
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-024
Utilizing the Anchor Balloon Technique to Overcome Uncrossable Lesion: A Practical Approach Optimizing PCI Outcomes
By Dede Jumatri Tito, Muhammad Syukri
Presenter
Dede Jumatri Tito
Authors
Dede Jumatri Tito1, Muhammad Syukri1
Affiliation
RSUP Dr. M. Djamil Hospital, Indonesia1,
View Study Report
TCTAP C-024
Coronary - ACS/AMI
Utilizing the Anchor Balloon Technique to Overcome Uncrossable Lesion: A Practical Approach Optimizing PCI Outcomes
Dede Jumatri Tito1, Muhammad Syukri1
RSUP Dr. M. Djamil Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
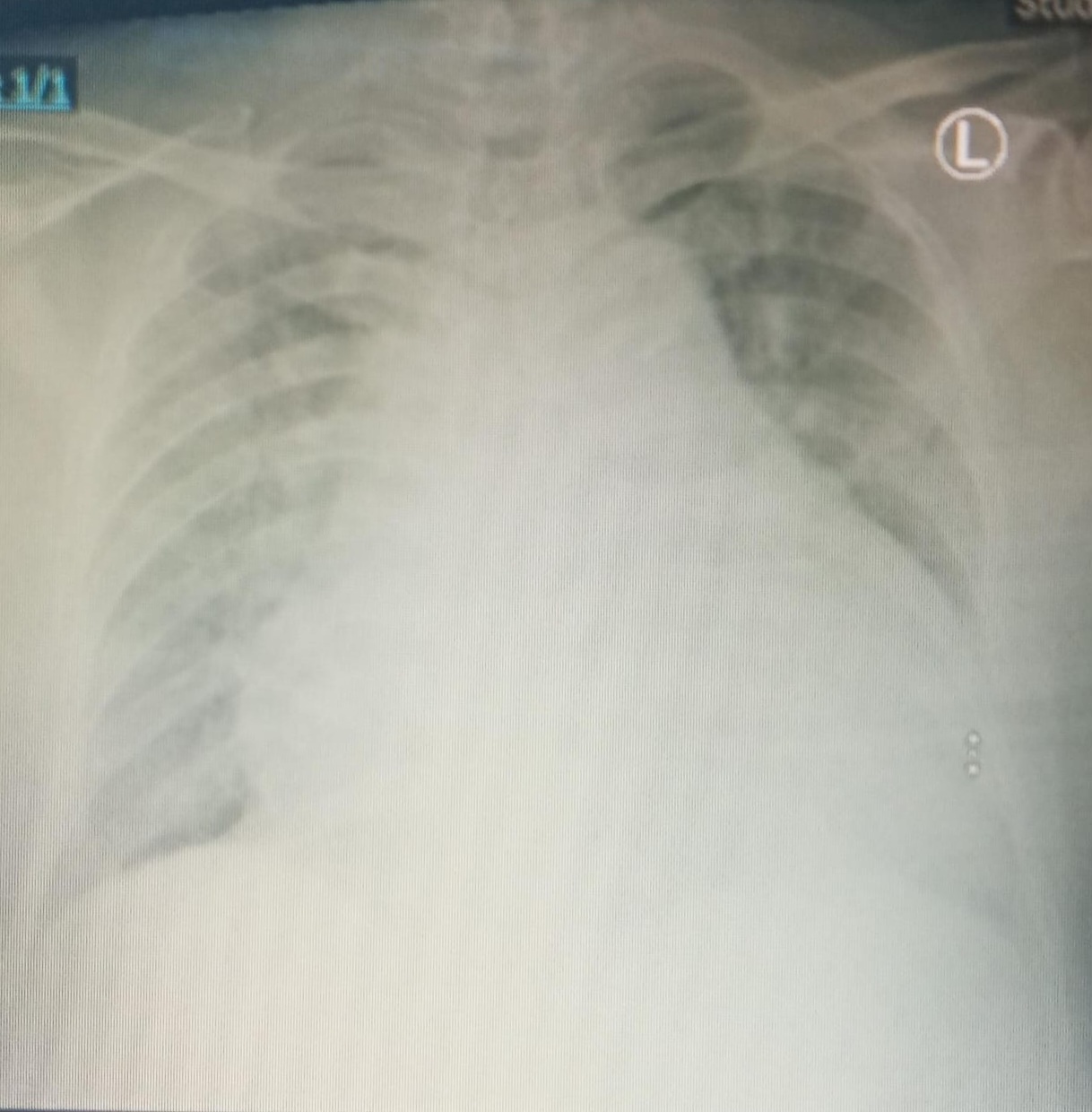
A 75-year-old male, admitted from emergency room with unstable angina pectoris. His cardiovascular risk factors were smoker, hypertension and dislipidemia with previous history of PCI using 1 DES at left main to proximal LAD in 2023. His vital signs upon arrival were blood pressure of 154/92 mmHg and heart rate of 95 bpm. There were no abnormal lung sounds and her peripheral perfusion was normal.
Relevant Test Results Prior to Catheterization
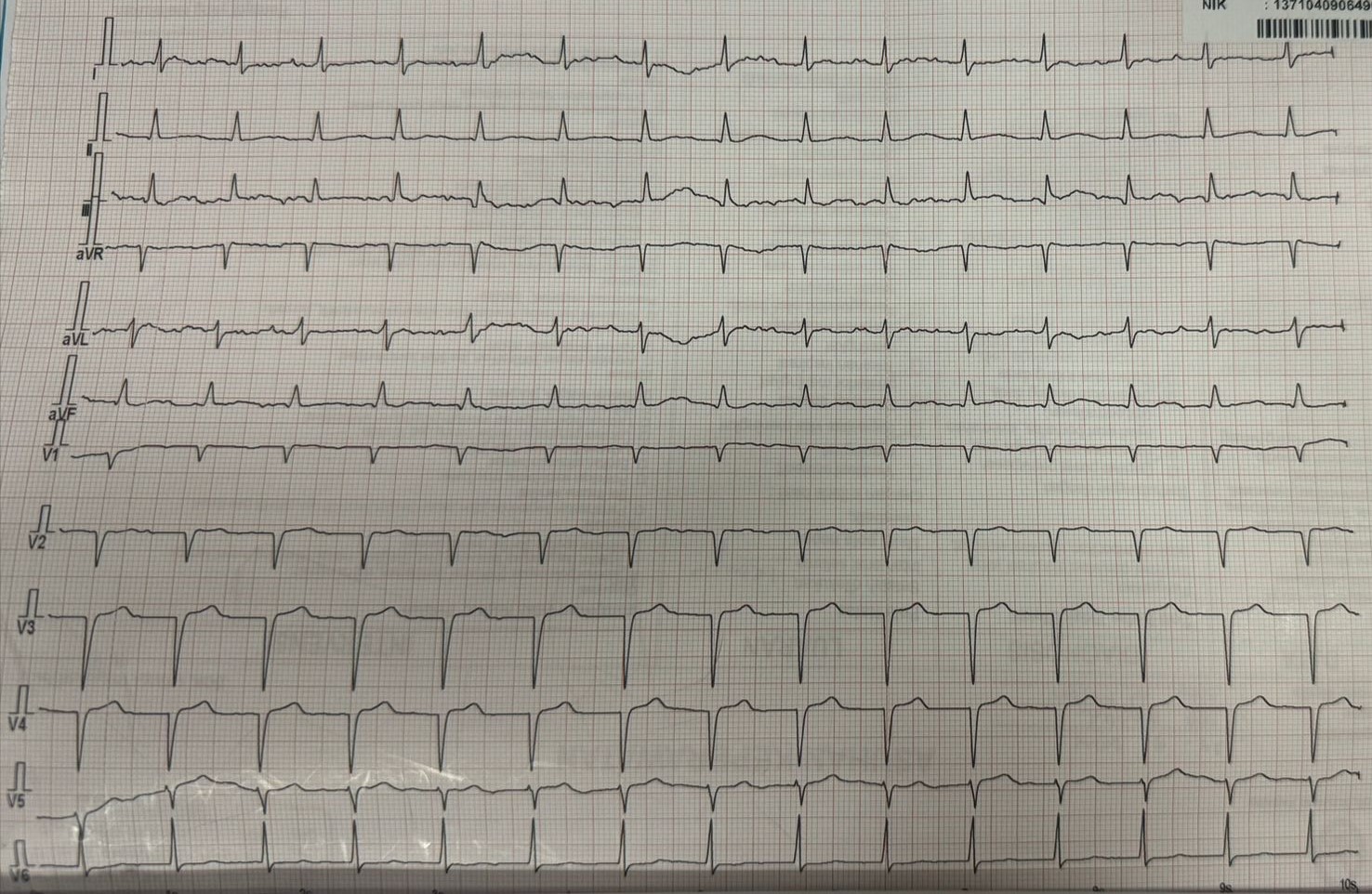
His ECG showednormal sinus rhytm with pathologic Q wave V1-V3. The laboratory findings were withinnormal limit.
Relevant Catheterization Findings
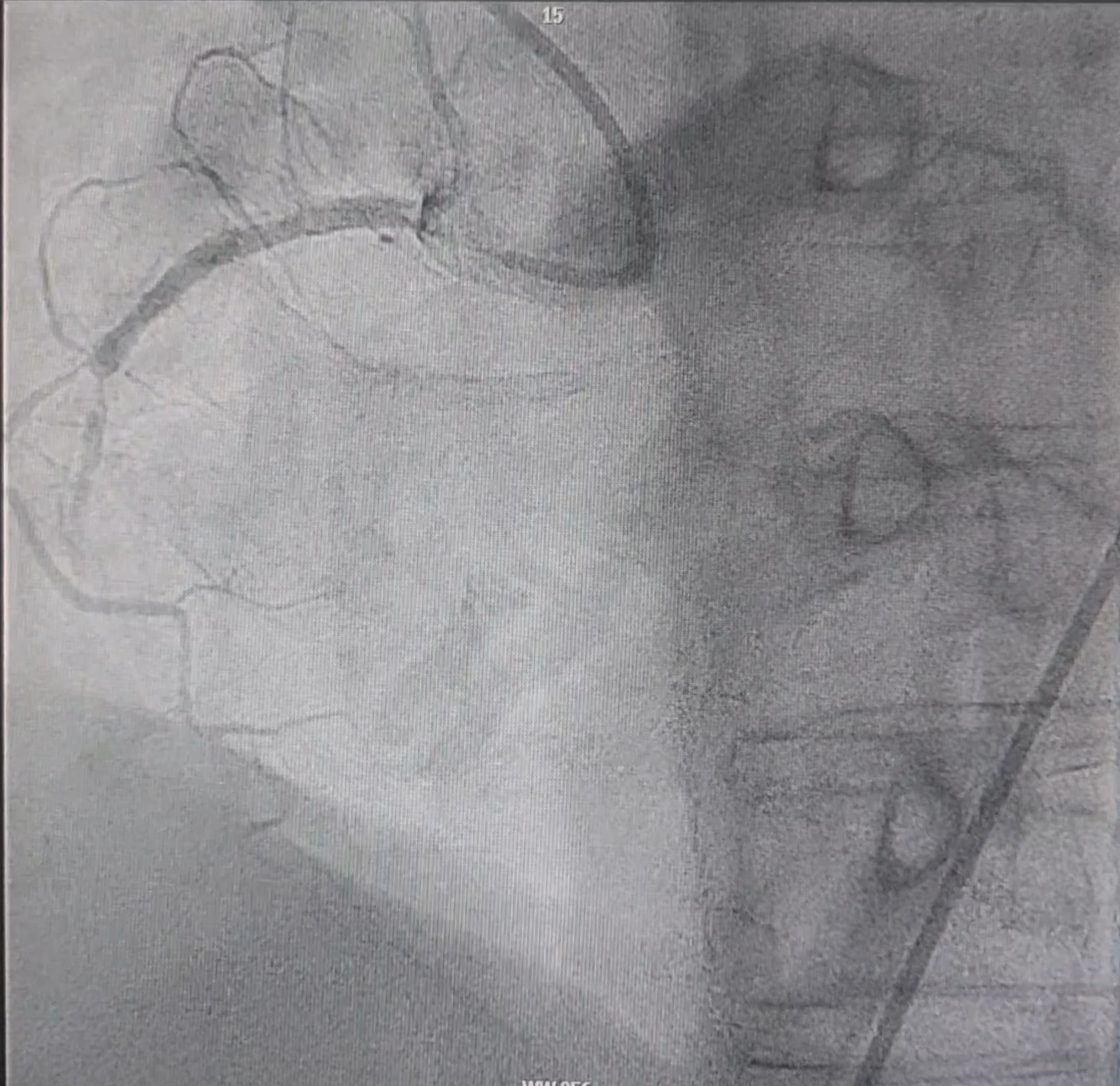
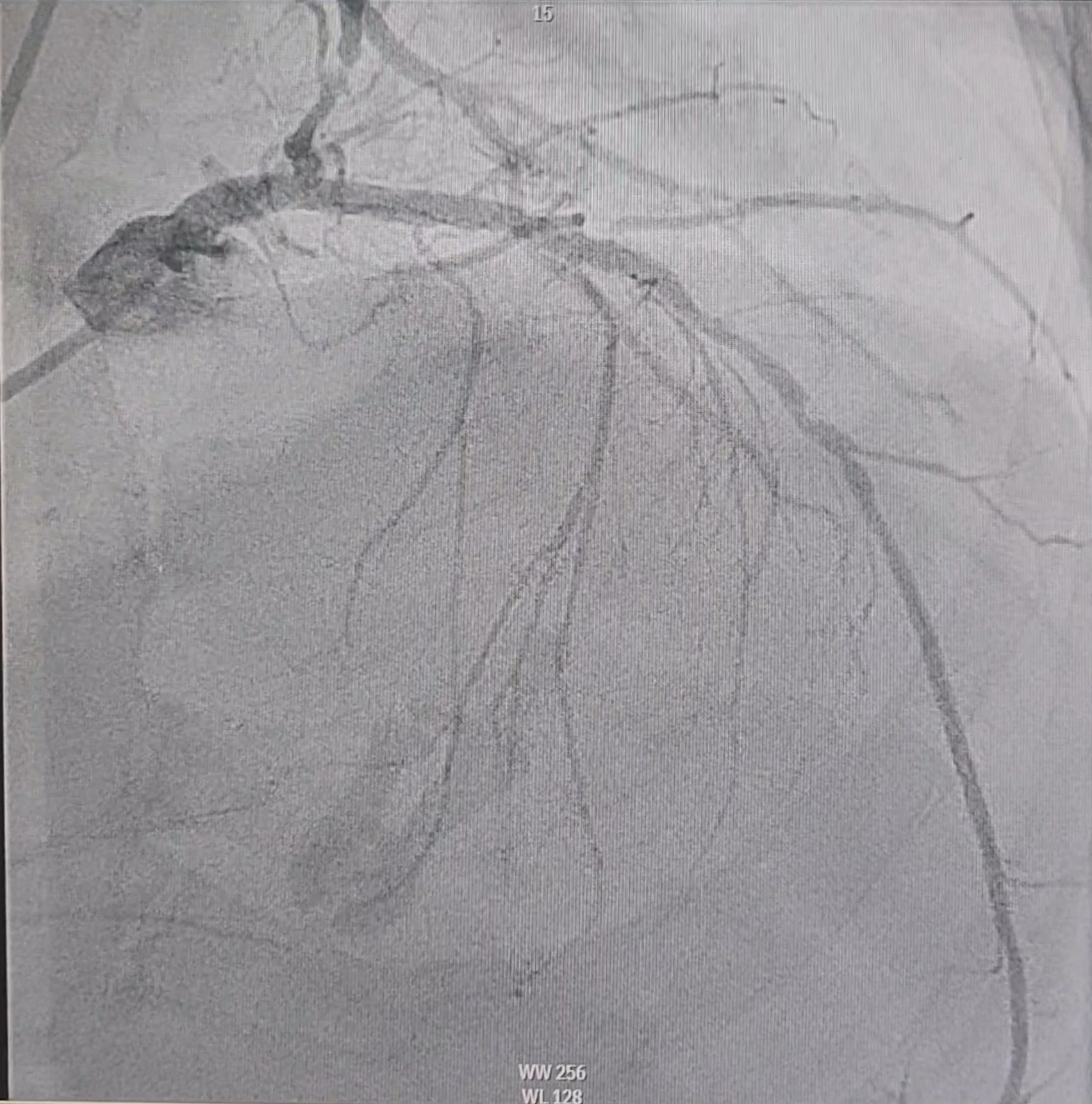
Left coronary angiography showed patent stent in left main – proximal Left Anterior Descending, moderate stenosis in distal Left Anterior Descending, normal Left Circumfex. Right coronary angiography showed subtotal stenosis in mid part.
Interventional Management
Procedural Step
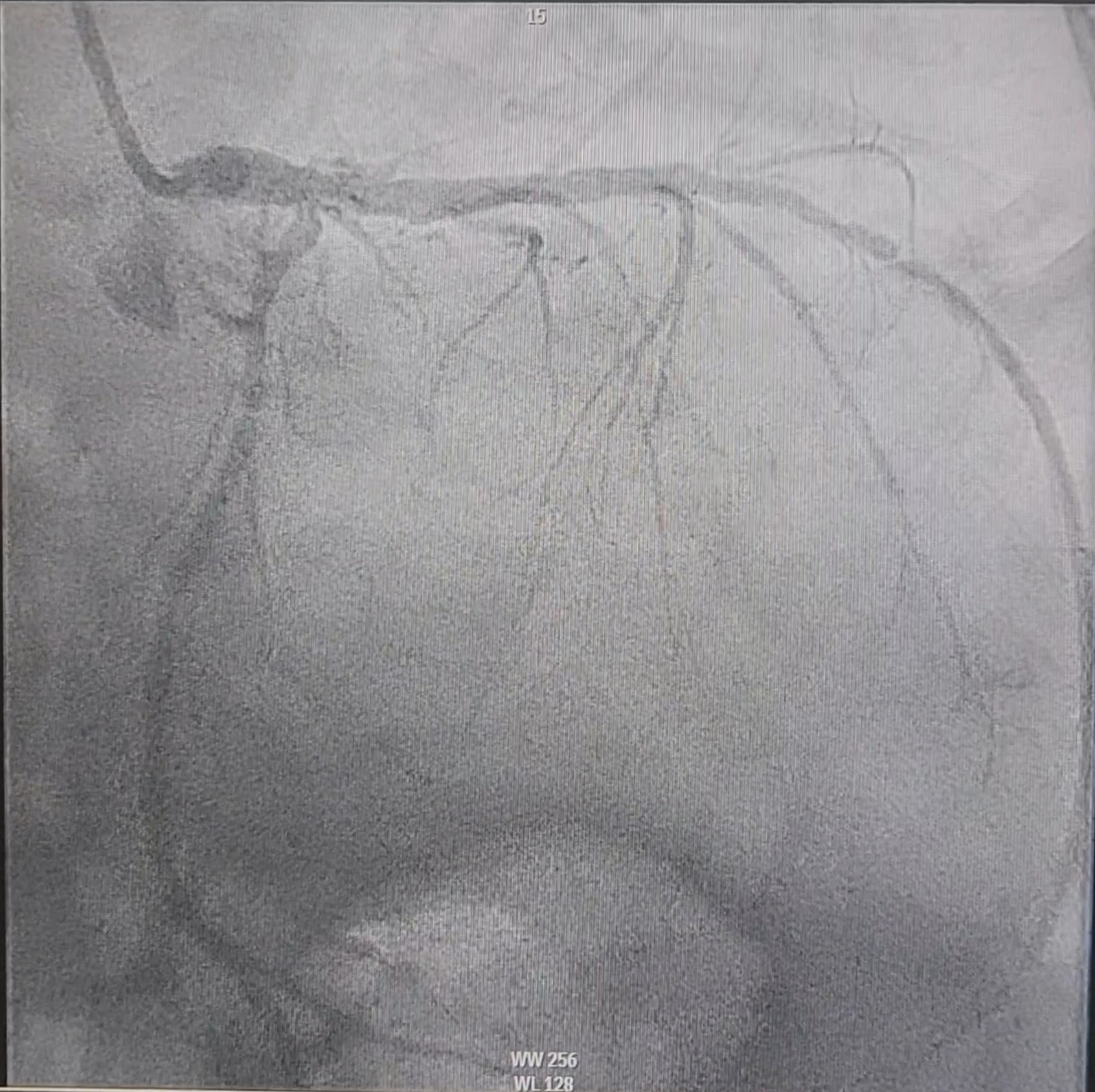
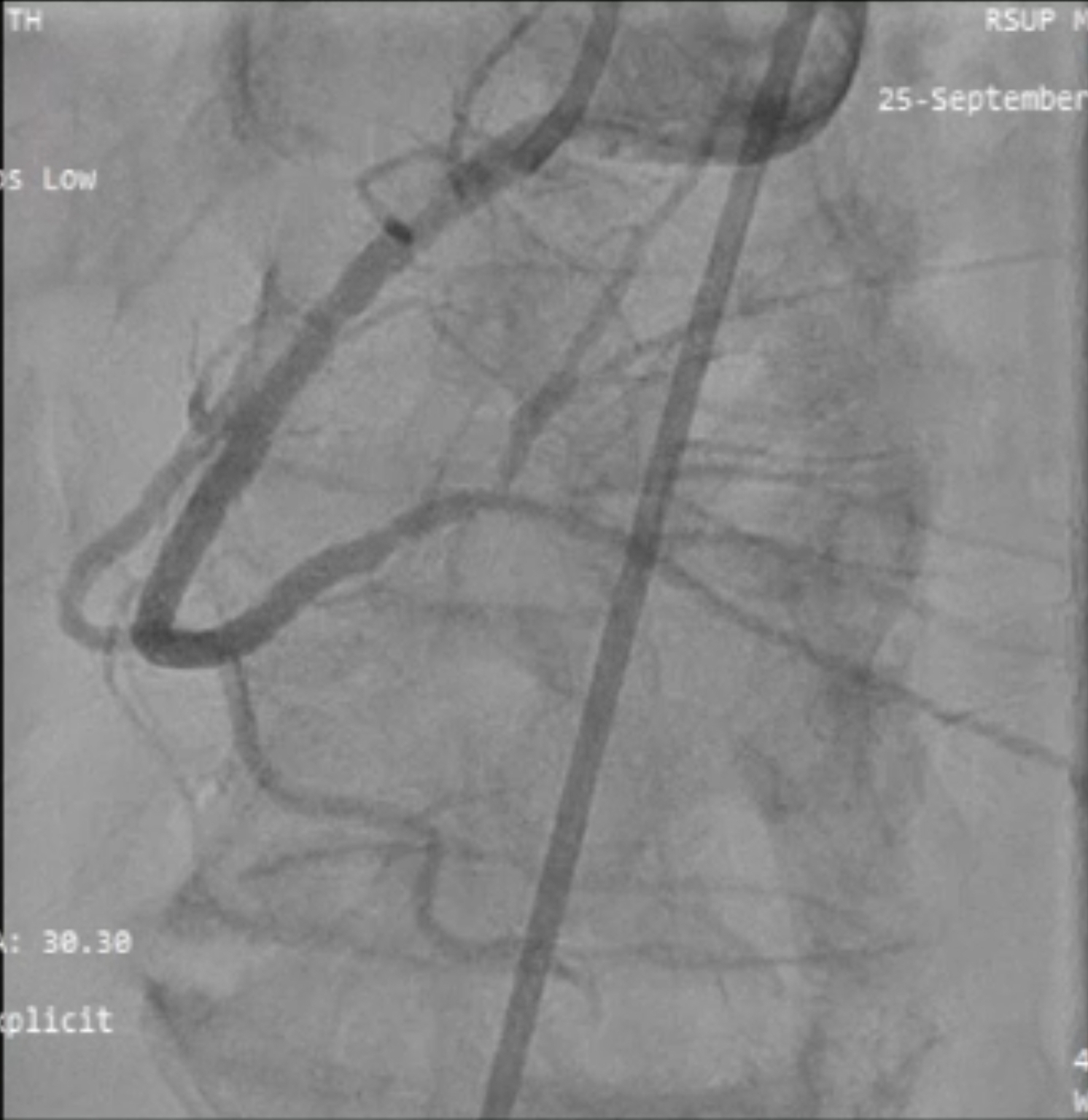
We proceed with PCI of RCA, using JR 3.5/6 F and floppy guidewire. Wire cannot cross the lesion. We tried to optimize wire support with an anchor wire in the RV branch, afterwards the wire can cross the lesion. For lesion preparation, a 1.0 x 10 mm semi-compliance balloon was inflated in the RV branch for the anchor. A 1.5 x 15 mm semi-compliance balloon can cross the lesion and be inflated with 14 atm. Afterwards a 2.0 x 15 mm NC balloon was inflated in the mid-distal RCA. Then a 2.75 x 36 mm DES was implanted in proximal - mid RCA, overlapped with 2.5 x 36 mm DES, which was deployed in the mid-distal RCA. Final Angiography showed excellent result.


Case Summary
Anchor balloon support techniques offer additional support by inflating a balloon in a proximal side branch to optimize guiding catheter stability, alignment and also improve support for device delivery. This case highlights the simple practical approach for achieving optimal PCI outcomes.