
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-091
Walking on the Edge of Unseen Dangers: Retrograde Wiring Through Left Main Subintima in an Ostial LAD CTO
By Nattapong Thaiyanurak, Thanyalak Chotayaporn, Noparat Oniem, Noparat Thanachaikun
Presenter
Nattapong Thaiyanurak
Authors
Nattapong Thaiyanurak1, Thanyalak Chotayaporn1, Noparat Oniem1, Noparat Thanachaikun1
Affiliation
Nakornping Hospital, Thailand1,
View Study Report
TCTAP C-091
Coronary - Complex PCI - CTO
Walking on the Edge of Unseen Dangers: Retrograde Wiring Through Left Main Subintima in an Ostial LAD CTO
Nattapong Thaiyanurak1, Thanyalak Chotayaporn1, Noparat Oniem1, Noparat Thanachaikun1
Nakornping Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
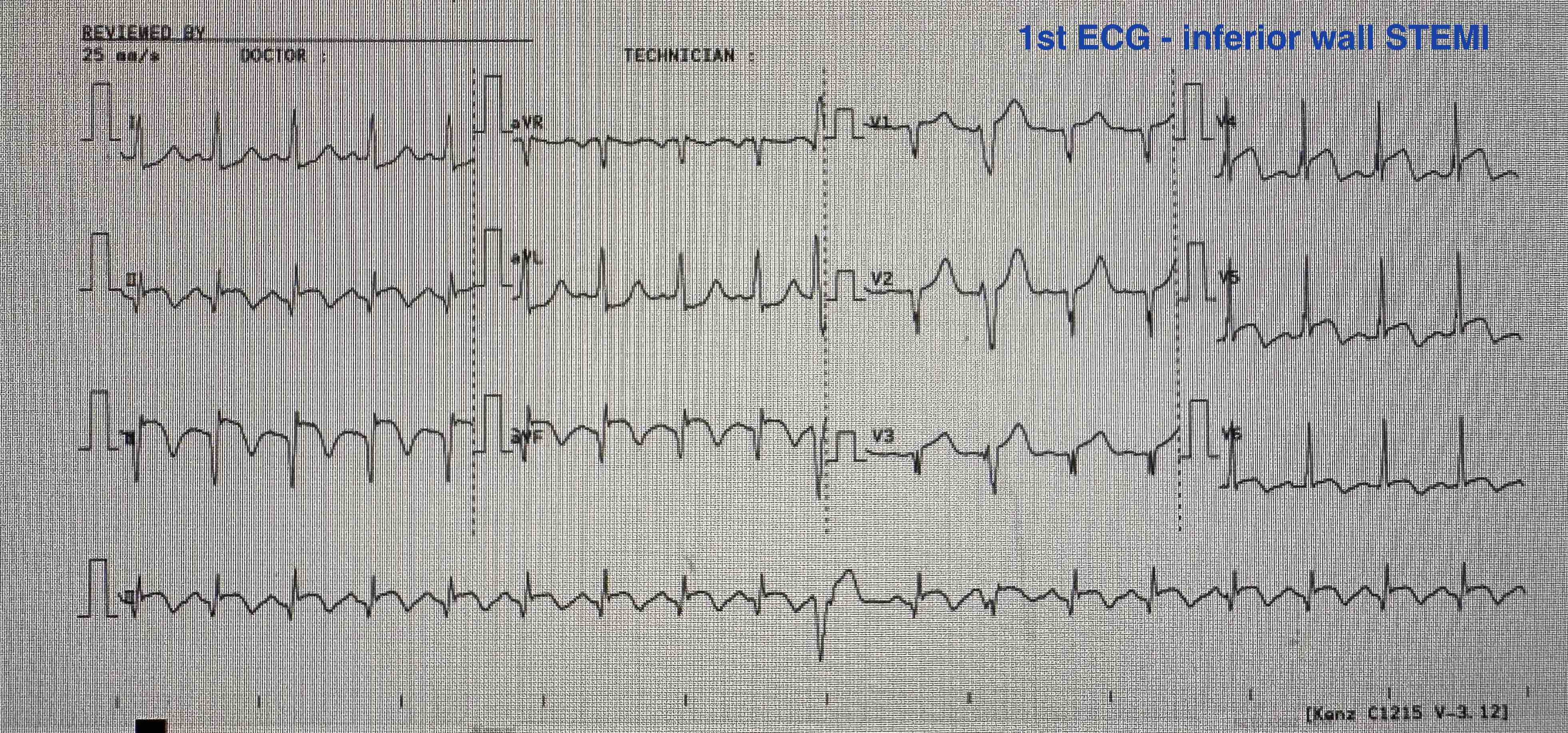
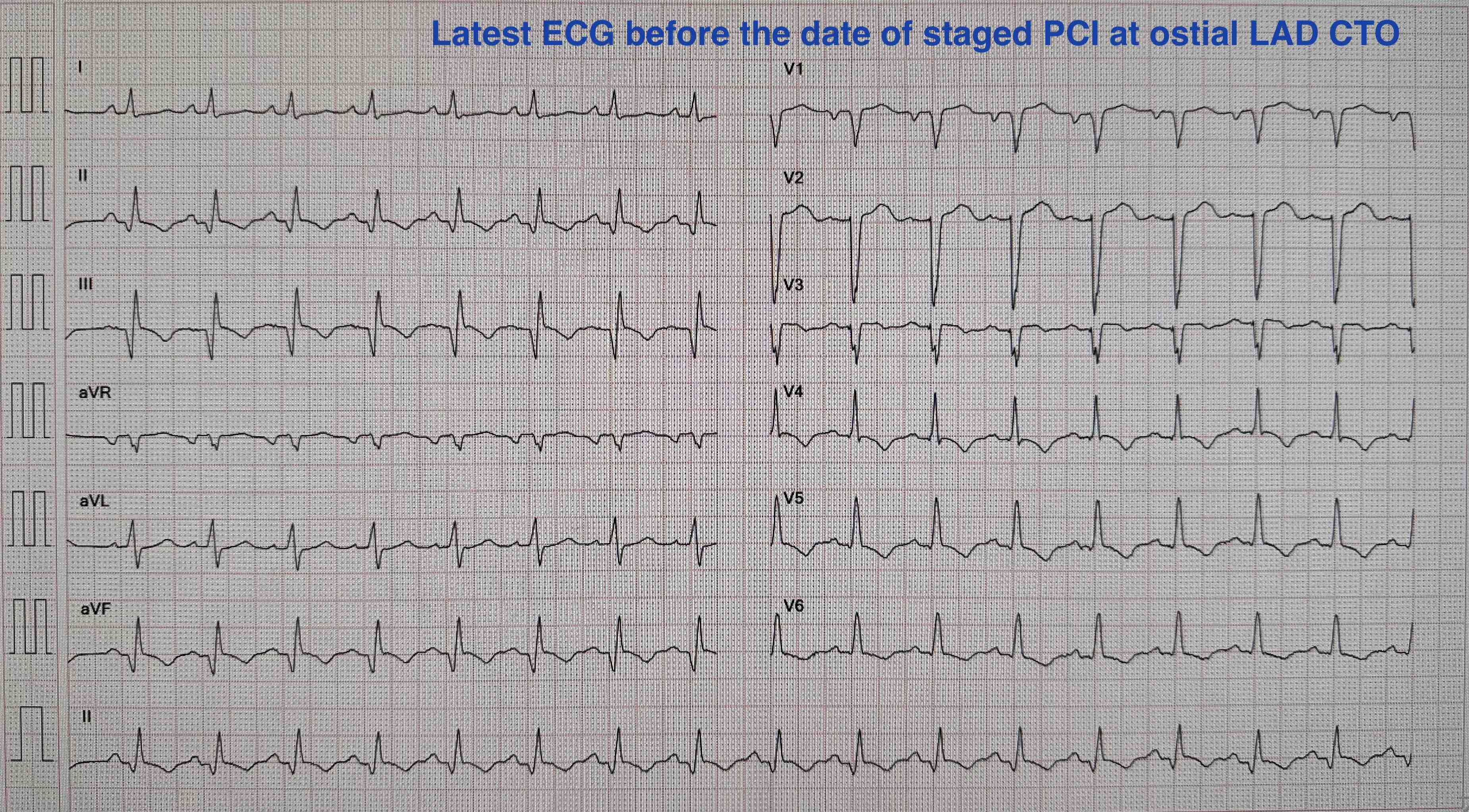
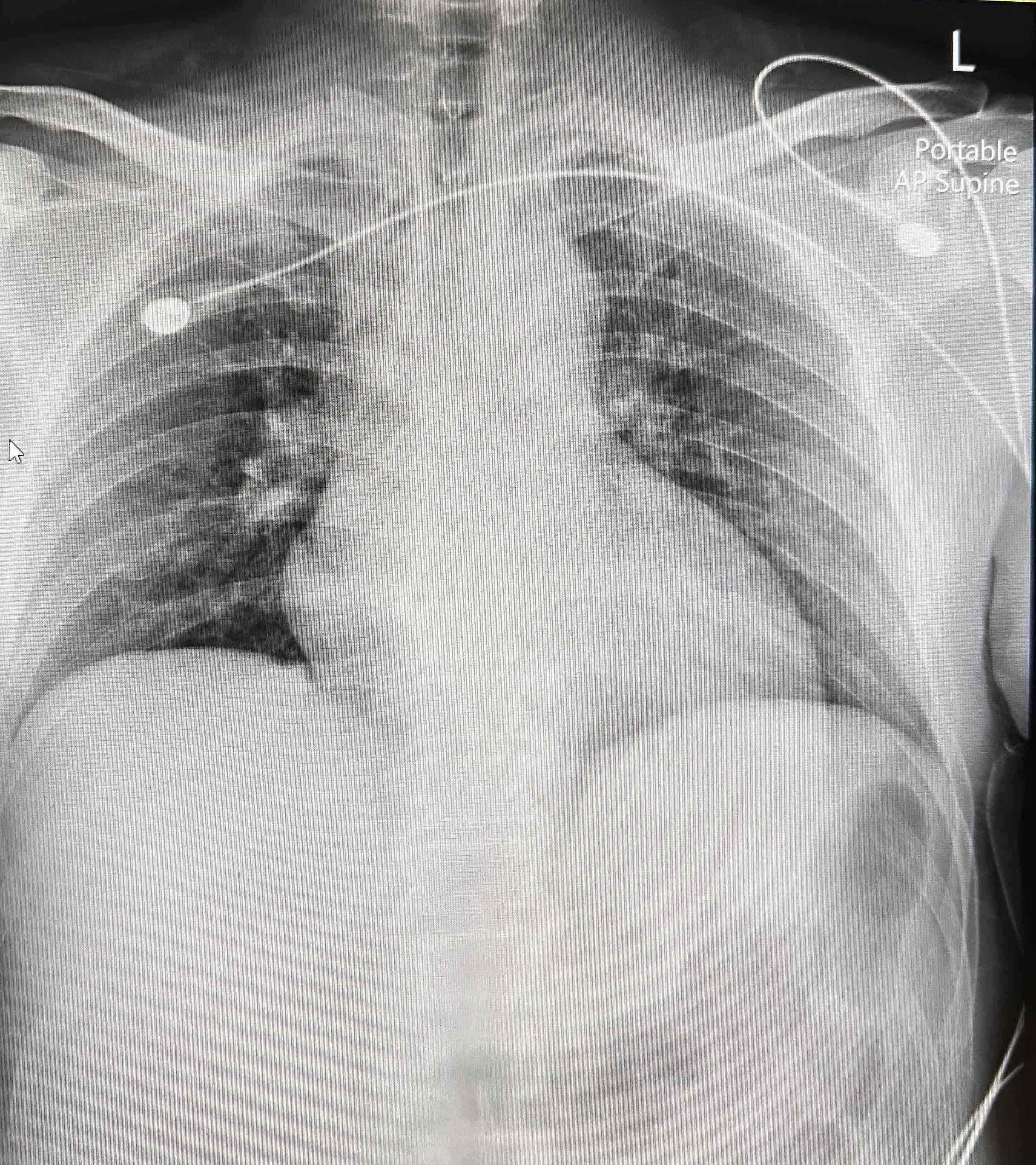
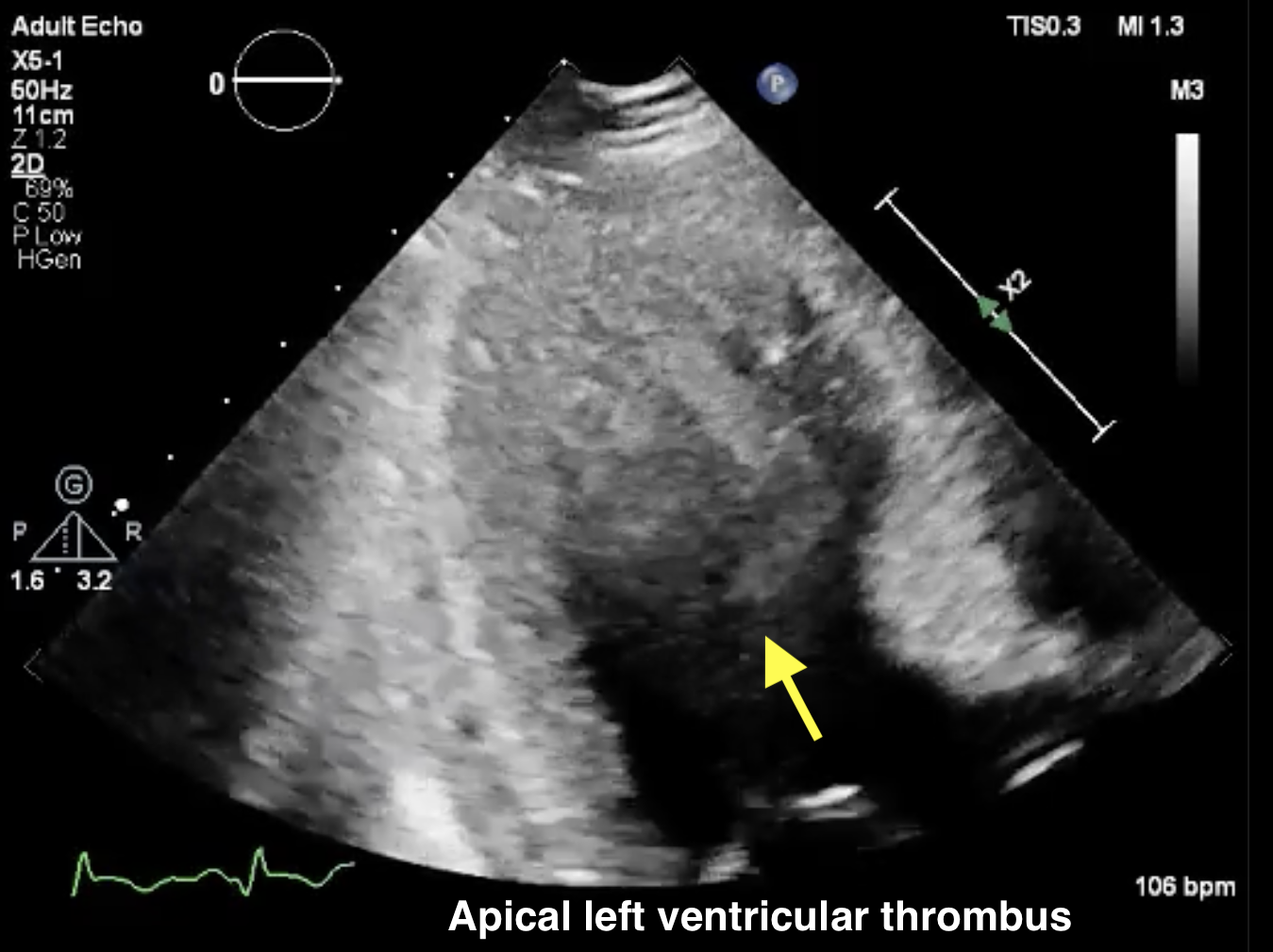
A 40-year-old Thai male with hypertension, dyslipidemia & active smoker presented with an inferior wall STEMI. He underwent primary PCI/DES to the RCA (IVUS-guided) & was scheduled for staged PCI of an ostial LAD CTO 1 month later. He was on warfarin for an apical LV thrombus detected during his STEMI admission. While awaiting the procedure, he experienced recurrent heart failure twice at a rural hospital. On the staged PCI date, physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
- Echo: LVEF 38.3%, akinesia at inferior, inferoseptal, anterior & anteroseptal wall, apical LV thrombus, no significant valvular heart disease- Serum creatinine 1.17 mg/dL (eGFR 60.6 ml/min/1.73sqm)- Hematocrit 42.3%, Hemoglobin 14.2 g/dL, Platelet 224,000/uL- Prothrombin time 18.4 seconds, INR 1.61- Total cholesterol 203 mg/dL, Triglyceride 171 mg/dL, HDL 23 mg/dL, LDL 132 mg/dL
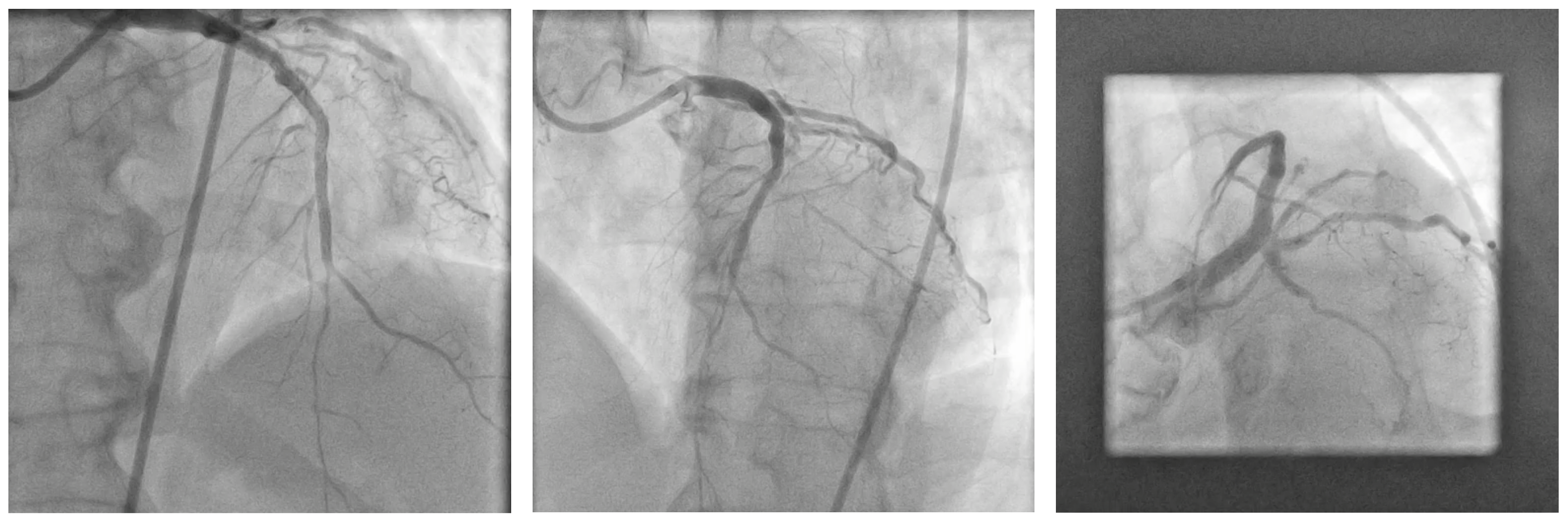
Relevant Catheterization Findings
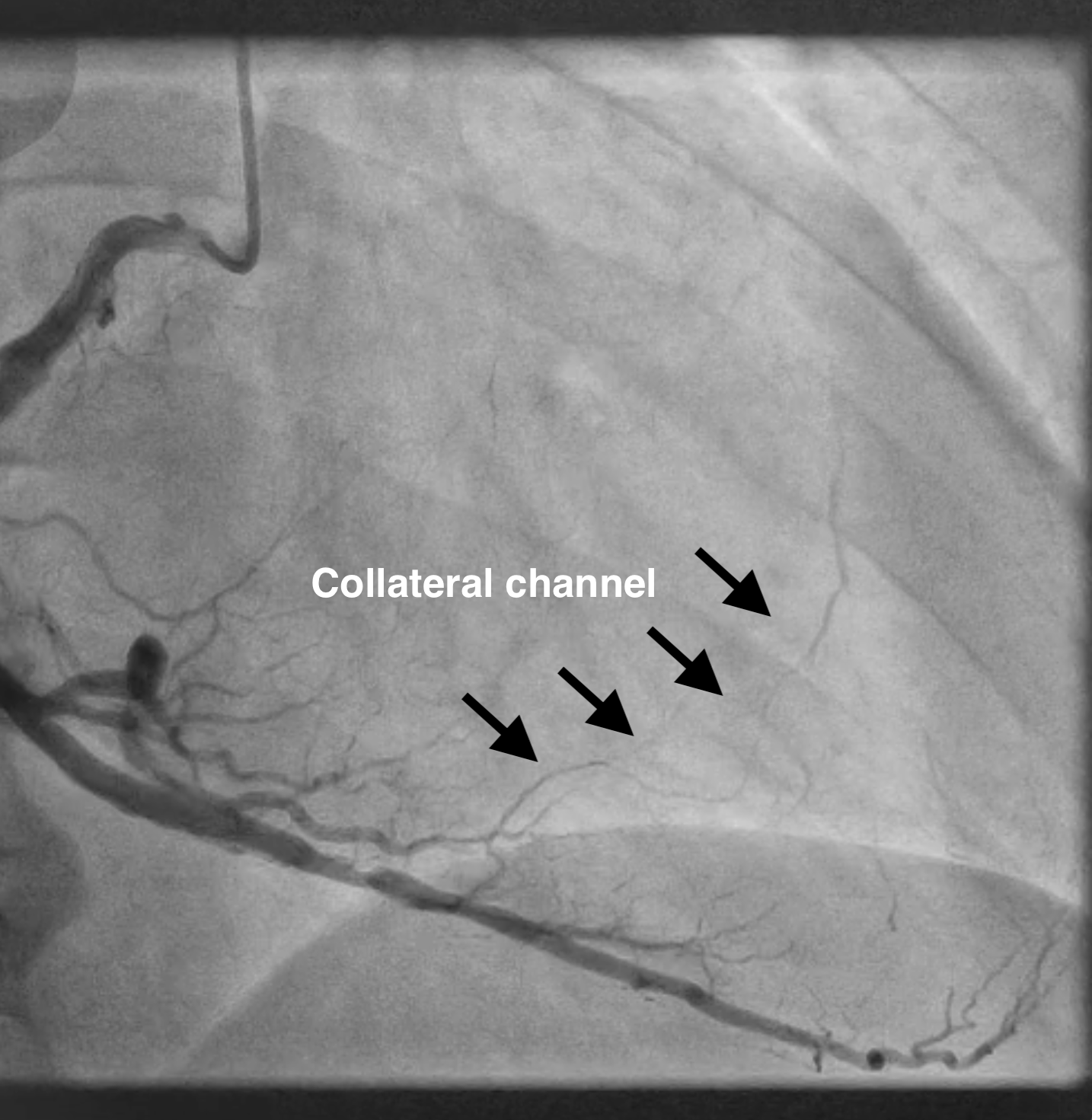
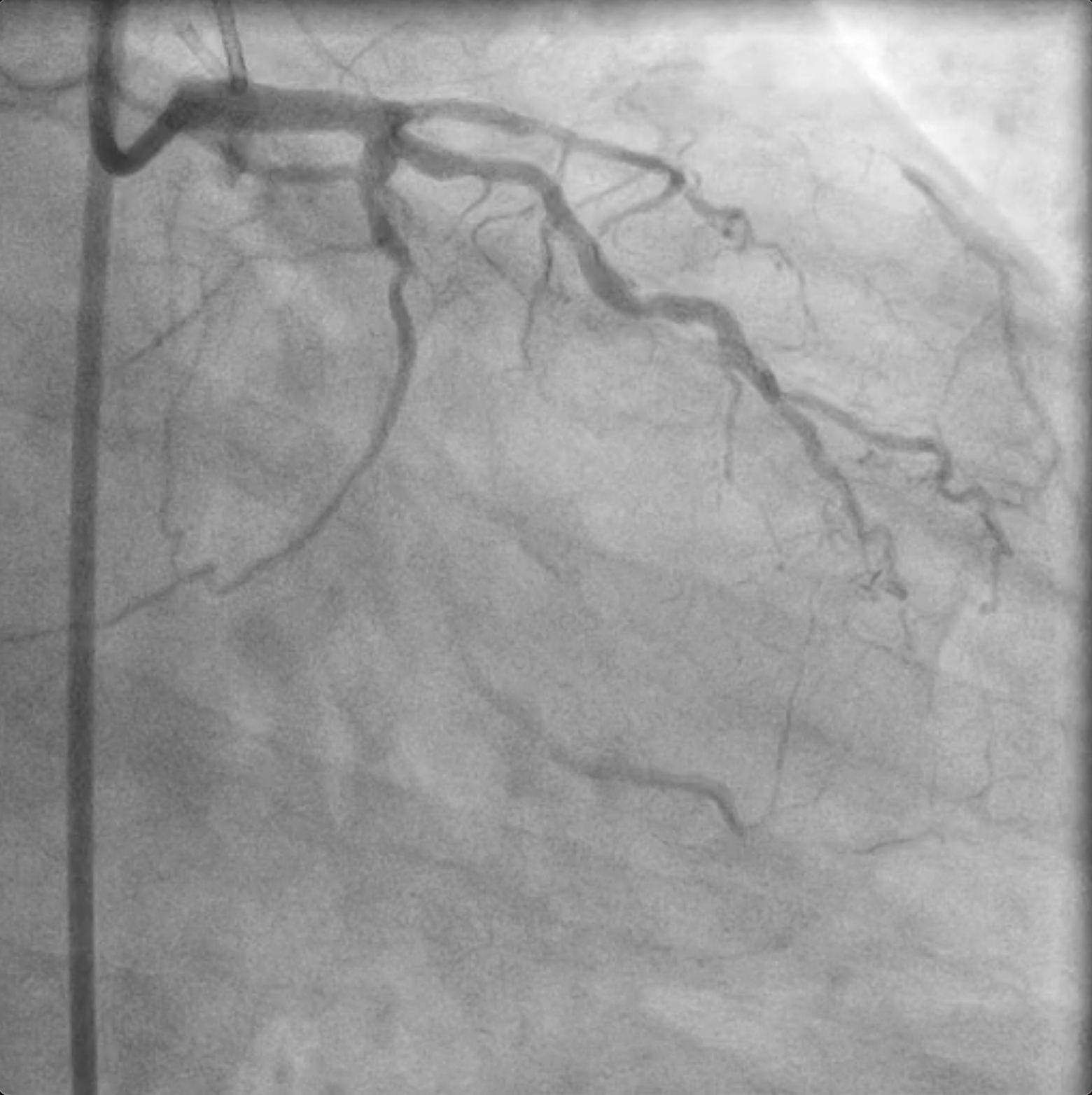
Coronary angiogram- LM: normal- LAD: CTO from the ostial LAD to mid-LAD, suitable for PCI (J-CTO score 3). Diffuse 90% stenosis at the distal LAD. Total occlusion at the ostial first diagonal (DG) branch.- LCX: CTO at the proximal LCX and first obtuse marginal (OM) branch. The ramus branch supplies collateral vessels to the first OM and D1 branches.- RCA (right dominant): Patent stents in the RCA. The RCA supplies collateral vessels to the CTO in the LAD.

Interventional Management
Procedural Step
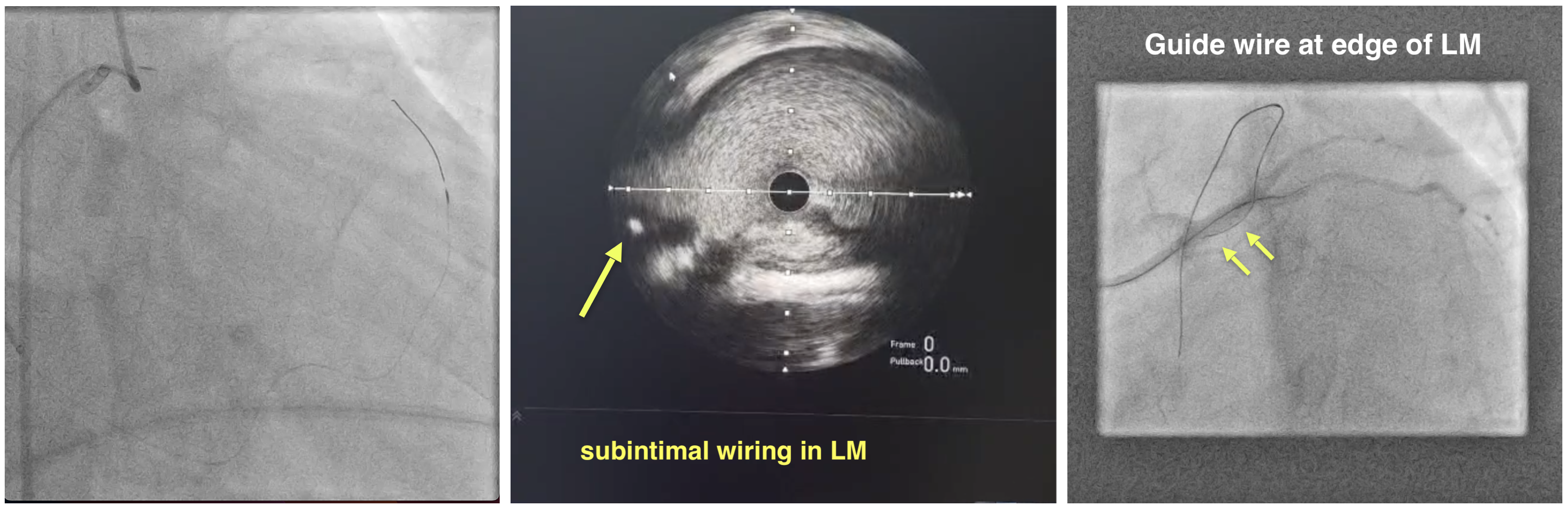
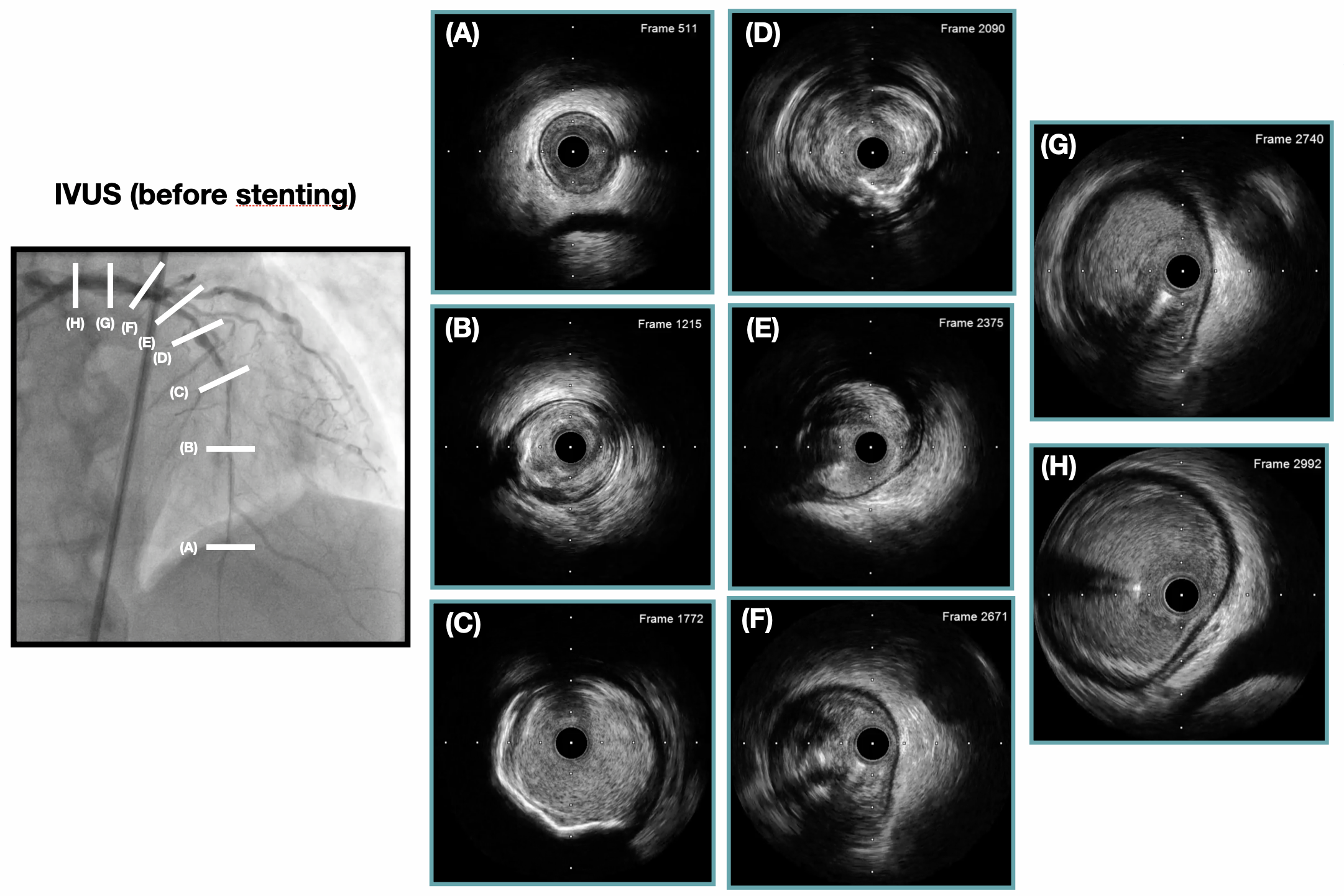
Access site: RFA & RRA approach/ Guiding catheter: RBU 3.5 6F & EBU 3.5 7F. Due to unclear proximal cap of the ostial LAD CTO & the presence of satisfactory collateral channels from RCA, a retrograde approach was selected. A Sion Blue guidewire (GW) with a Caravel microcatheter was advanced into the initial segment of the septal channel via RPD. Subsequently, a SUOH GW was advanced through the septal channel to the distal cap of the CTO using the balloon-assisted tracking technique to facilitate guide extension catheter delivery. Fielder XTR, Gaia Next 1, and Gaia Next 2 guidewires were used sequentially to penetrate the proximal cap & pass into the LM. However, multiple attempts at advancing the retrograde GW into the antegrade microcatheter using the Rendezvous technique were failed. Angiogram revealed the GW's location at the edge of the LM. IVUS imaging delivered into the ramus branch confirmed subintimal wiring in the LM. IVUS-guided CTO tip identification was employed to achieve successful antegrade wiring through the CTO segment. The lesion was pre-dilated using balloons (1.0 × 5 mm, 2.0 × 20 mm) and a scoring balloon (3.0 × 15 mm) to address the calcified proximal LAD segment. Biomatrix Alpha stents (2.5 × 36 mm, 3.0 × 24 mm & 4.0 × 29 mm) were deployed from the mid LAD to LM. POBA was performed in the distal LAD due to the small vessel size. Post-dilation with non-compliant balloons was guided by IVUS. Final IVUS & angiogram showed good result.
Case Summary
- Subintimal wiring in the left main (LM) during retrograde wiring requires caution to avoid subintimal PCI and abrupt LM closure when crossing the ostial LAD CTO segment. - Intravascular imaging, particularly wire tip identification, is crucial for procedural success in cases with ambiguous CTO stumps.- Balloon-assisted tracking effectively facilitates guide extension catheter delivery and enhances support for retrograde wiring. - 1 month post-PCI of the LAD CTO, staged PCI of the LCX CTO was successfully performed. Follow-up angiography showed patent stents in the LM to mid-LAD, improved distal LAD size, & significant improvement in heart failure symptoms with optimized therapy.