.Random blood sugar was 108 mg%. Her serum creatinine was 1.1. Chest Xrayrevealed no abnormality. EKG---Acute inferior wall myocardial infarction withcomplete heart block.
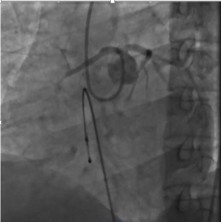
Relevant Catheterization Findings
Coronary angiography was done from right radial route. Temporary pacemaker was placed from right femoral vein. Coronary angiogram revealed normal Left main, Left anterior descending artery and Left circumflex artery. We could not find right coronary artery (RCA). She had total occlusion of Right coronary artery from proximal part. But RCA was originating from left coronary sinus instead of right coronary sinus. Judkin right 4 was used to cannulate right coronary artery which is originating from left coronary sinus just opposite to left main coronary artery.
Interventional Management
Procedural Step
Primary PCI was done by radial route. 6F Left Judkin guide catheter was taken. It was placed in left coronary sinus. Then it was pushed and rotated in such a way that it can hook right coronary artery ostium. Left coronary ostium was from opposite wall. Right coronary ostium was engaged with lot of difficulty. Coronary floppy guidewire was used to cross the lesion following “Go With Flow” technique. Then lesion was predilated by semicompliant balloon 2.5 x 10 at 8 atm.
3.5 x 24 mm drug eluting stent was deployed in culprit lesion AT 14 atm and it was post dilated by 3.5 x 20 non compliant balloon at 16 atm. TIMI 3 flow was restored. Patient became pain free and came back to sinus rhythm after two hours.


3.5 x 24 mm drug eluting stent was deployed in culprit lesion AT 14 atm and it was post dilated by 3.5 x 20 non compliant balloon at 16 atm. TIMI 3 flow was restored. Patient became pain free and came back to sinus rhythm after two hours.
Case Summary
Congenital coronary artery anomalies are found in 0.2% to 1.2% of patients undergoing percutaneous coronary intervention. Unusual origin and course of an anomalous coronary artery can cause technical challenges during interventional procedure and may lead to use of large iodinated contrast volumes, high radiation exposure. Anomalous origin of a coronary artery may erroneously be interpreted as totally occluded culprit vessel in ST elevation myocardial infarction. Aortic root angiogram in two orthogonal view will help to identify origin of anomalous coronary Artery. Conventional use of catheters to locate abnormal origin will cause delay in acute coronary syndrome patients where time is of paramount importance. Computed tomographic angiography can provide rapid and accurate information regarding the origins and course of the coronary arteries and it’s a preferred approach in non acute coronary syndrome patients. Incidence of right coronary artery arising from left coronary sinus is around 0.23%. An anomalous right coronary artery can arise from different locations within the sinuses of Valsalva. Special catheters are required to engage anomalous artery.A) RCA ostium adjacent to left main coronary artery ostium---most common and technically challenging. Preferred catheters are Left Amplatz (45 or 90degree) or Left sided extra back up catheters for selective engagement.B) RCA ostium inferior to left main coronary artery ostium--- Left Amplatz (1/2/3) or right Amplatz (1,2,3) catheters are useful guide for cannulation. C) RCA ostium toward the commissure of the right and left cusp---Left Amplatz (1/2/3) or right Amplatz (1,2,3) catheters are useful. D) RCA ostium above the sinotubular plane---Judkins 4 right catheter, hockey stick, multipurpose, Amplatz left or right are helpful for selective cannulation. E) RCA ostium from right cusp superior and toward the left cusp---Options are 3DRC, Amplatz left or right, Sherpa NX Balanced.Wiring may be difficult. “Go with Flow” is a useful technique for wiring anomalous coronary artery. Balloon and Stent delivery may be difficult at times when balloon anchoring/trapping methods may be helpful. We have used Judkin right 4 guidecatheter to cannulate right coronary artery originating just opposite Left main coronary artery in an unconventional way. Right coronary artery originating from Left coronary sinus may have interarterial course between Left main and pulmonary artery which can cause ishaemia and sudden cardiac arrest during exercise. It may have slit like ostium, the acute take off angle, the proximal narrowing (also referred to as hypoplasia) and intramural course (within tunica media of the aortic wall). These are high risk features for ischaemia and sudden cardiac arrest during exertion. Percutaneous intervention in these group are also more prone to have dissection and restenosis.